د.هالة عبدالغني الراوي
المرحلة الرابعة
2015
-
-2016
Objectives:
To be familiar with different fetalmalpresentation,their management & possible
comlication
FETAL MALPRESENTATION
Refers to fetal presenting part other than vertex and includes breech,
transverse, face and brow.
Malpresentation may be identified late in pregnancy or may not be discovered
until the initial assessment during labour.
FACE PRESENTATION
Incidence: 1:500 deliveries.
General causes for face presentation
:( complete extension of the fetal
head)
1. Congenital fetal anomalies such as anencephaly, thyroid tumour.
2. Multiple pregnancies.
3. Prematurity.
4. Less common associated factors include uterine abnormalities such as
bicornuate uterus, placenta praevia, pelvic tumors and polyhydramnios.
5. In the majority it is due to extension of the head in a normal fetus.
70% of cases reported to be multiparous.
Types of face presentation:
Mentoanterior face presentation (77%).
Mentoposterior face presentation.
50% remained undiagnosed until delivery is imminent.
CLINICAL FINDINGS:
Possibility of face presentation can be suspected on:
Abdominal examination: if the prominence of the head is palpable more
prominently at higher level on the opposite side of the fetal spine. In thin women
a deep groove may be palpable between the occipit and the back.
Vaginal examination: when the eye, nose, the mouth with the hard gum margins
and mandible are palpated.
Difficulties may be encountered in recognizing the presentation when the
membranes are intact especially when the presenting part is high or in the
presence of face oedema due to few hours of labour.
MANAGEMENT:
Ultrasound is advised to exclude fetal or pelvic abnormalities that preclude
vaginal delivery.
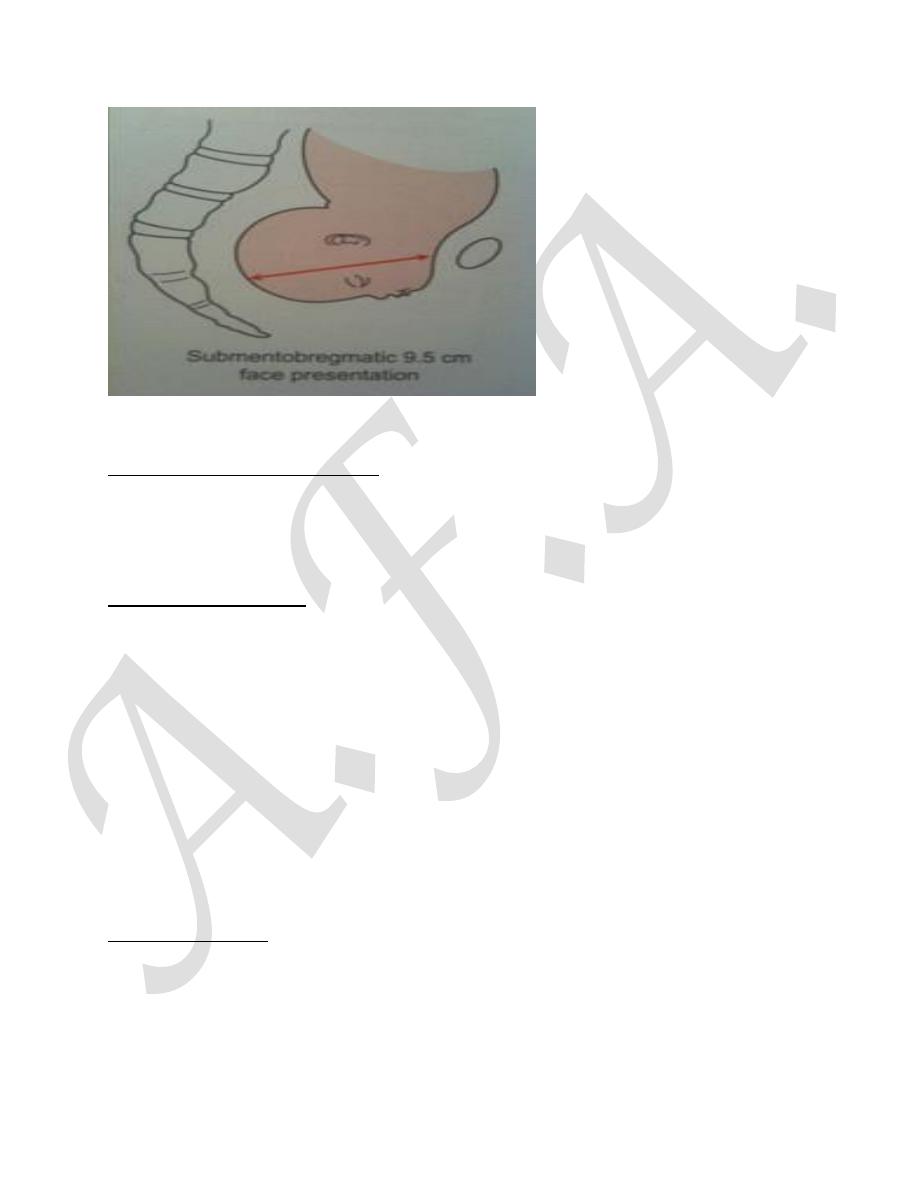
Mechanism of labor has some similarity to that of vertex presentation. face
presentation may apply themselves poorly to the cervix & the resulting progress
in labour may be poor. The transverse submento-bregmatic diameter (9.5cm)

enters the pelvis. In the vast majority it rotates forwards to be in the mento-
anterior position with the chin behind the symphysis pubis. Descend is possible
posteriorly in the pelvis when the position is mento-anterior because of large
space in the lateral sacral area. Once the face seen at the introitus the head may
be born by flexion with the chin emerging under the pubic arch followed by the
forehead over the perineum.
Episiotomy is advisable to avoid perineal trauma.
If the face rotates to a mento-posterior position although the diameters are the
