
1
Fifth stage
Neuro-Surgery
Lec-1
د
.
عبدالرحمن
2/5/2016
Neurosurgical Investigations
Neurosurgical Investigations
1. Cerebrospinal fluid investigation:
2. Radiological investigations:
Plain X-rays
CT scan
MRI
Radioisotope studies.
Cranial and Spinal Angiography.
Myelography
3. Electroencephalography (EEG).
4. Nerve conduction Studies/Electromyography (EMG).
Cerebrospinal fluid(CSF) investigation:
CSF can be obtained by:
• Lumbar puncture.
• Cisternal puncture.
• Cannulation of the lateral ventricle.
2
Lumbar Puncture Indications
1. Meningitis.
2. Subarachnoid haemorrhage.
3. Neurological diseases such as Multiple Sclerosis.
4. Cytological examination for neoplastic disease.
5. Radiological imaging (e.g. myelography) or radio-isotope investigations.
6. Measurement of intracranial pressure.
Measurement of intracranial pressure
Contraindications to Lumbar Puncture
1. Raised intracranial pressure.
2. Papilloedema .
3. Local infection.
Complications of lumbar puncture
1. Progression of brain herniation
2. Progression of spinal cord compression
3. Injury to the neural structures
4. Headache: low CSF pressure.
5. Backache
6. Infection—local and meningitis
7. Implantation of epidermoid tumour (rare).
3
Radiological investigations
1. Plain X-rays
2. CT scan
3. MRI
4. Radioisotope Studies.
5. Cranial and Spinal Angiography.
6. Myelography
I. Plain X-ray
A. Skull X-ray:
B. Plain X-rays of the spine:
a. X-rays of cervical spines:
b. X-ray of thoracic (dorsal) spines:
c. X-ray of the lumbosacral spines:
Skull X-ray
The major abnormalities to look for on a skull X-ray are:
1. Fractures
2. Hyperostosis, e.g. meningioma.
3. Bone erosion due to skull vault tumours.
4. Midline shift of the pineal gland—from space occupying lesion.
5. Abnormal calcification, e.g. tumours such as meningioma, oligodendroglioma,
craniopharyngioma or calcified wall of an aneurysm.
6. Signs of long-standing raised intracranial pressure— erosion of the dorsum sellae and
‘copper beating’ of the skull vault.
Plain X-rays of the spine
Particular note should be taken of:
1. Vertebral alignment.
2. Presence of degenerative disease with narrowing of the neural foramina and spinal
canal.
4
3. Evidence of metastatic tumour with erosion or sclerosis of the vertebral body, pedicles
or lamina.
4. Enlargement of a neural foramen indicating a spinal schwannoma.
5. Congenital abnormalities such as spina bifida.
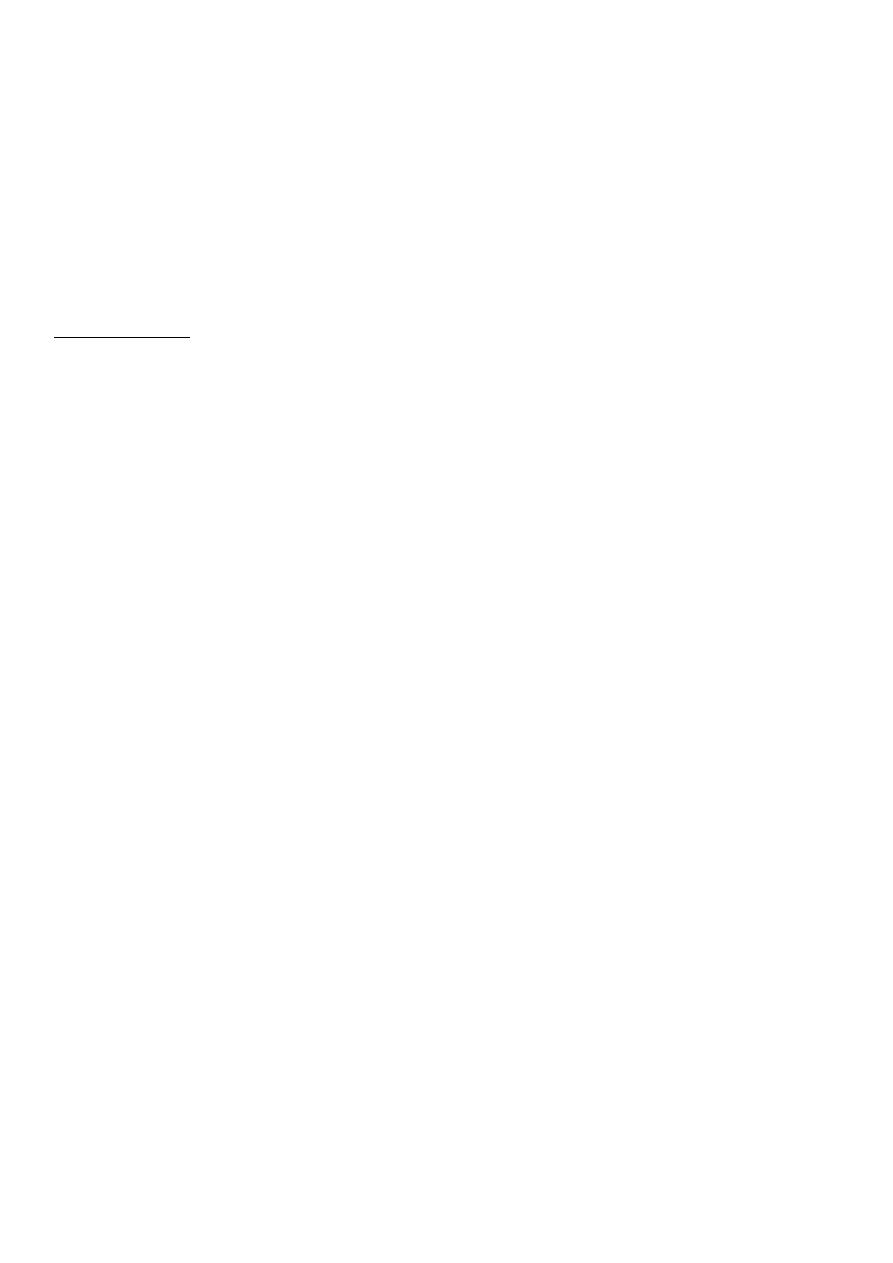
II. Computed Tomography (CT) Scan
Indications for Computed Tomography in Neurosurgery:
A. Cranial CT:
1. Diagnosis of acute neurosurgical lesions in the head and spine, including:
a. Skull and spinal fractures.
b. Intracranial hemorrhage: like extradural haematoma,subdural haematoma,
intracerebral haematoma.
2. Oedema: brain oedema whether due to trauma or other cause.
3. Mass lesions: mainly brain mass lesions like tumours and brain abscess.
4. Hydrocephalus
5. Stroke: differentiate between infarction and intracranial haemorrhage.

5
Spinal CT:
1. Lumbar and cervical disc prolapse.
2. Lumbar and cervical canal stenosis.
3. Spinal trauma
4. Spinal dysraphism.
Indications for Magnetic Resonance Imaging
1. Intracranial tumours.
2. CNS infection—cerebral abscess, herpes simplex encephalitis.
3. Arteriovenous malformations.
4. Venous sinus thrombosis.
5. Craniospinal abnormalities such as the Chiari malformation.
6. Syringomyelia.
7. Spinal tumours.
8. Disc prolapse (including cervical, lumbar and dorsal disc prolapse).
9. Spinal canal stenosis (lumbar or cervical stenosis) and cervical myelopathy.
CT is better than MRI:
1. Diagnoses of bone related pathologies like fractures and bone tumours.
2. Less time is needed to perform CT than MRI (few minutes) so CT is better in irritable
patients and critically ill patients.
MRI is better than CT:
1. In diagnoses of diseases related to soft tissues:
Posterior fossa tumours (cerebellar and brain stem tumours).
Spinal cord pathology (compression and tumours), and one can do myelography with
non invasive method (no need for lumbar puncture).
Infarction can be diagnosed as early as few hours whereas CT needs 48 hours to
diagnose it.
2. No ionizing radiation.

6
3. No bone artifact so that lesions around the skull base are clearly identified.
4. High resolution.
Contraindications to MRI
1. Intracranial clips.
2. Metallic foreign bodies anywhere in the body like plating and screwing, shells.
3. Pacemaker.
4. Cochlear implants.
5. Conditions requiring close monitoring of the patients (long time).
6. Claustrophobia.
7. Gross obesity( can not enter inside the tunnel).
8. Uncontrolled movement disorders (Parkinson’s disease).
9. Respiratory disease that require assisted ventilation or carry risk of apnoea (although
now there is MRI-compatible machines).
Radioisotope Studies
These include the new sophisticated techniques using radioisotopes, such as single photon
emission computerized tomography (SPECT) or positron emission tomography (PET): are
used to measure cerebral blood flow or cerebral metabolism.
