Congenital anomalies of renal tract
Bifid collecting system :- Most frequent.
- Unilateral or bilateral.
- Incomplete; sometimes only pelvis is bifid , 10 %of population, (not significant)
- Complete; (1-2 % of population), two ureters may be separate down to their insertion into the bladder.
Upper moiety ureter inserts inferior and medial to its normal site, or ectopically to vagina or urethra leading to urine incontinence if beyond urethral sphincter, may associate with obstruction or uretrocele.
- Lower moiety ureter inserts into normal anatomical position, usually associated with reflux.

Renal agenesis :
- incidental finding.
- The opposite kidney shows compensatory hypertrophy.
- Can be diagnosed as absent kidney on ultrasound or CT.
- IVU will show a single kidney with active contrast excretion .

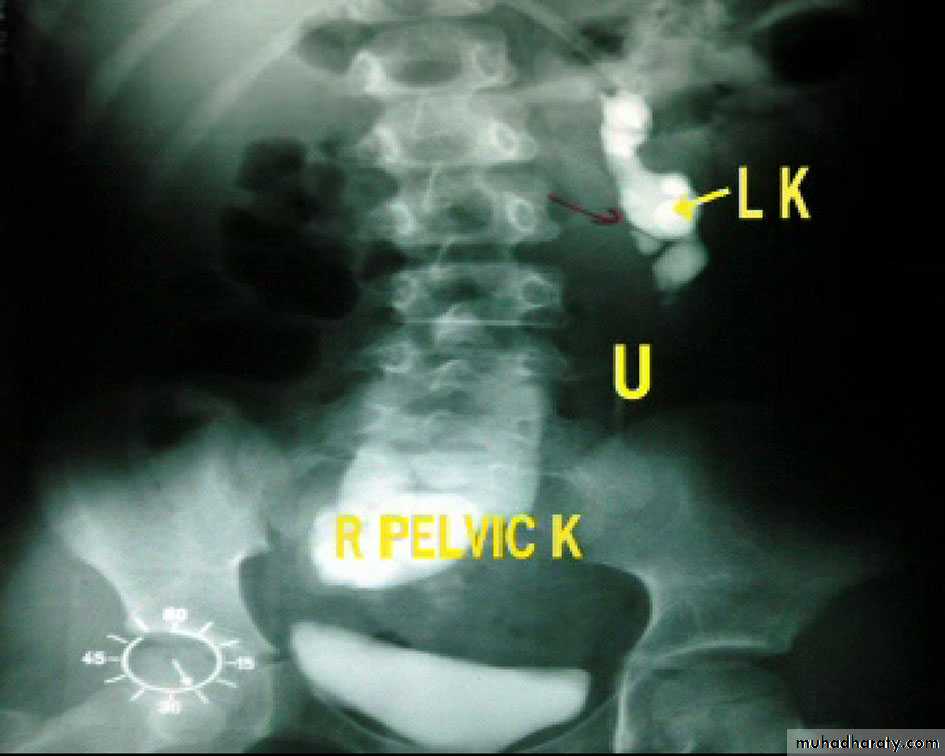
Ectopic kidney:
- Result from halted ascend of kidneys during fetal development
- Often are incidental findings during routine ultrasound, -usually located in the lower abdomen and rotated, -short ureter.
-Chronic pyelonephritis, calculi and hydronephrosis are more common .

Horse shoe kidney -Kidneys may fail to separate.
-Almost invariably the lower poles remain fused.
-The kidneys axes are more parallel to the spine and malrotated.
-Diagnosis can be made by plain x-ray in some cases.
-US, CT scan and MRI can better demonstrate the anatomy and morphology hence the diagnosis.
-May be an incidental finding.
-PUJ obstruction and calculi formation are common .
IVU shows
1. The kidneys at low position .
2.Close to the spine with long axis parallel to the spine .
3. Malrotation manifested by medially directed calyces.
4- The renal pelvis and ureters are anterior and lateral in position .

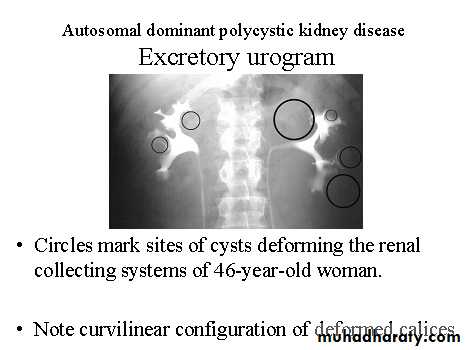
Poly cystic disease
Adult typePresent after the third decade of life , Familial.
Renal parenchyma is replaced by numerous cysts containing fluid , The cysts are of variable size ,
Clinically renal colic, loin mass , heamaturia and hypertension, Renal tissue interposed between the cysts after time dssimcted ended with renal failure
Almost bilateral.
IVU
Large kidney .
Lobulated out-line.
Distortion of pelvi- calyceal system depend on cyst size, number and position.
In advanced cases there is elongation and stretching of minor and major calyces ( spider leg).
In advanced cases IVU shows non-functioning kidney .
Infantile type :
Usually affect liver, spleen and pancreas , Incompatible with life .I.V.U.
- Bilateral Large kidney due to numerous small cysts (1-2 mm size ).- The out-line is not lobulated as in adult.
- I.V.U, may be normal.
- Nephrogram shows minute filling defects.