same as mento-anterior, the lateral dimensions of the frontal bones are large and
do not permit descend behind the narrow retropubic arch and hence cesaerean
section is advisable, around 50% of mento-posterior will rotates to mento-
anterior position.
Even with favourable mento-lateral or anterior position failure of progress in the
1
st
stage indicates ceasarean section,oxytocin should not be used.
delay in the second stage is common. In late second stage of labour with the face
at the outlet in mento-anterior or lateral position outlet forceps delivery can be
carried out by skilled personal if spontaneous delivery is not forthcoming.
&ventous delivery is contraindicated.
Following delivery the fetal face is usually very oedematous and may be bruised.
This usually persists for several days and may cause feeding difficulties.
Risks of vaginal delivery:
1- Soft tissue trauma to the fetal face.
2- Perineal damage including anal sphincter injury to the mother.
3- Second stage emergency caesarean section.
BROW PRESENTATION
INCIDENCE: Rare, 1:2000 deliveries.
AETIOLOGY: The same as for face presentation and the prematurity associated
with 20% of cases.
In brow presentation the head is less extreme extended and presents to the pelvis
with the largest diameter (mento-vertical=13.5 cm).
CLINICAL FINDINGS:
Abdominal findings typically include large, high head as the mento-vertical
diameter is unlikely to engage. Vaginally the lower most part of the head
(forehead) is palpable but it is termed as brow because the orbital ridges and the
bridge of the nose are the most definable part of the presentation.
MANAGEMENT:
Ultrasound examination is essential to exclude fetal or pelvic abnormalities.
Many brow presentations in early labour are transient and either flexes into
vertex presentation or further extends into a face presentation and may result in
vaginal delivery. Persistence of brow presentation in labour at term necessitates
caesarean section.
In early labour time is allowed to see whether flexion or extension would take
place. Failure to progress in the next few hours in labour with the persistence of
brow presentation indicates caesarean section and not augmentation of labour
with oxytocin.
In extreme prematurity the fetus may descend as a brow and deliver as a brow or
may convert to a face or vertex after it reaches the pelvic floor. Although vaginal
delivery is possible in preterm fetuses there is a possibility of spinal cord damage
and caesarean section is preferred.

