1
Forth stage
Obstetric
Lec-9
.د
ا
سماء
1/1/2016
Antepartum Hemorrhage
Antepartum haemorrhage: is bleeding from the the placental site from 24 week
gesation and before delivery of the fetus.
Bloody show ( Slight vaginal bleeding ) is common during active labor due to
effacement and dilatation of the cervix, with tearing of small veins.
Causes of antepartum haemorrhage:
Common:
Placenta previa..
Abruptio placentae
Uncommon:
Uterine rupture
Fetal (chorionic) vessels rupture.
Cervical or vaginal laceration.
Cervical or vaginal lesions.
Congenital bleeding disorders.
Placenta previa:
Incidence of placenta previa is 0.5% in all pregnancies.
Bleeding from a placenta previa account for about 20% of
cases of antepartum haemorrhage.
Presentation:
70% present with painless vaginal bleeding in the third
trimester.
20 % have uterine contraction.
10% diagnosed incidentally by US.
Predisposing risk factors
Factors associated with higher incidence of placenta previa:
Multiparity.
Increasing maternal age.
Prior placenta previa have 4-8% risk of placenta previa in subsequent pregnancy.
Multiple gestation
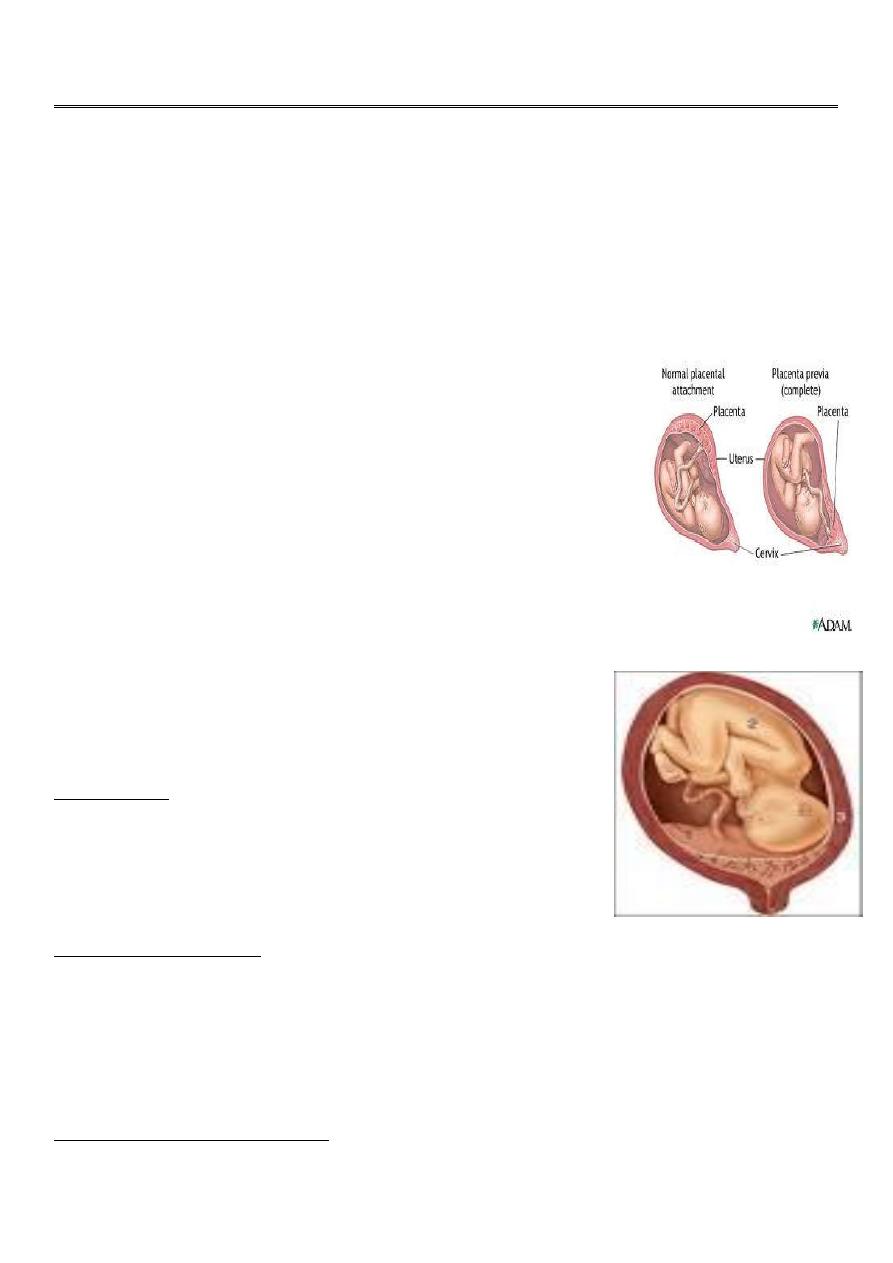
Classification of placenta previa:
Placentra previa is classified according to the relation ship of the placenta to the internal os
into:

2
Grade I :Marginal placenta previa : the edge of the placenta Is at the margin of the
internal os.
Grade II : the placenta is covering the cervix when it’s closed
Grade III :Major degree :Total placenta previa: internal os is covered completely by the
placenta
Grade IV :Major degree :central placenta previa
Partial placenta previa: internal os is partially covered by the placenta.
Low lying placenta: the placenta is attached to the lower uterine segment 2 cm from
the internal os.
Clinical presentation:
The most common characteristics :
Painless vaginal haemorrhage after second trimester or because for abortion .
Bleeding may occur without warning and without pain in a women who have
uneventful prenatal coarse , fortunately the initial bleeding is rarely so profuse to be
fatal , stop spontaneously to recur .In patient with placenta near the cervix bleeding
may not occur until the onset of labor.
The mean gestational age at the onset of labor is 30 weeks.
1/3 present before 30 weeks.
P.p. Most exclusively now diagnosed today by ultrasonography ,4-6% of patients have
some features of placenta previa on US before 20 weeks ,90% are resolved to normal
placentation by the third trimester . in case of complete placenta previa 10% resolved
by the third trimester.
Examination finding in placenta previa
During examination the abdomen is soft not tender uterine contraction may be
positive.
Uterus may be larger than date .
there may be malpresentation as breech or transverse lie or non engaged cephalic
presentation .
Fetal heart is positive and usually not affected by the initial blood loss.
Clinical diagnosis can be firmly established by finger examination feeling the placenta
near the internal os which should never be permissible unless the women is in the

3
operating theater with all preparation for immediate C.S. and unless delivery is
planned and when no facility for immediate US is not available.
Placental localization by US is the simplest ,precise and safest method for localization
of the placenta .
Trasnabdominal sonography has an accuracy of 95% for placenta previa detection
false positive result may be due to bladder distention so the scan should be repeated
after emptying of the bladder.
False negative in case of the placenta is implanted posteriorly and the fetal vertex is
low and the placenta is low and obscured and the diagnosis is missed
Transvaginal sonography is accurately diagnose all case of placenta previa but there is
risk of bleeding.
Preterm patient with placenta previa:
No vaginal bleeding require close observation with blood is prepared and facility for
immediate transport to hospital if bleeding occurs.
In properly selected patient there is no difference between inpatient and outpatient
treatment.
If mild to moderate vaginal bleeding conservative management inform of correction of
anemia , corticosteroid therapy
If sever and persistent vaginal bleeding and any bleeding after 36 week emergency
delivery is indicated .
Patient with no vaginal bleeding should be delivered at term (38 week).
Mode of delivery
Practically Caesarean section is indicated in all cases of placenta previa
Patient with placenta previa are liable for intraoperative and post partum haemorrhage
because of :
Placental bed at lower segment with poor uterine contraction.
Wide bed of placenta because of less blood supply.
Risk of placenta accreta (anterior placenta previa overlying previous uterine scar).
DIC.
Measures to control intraoperative bleeding in placenta previa cases:
Oxytocic drugs/hot packs/uterine packing.
Oversewing placental bed in placenta accreta.

4
Ligation of vessels(uterine and internal iliac )
Hysterectomy indicated as life saving and in patients completed their family.
Abruptio Placentae
Bleeding from a normally situated placenta due to it’s premature separation ,it could
be partial or complete,
Abruptio placentae denotes a sudden accident (clinical characteristics of this condition)
so referred to as accidental haemorrhage.
Types of abruptio placentae
-Revealed haemorrhage (external )When the blood from the placenta insinuate itself
between the membrane and the uterus then escape through the cervix.
-concealed haemorrhage (internal) : less often when the blood doesn’t escapes
externally but retained inside in between the detached placenta and uterus ,this type
carries greater hazards because the amount of bleeding is not properly appreciated
and because the possibility of disseminated intravascular coagulation.
Bleeding in placental abruption is almost always maternal in origin, with evidence of
fetomaternal haemorrhage in 20% of cases.
Incidence :1/200 deliveries .
Risk factors:
.Increased age and parity.
..Preeclampsia.
…Chronic hypertention.
….Preterm rupture of membrane.
…..Cigarette smoking.
……Thrombocytopenia.
…….Cocaine use.
……..Prior abruption.
………External trauma.
……….Uterine leiomyoma.
Clinical diagnosis:
Clinical picture vary considerably there might be Profuse bleeding with mild separation with
no fetal compromise or no external bleeding with complete separation of placenta and fetal
death.
Diagnosis of placental abruption is certain if the patient presented with painful Vaginal
bleeding associated with uterine tenderness , hyperactivity and increased tone .
Fetus is cephalic may be in distress or decreased fetal movement or even fetal death.
Diagnosis of placental abruption is initially clinical US detect 2% of abruption ,despite initial
US examination is required to exclude cases where placenta previa coexist with abruption.

5
Complication:
Shock : sometimes shock is out of proportion to the amount of blood loss.
Fetal distress in 60% and fetal death in 15%
Consumptive coagulopathy .placental abrption is the most common cause of DIC in
occurs in about 20% of cases especially in cases where abruption is massive or fetal
death has occurred.
Renal failure.
Couvelaire uterus : extravasation of blood into the uterine musculature , diagnosed
during laparotomy , rarly it cause sever post partum haemorrhage by interfering with
uterine contraction to indicate hysterectomy.
Treatment:
our aim is resuscitation with blood and crystalloids and prompt delivery to the mother to
control haemorrhage.
And the management will vary depending upon gestational age and the status of the
mother and the fetus.
If the baby is viable:
Expectant management in preterm labor with mild vaginal bleeding: delaying delivery till
term if the bleeding is mild and not in labor ,if sever vaginal bleeding and in labor delivery is
VD if no delay . if sever vaginal bleeding and not in labor delivery is by C.S. because lack of
omnious deceleration does not guarantee the safety of intrauterine environment for any
period of time , any time placental separation can be caused by uterine contraction with
rapid fetal compromise.
Fetal compromise in placental abruption can be caused by :
placental separation.
maternal haemorrhage
fetal haemorrhage
uterine hypertonus
If the baby is dead: vaginal delivery is preferred unless the haemorrhage is so brisk that
cannot replaced by blood transfusion or there is other obstetric indication for caesarean
delivery . although in patient with DIC there is risk of brisk bleeding from the uterine and
abdominal wound because of serious coagulation defect ( not placental site bleeding as it’
controlled by uterine contraction).