Malpresentation and malposition of fetus
obstetrics and gynaecology department 2015Malpresentation :any fetal presentation other then vertex including :breech, shoulder, face ,brow ,and compound presentation.
Cosequences:
Presenting part, ill-fittingUterine Contractions, poor
Membranes, rupture early- cord prolapse
Labour, difficult, long, obstructed
Birth trauma
Operative intervention
Increased perinatal and maternal mortality and morbidity
Fetal malformationIntrauterine fetal death
Cord proplase
Birth trauma,
Birth asphysixa
Infection, fetus, neonate and mother
Uterine rupture
Thromboembolism in the mother.
For optimal result:
Early diagnosis,
Planned delivery
Experienced staff
Well equipped hospital
Cross match 2 unit
Adequate hydration
Monitor in Labour
Pain relief
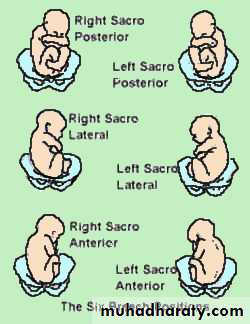
Breech presentation
Breech presentation :occurs when the fetal buttocks or lower extremities present into the maternal pelvis.
Breech presentation occurs in 3-4% of all deliveries.
The occurrence of breech presentation decreases with advancing gestational age. Breech presentation occurs in 25% of births that occur before 28 weeks’ gestation, in 7% of births that occur at 32 weeks, and 1-3% of births that occur at term. . Perinatal mortality is increased 2- to 4-fold with breech presentation, regardless of the mode of delivery. Deaths most often are associated with malformations, prematurity, and intrauterine fetal demise.Predisposing factor
prematurity,is major cause about 20 % are of low birth weight.uterine abnormalities (malformations, fibroids).
fetal abnormalities (CNS malformations, neck masses, aneuploidy).
multiple gestations.
AF abnormality.
Abnormal placentation.
Contracted pelvis.
Types of breech presentation
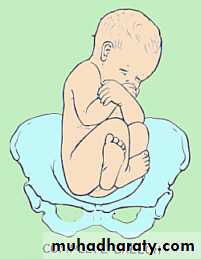
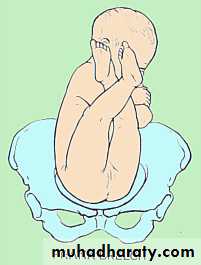
Frank breech (65%) - Hips flexed, knees extended
Complete breech (25%) - Hips flexed, knees flexed
Footling or incomplete (10%) - One or both hips extended, foot presenting

diagnosis
Diagnosis of breech:Palpations and ballottement(leopold man.)
Pelvic exam.
Ultrasound
X-ray studies.
Diagnose underlying cause.
management
No action until 37-38 weeks of gestation
Reason???
Exclude
fetal anomaliesPlacenta previae
Multiple pregnancy
Offer external cephalic version (ECV)
Should not be attempted if there are risksRisks??
Prerequisites??
Drawbacks of ECV
Management of breech presentation
Antepartum management.Delivery management.
Vaginal breech delivery.
Antepartum management
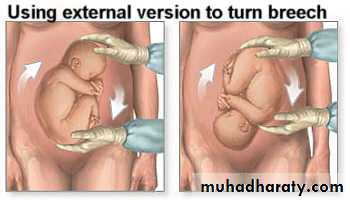
ECV
Is a procedure to turn the breech fetus to a vertex presentation through external uterine manipulation ,in hospital ,under US guidance.
ECV may be considered at breech presentation at term before the onset of labour.
Vertion is not carried before 36-37 weeks(tendency for spontaneous reversion)
Carried in hospital equipped for emergency CS because of the risk of placental abruption ,or cord compression(fasting patient with I,v line)
Contraindication:
Evidence of uteroplacental insufficiency.Placenta previa.
Non reassuring fetal monitoring.
Hypertension.
IUGR or oligohyraminos.
History of previous uterine surgery.
Immediate success rate is 35%-76%.
Reversion to breech at term after ECV is2%.ECV decrease the rate of CS ,but perinatal mortality is not affected.
Mode of delivery:
Assisted Vaginal Breech deliveryElective Caesarean Section (CS)
Emergency CS
Crieteria for VD or CS
VD
Frank
GA>34w
FW=2500-3500gr
Adequate pelvis
Flexed head
If Nonviable fetus
No indication CS
Good progress labor
Willing of the patient
Experienced staff
CS
FW<2500or> 3500gr
Footling
Small pelvis
Deflexed head
Arrest of labor
GA24-34w
Elderly PG
Infertility or poor history
Fetal distress
PIH,PE
APH
Previous CS
Pelvic tumor.
• Three types of vaginal breech deliveries:
• Spontaneous breech delivery
• Assisted breech delivery
• Total breech extraction
Assisted vaginal breech delivry
As breech delivery can occur in any place when immediate CS is not available ,practice of deliver skill is important to every practice in OB.Ensure full dilatation of cervix
Thick meconium passage is common as the breech is squeezed through the birth canal. This usually is not associated with meconium aspiration because the meconium passes out of the vagina and does not mix with the amniotic fluid.
Ritgen maneuver is applied to take pressure off the perineum during vaginal delivery. Episiotomies often are cut for assisted vaginal breech deliveries, even in multiparous women, to prevent soft-tissue dystocia.

No downward or outward traction is applied to the fetus until the umbilicus has been reached.

With a towel wrapped around the fetal hips, gentle downward and outward traction is applied in conjunction with maternal expulsive efforts until the scapula is reached. An assistant should be applying gentle fundal pressure to keep the fetal head flexed.

After the scapula is reached, the fetus should be rotated 90° in order to delivery the anterior arm.

The anterior arm is followed to the elbow, and the arm is swept out of the vagina.

The fetus is rotated 180°, and the contralateral arm is delivered in a similar manner as the first. The infant is then rotated 90° to the back-up position in preparation for delivery of the head.

The fetal head is maintained in a flexed position by using the Mauriceau-Smellie-Veit maneuver, which is performed by placing the index and middle fingers over the maxillary prominence on either side of the nose. The fetal body is supported in a neutral position with care to not overextend the neck.

Piper forceps application: Pipers are specialized forceps used only for the aftercoming head of a breech presentation. They are used to keep the head flexed during extraction of the fetal head. An assistant is needed to hold the infant while the operator gets on one knee to apply the forceps from below.

Assisted vaginal breech delivery: Low 1-minute Apgar scores are not uncommon after a vaginal breech delivery. A pediatrician should be present for the delivery in the event that neonatal resuscitation is needed.

Risk of breech vaginal delivery
Lower Apgar scorsAn entrapped head
Nuchal arms
Cervical spine injury
Cord prolapse
Face presentation
1:300
Full extension of the head
Presenting part: Face
Denominator: Omentum/Chin
Diameter; Subomento bregmatic 9.5cm
Presentation, Mento anterior– Vaginal delivery
Mento posterior- Ceasaeran
Causes:
AnenecephalyPrematurity
Multifetal pregnancy
Polyhydramnious
Neck tumours
Sternomastoid spasm
Multiparty
Diagnosis:
AbdominalVaginal
Brow presentation
1:800, 1:2000 deliveries
The area between the orbital ridge and the anterior fontenalle
Most unfavourable of all presentation
Transient presentation;
Full flexion—Occiput
Full extension---Face
Diagnosis is during labour.