In cases of intrauterine death and in those of lethal malformations in the extreme
preterm period, labour may be allowed with good progress aiming for vaginal
delivery.
At term destructive operations and vaginal delivery may be possible for cases of
fetal death and lethal anomaly but caesarean section is still preferred to avoid
genital tract trauma in the hands of those who are not familiar with these
techniques.
Complications during labour:
1- Cord prolapse with membrane rupture.
2- Uterine rupture in neglected cases especially in multipara and grand multipara.
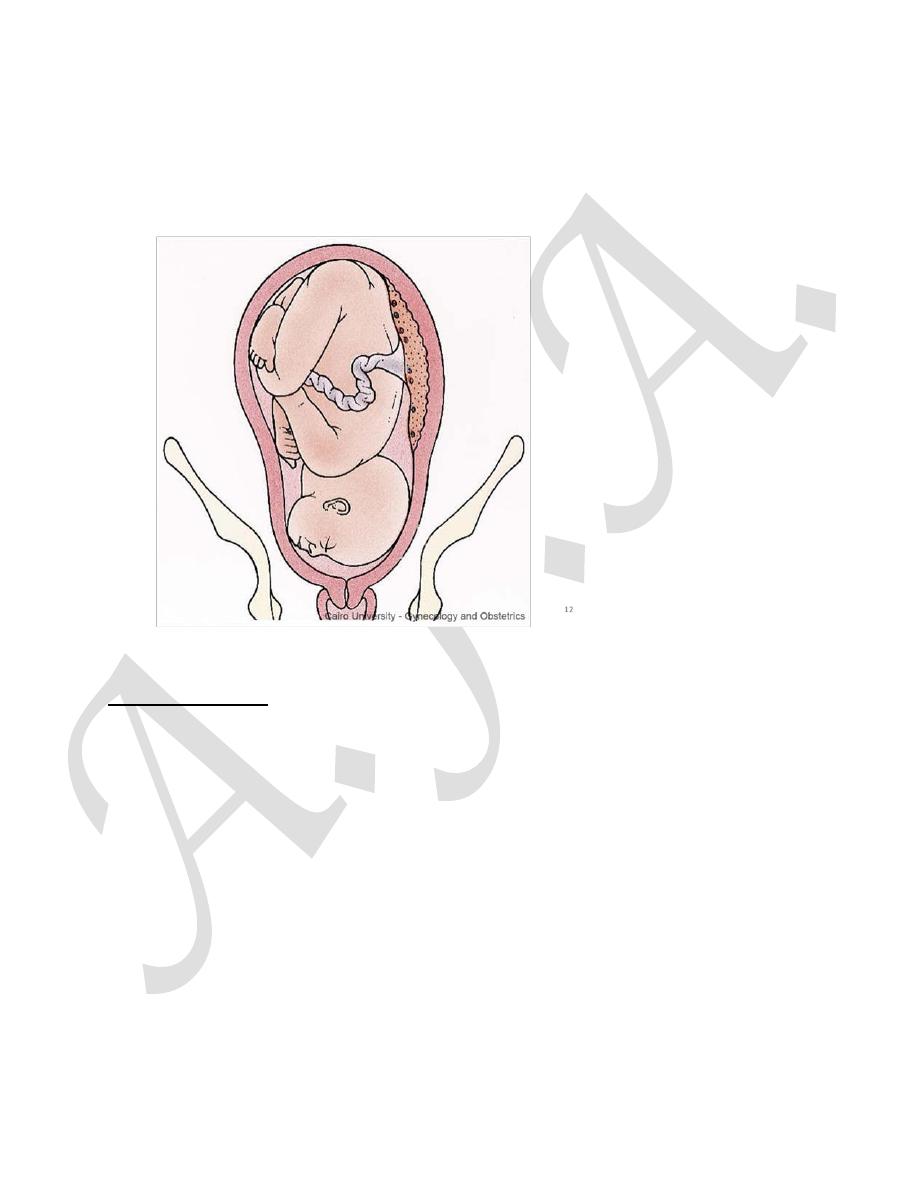
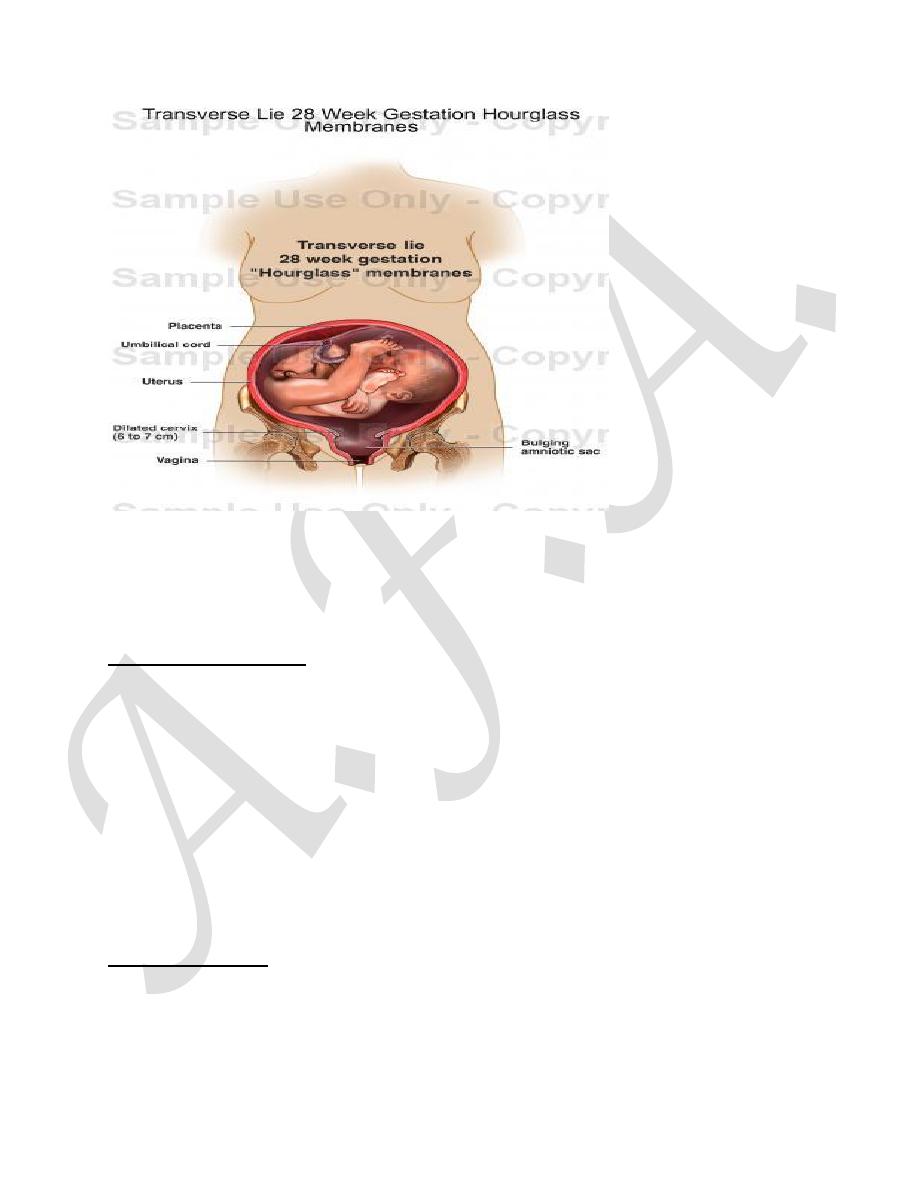
TRANSVERSE LIE
INCIDENCE: At term 1:300 pregnancies at term.
In transverse lie the fetus lies horizontally in the pelvis. The presenting part is
usually one of the shoulders (acromion process), an iliac crest, a hand or an
elbow.
AETIOLOGICAL FACTORS:
1- Multiparous women with singleton pregnancies without any cause due to the
laxity of the uterus.