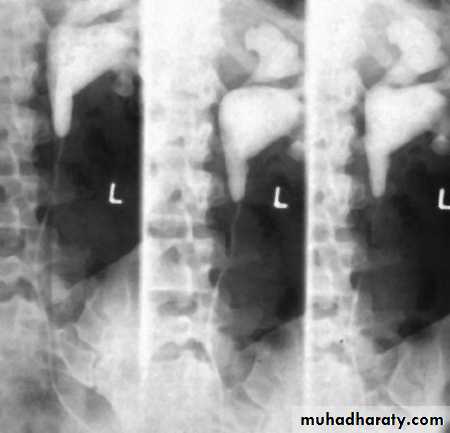
Infantile hydronephrosis ( PUJ OBSTRUCTION ):
IVU shows :
Marked dilatation of pelvis and may be extra-renal.
Calyceal dilatation is late and in advanced cases form foot shape PCS
The ureter is not seen and when it is seen looksnormal .
Delayed film with I.V. diuretic produce gross dilatation .

Congenital anomalies of ureter
Mega ureter :
Unilateral or bilateral dilatation of the ureter with no evidence of organic obstruction. o Cause – unknown
Retrocaval ureter :
The middle third of right ureter curve medially behind the IVC , then laterally to regain it’s normal position , this lead to obstruction of upper third of ureter.

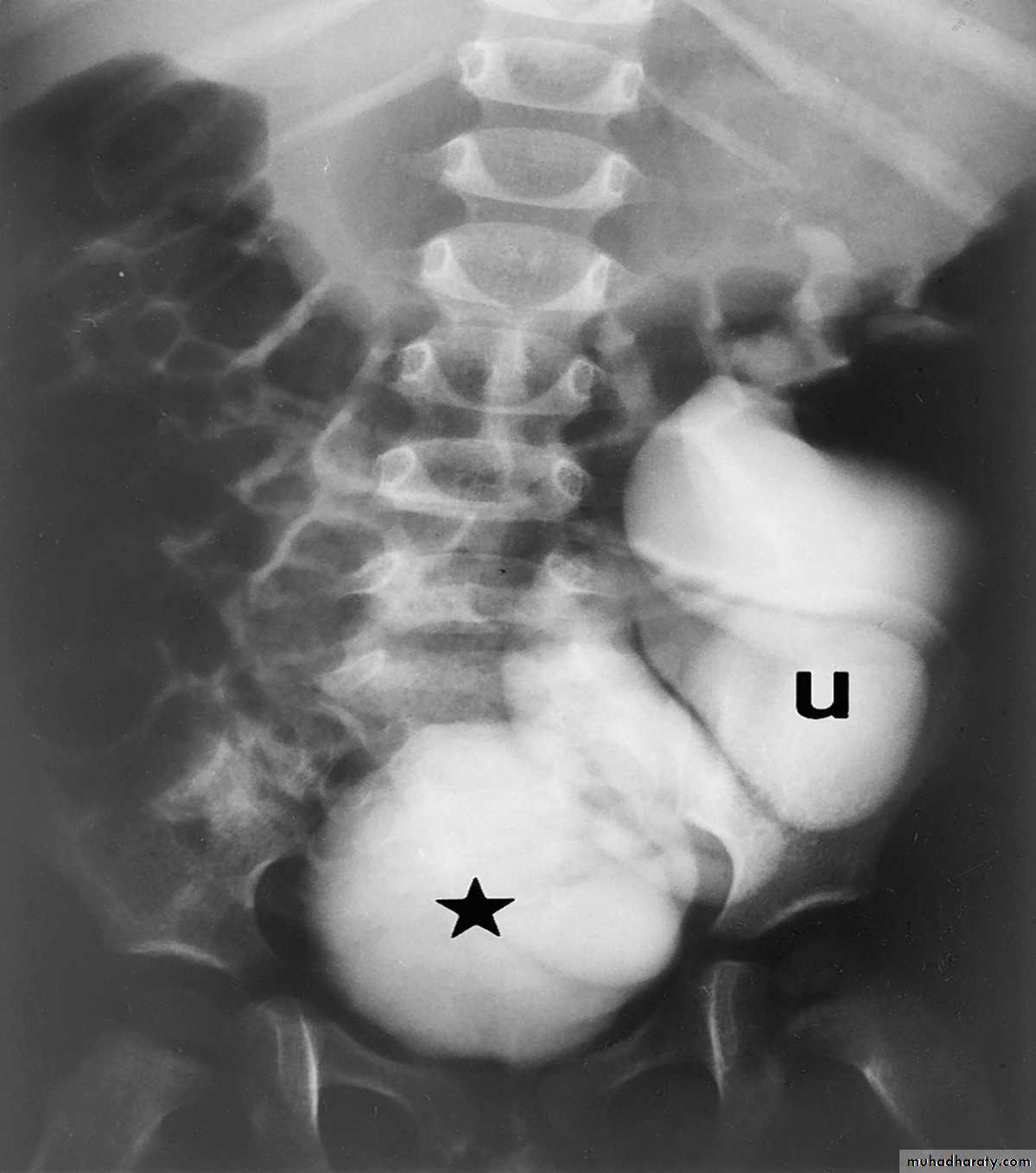
Ureterocele :
Congenital cystic dilatation of lower end of ureter ( intra-mural part) due to pin-hole meatus . May be simple or ectopic .simple : the orifice is in proper position of bladder ,
Ectopic >> in bladder neck , urethra , uterus & vagina .
IVU :
- There is rounded or elliptical dilatation of lower end of ureter with thin lineal filling defect around it , resembling (cobra head appearance),
- Proximal dilatation of rest of ureter .
- In advanced cases hydronephrosis .
- In obstructed ureterocele , filling defect in the bladder

Ectopia vesica :
bladder located at low position & plain x-ray shows separation of symphysis pubis .

Review