These are used for:
1. Both techniques have been used for the investigation of epilepsy.
2. Study the biological activity of brain tumours, especially gliomas, in order to
differentiate low-grade tumours from high-grade and post-radiation necrosis from
recurrent tumour.
Cranial and Spinal Angiography:
Main indications in neurosurgery:
1. Investigation of cerebral ischaemia due to carotid artery disease and intracranial
atheroma.
2. Investigation of subarachnoid haemorrhage, e.g. cerebral aneurysm, arteriovenous
malformation.

7
3. Investigation of venous sinus thrombosis.
4. Preoperative embolization of meningioma.
Myelography
Complications of Myelography: which are now very uncommon, include:
1. Epileptic seizures.
2. Systemic reactions to the contrast medium .
3. The risks of the lumbar puncture itself.
The major indications for myelography were:
1. Disc prolapse (cervical and lumbar).
2. Spinal canal stenosis (cervical and lumbar).
3. Spinal tumours.
Electroencephalography(EEG)
The major indications for EEG recordings in neurological practice are:
1. Suspicion of epilepsy in a new patient.
2. Assessment of epilepsy in a patient with recurrent seizures.
3. Assessment of the risk of epilepsy in a patient who has undergone intracranial
surgery or following a severe head injury.
4. As an aid in the diagnosis of herpes simplex encephalitis and Creutzfeldt–Jakob
disease.
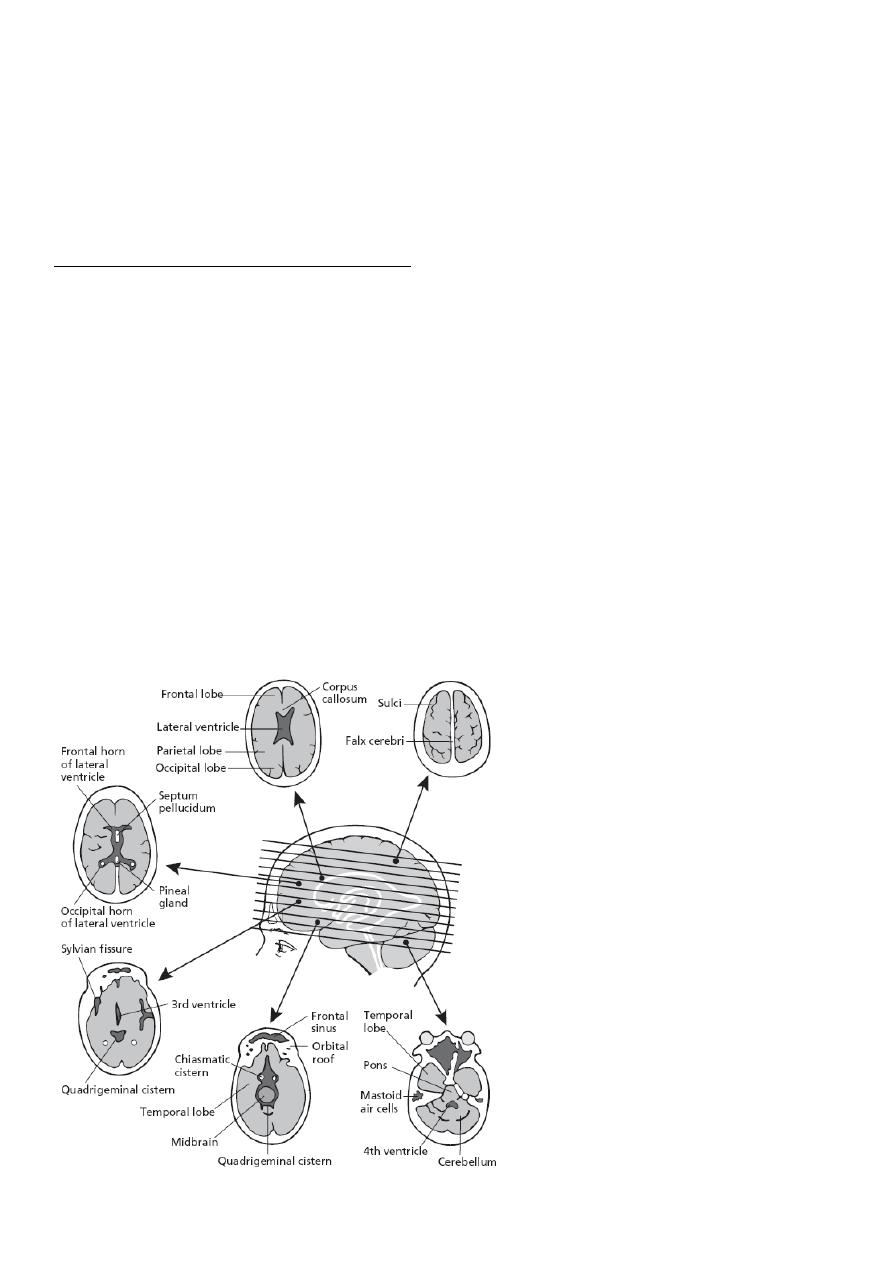
Nerve conduction studies/ Electromyography(EMG)
The Indications for these studies include:
1. Peripheral nerve injuries.
2. Peripheral nerve entrapment.
3. Brachial plexus injury.
4. Neuropathy.
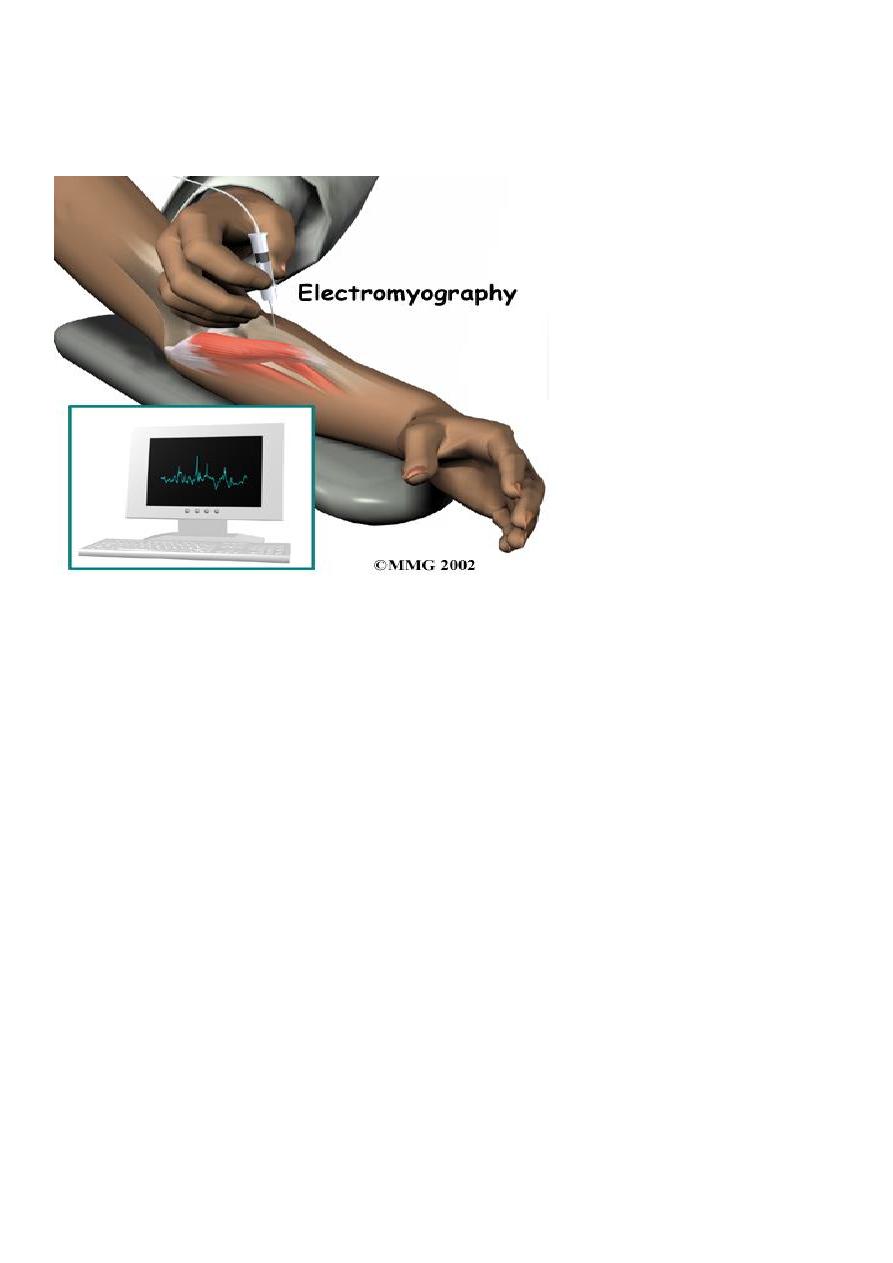
8
5. Myopathy (studies are normal).
6. Muscular dystrophy (studies are normal).