2- Preterm.
3- Congenital fetal or uterine malformation.
4- Fibroids.
5- Placenta praevia.
6- Polyhydramnios.
CLINICAL FINDINGS:
Inability to locate a fetal pole in the pelvis on either abdominal or vaginal
examination should suggest a non longitudinal lie whether in the antenatal period
or during labour. the head is in one flank and the buttocks in the other.
-Vaginal examination—the pelvis is empty of presenting parts.
- Investigation: ultrasound scan confirms diagnosis.
Unstable lie
Is when the fetal presentation repeatedly changes beyond 37 weeks
gestation
.
MANAGEMENT:
Ultrasound examination should be used to confirm the lie, exclude fetal anomaly
and pelvic tumours and localize the placenta.
Management of transverse lie in pregnancy

1- Before 36 weeks, The position is usually self-curing.
2- Past 37 weeks in a multiparous patient, admission to hospital should be
advised, where ECV is attempted
3- Should the woman go to term with the fetus still in a transverse position,
management may be by either of the following:
stabilizing induction:
ECV(external cephalic version) is done in the labour ward.
The fetal head is held over the brim of the mother’s pelvis and high membrane
rupture is performed.
Amniotic fluid escapes and the head often sinks into the pelvis.
Labour follows in the normal fashion.
An elective Caesarean section:
this may be the safer line of treatment for the fetus since it cuts down the
risks of prolapsed cord during labour,
Management During labour
In early labour with the membranes intact, wait in anticipation of spontaneous
or assisted correction to longitudinal lie while making all the preparation for CS.
If the membranes rupture and the fetus still in the transverse lie, CS should be
performed to avoid injury to the fetus or the uterus. In cases where the diagnosis
is made late the fetus may be impacted in the transverse lie and save delivery
may be only possible by a CS with a midline vertical incision. It may be possible to
deliver the fetus through a lower segment transverse incision with acute uterine
relaxation using a short acting drug. Labour and spontaneous vaginal delivery is
possible in extreme preterm and macerated fetuses.
Complication of Transverse and Unstable lie:
• Cord or hand prolapse.
• Obstructed labour .
• Uterine rupture.
• Difficult intra operative delivery of the fetus.
• Birth trauma ( erbs pulsy).
• Postpartum haemorrhage.
CORD ACCIDENTS (CORD PRESENTATION AND CORD
PROLAPSE)
DEFINITION: Cord presentation is defined as the umbilical cord lying below the
fetus, but the membranes remaining intact. Cord prolapse occurs when the
membranes rupture and the cord descends through the cervix into the vagina.
INCIDENCE: Cord presentation or prolapse is 1:500 deliveries.
Risk factors:
1- Low birth weight (< 2.5kg).
2- Prematurity.
3- Breech presentation (especially footling breech).
4- All other malpresentations including shoulder presentation.
5- Second born twin.
6-polyhydramnios
7-placenta previa
8-large baby
9-pelvic tumours(e.g.fibroids in the lower segment)
10-narrow pelvis

The umbilical cord vein is compressed between the presenting part and the bony
pelvis, reducing or stopping the flow of oxygenated blood to the fetus leading to
acute fetal hypoxia. The drop in ambient temperature if the cord prolapses
beyond the introitus may cause cord vascular spasm leading to acute fetal
hypoxia also.
MANAGEMENT:
Vaginal examination will reveal the cord presentation or prolapse.
Care of cord prolapse:
1- Avoid feeling for pulsation; it increases the cord handling which may cause
spasm.
2- Assess the fetal viability by pinard, Doppler, CTG.
If the fetus is viable:
3- The cervix is fully dilated consider assisted vaginal delivery (Ventouse or
forceps) if easy vaginal delivery is anticipated.
4- If the cervix is fully dilated and the head is high or there are other factors
suggest difficulty encountered at vaginal delivery resort to C/S immediately.
5- If the cervix is not fully dilated with normal fetal heart urgent caesarean section
is required.
6- Whilst arranging for C/S, relieve pressure on the cord to allow oxygen to reach
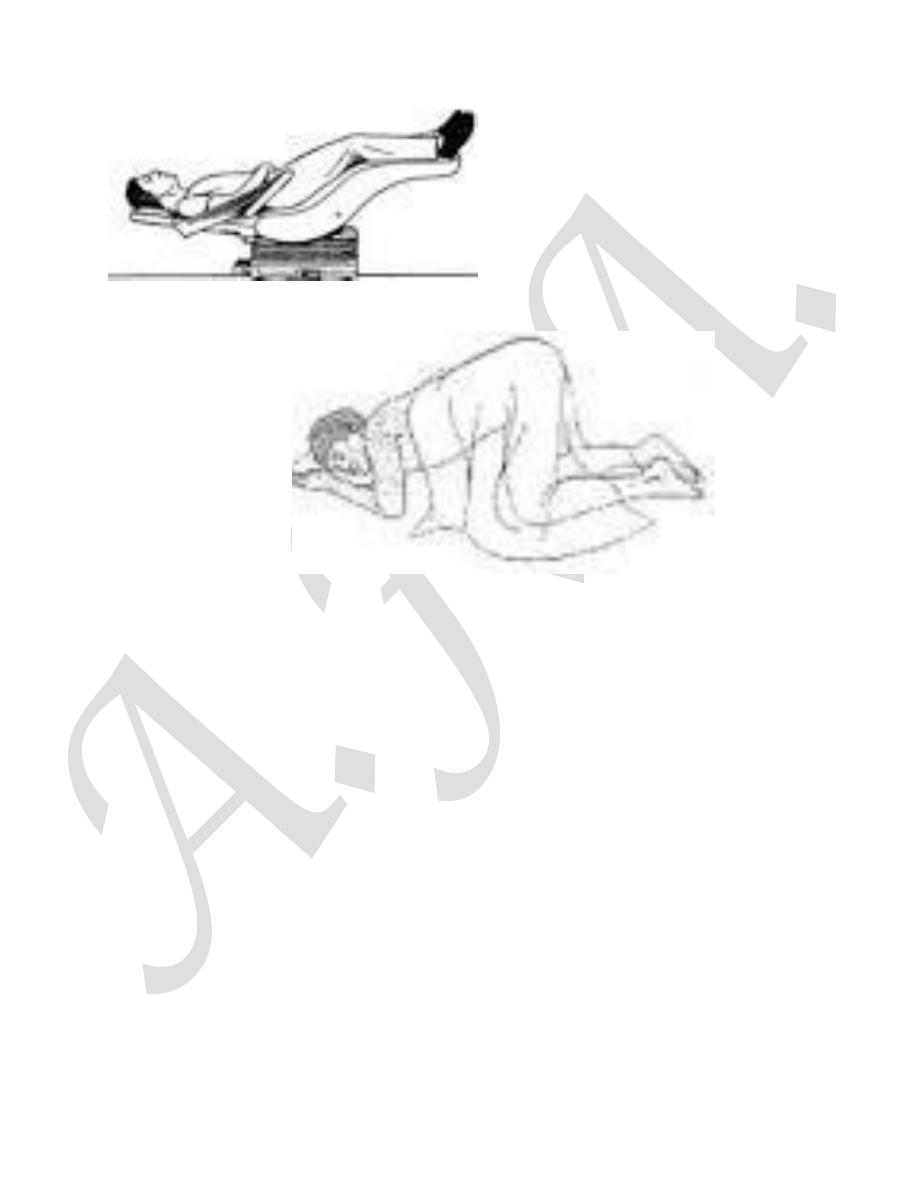
the fetus by the followings:
a- Knee-elbow position / left lateral with Trendelenberg position.
b- Manual elevation of the presenting part to relieve the pressure on the cord.
c- Catheterize and fill the bladder with 500 ml of normal saline then clamp the
catheter to displace the fetal presenting part upwards. Unclamp catheter and
drain the bladder before opening the abdomen.
If the fetus is not viable await spontaneous vaginal delivery unless there are
other indications for C/S.