4th stage
MedicineLec
د.عماد
5/4/2016
Pituitary gland
The pituitary is located at the base of the brain, in a small depression of the sphenoid bone (sella turcica).
Purpose: control the activity of many other endocrine glands “ Master gland”
Has two lobes, the anterior & posterior lobes.
Boundaries :-
Superiorly : optic chiasma
Inferiorly : sphenoidal sinuses
Lateral : cavernous sinuses ( contain 3rd , 4th and 6th cr. Nerves + internal carotid artery )
Structure :-
Composed of anterior and posterior lobes , connected to pituitary by infundibular stalk , portal vessels carry blood from hypothalamus to anterior lobe of pituitary nerve fibers to posterior lobes .
Physiology :-
Hormones secreted from anterior pituitary(controlled by substances produced in hypothalamus and released into portal blood flow down pit stalk)
LH,FSH
TSH
Prolactin
GH
ACTH
Hormones secreted from post pituitary (synthesized in hypothalamus and transported through nerve axon down to be released from pos pit gland
ADH (anti diuretic hormone ) 2. Oxytosin
Anatomy :-
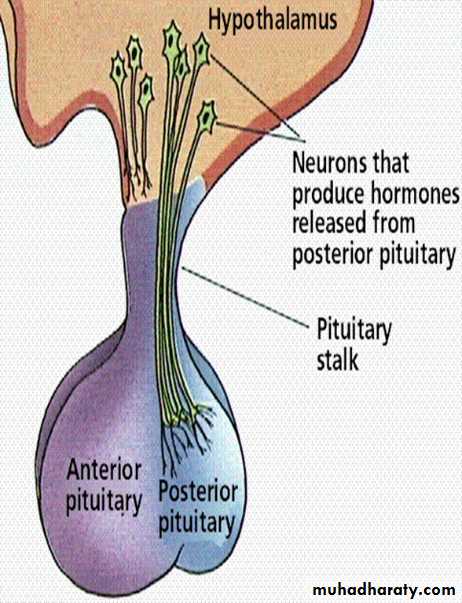
Anterior lobe: glandular tissue, accounts for 75% of total weight. Hormones in this lobe are controlled by regulating hormones from the hypothalmus (stimulate or inhibit)
Posterior: nerve tissue & contains axons that originate in the hypothalmus. Therefore this lobe does not produce hormones but stores those produced by the neurosecretory cells in the hypothalmus. Release of hormones is triggered by receptors in the hypothalmus.
Anterior Pituitary Secretes :
GH:stimulates growth of bone and muscle , promotes protein synthesis and fat metabolism.ACTH(Adrenocorticotropin ): stimulates adrenal gland cortex secretion of mineralcorticoids (aldosterone) & glucocorticoids (cortisol).
TSH: stimulates thyroid to increase secretion of thyroxine, its control is from regulating hormones in the hypothalmus
Prolactin:stimulates milk production from the breasts after childbirth to enable nursing. Oxytoxin from posterior lobe controls milk ejection.
FSH: promotes sperm production in men and stimulates the ovaries to enable ovulation in women. LH and FSH work together to cause normal function of the ovaries and testes.
LH: regulates testosterone in men and estrogen, progesterone in women.
Posterior Pituitary secrets :
Antidiuretic hormone or ADH - also called vasopressin, vasoconstricts arterioles to increase arterial pressure; increases water reabsorption in distal tubules.Oxytocin: stimulates uterus to contract at childbirth; stimulates mammary ducts to contract (milk ejection in lactation).
Presenting problems in hypothalamic and pituitary diseses
A-Hypopituitarism 1-anterior pituitary hormone deficiency
Combined deficiency of any of the ant pituitary hormones.Clinical presentation vary.
Most common cause is pituitary macroadenoma
Causes of ant pituitary hormone deficiency :
1.Structuralprimary pit tumor
Adenoma, carcinoma, Craniopharyngioma, Meningioma, Heamorrhage (apoplexy), Langerhans cell histocytosis, Arachnoid cyst, Secondary tumour (leukemia, lymphoma), Chordoma
2.Inflammatory / infiltrative
sarcoidosis, haemochromatosis, infections (pit abscess, TB, syphlis,encephalitis).
3.Congenital deficiencies
GnRh (kallmann’s syndrome), TRH, GHRH, CRH
4. Functional
chronic systemic illness, excessive excersise, anorexia nervosa5.Other
head injury, parasellar radiotherapy and surgery, post partum necrosis (Sheehan's syndrome)
Clinical assessment
1-Progressive loss of pit. functions in following consequences
- GH :
-Lethargy, muscle weakness, increased fat mass
-Gonadotrophines (LH,FSH) :
in male Loss of libido, gynecomastie, decrease shaving
in female oligomenorrhea or amenorrhea
absent pubic hair in both sexes with fine & wrinkled skin
chronic anemia
- ACTH (loss of cortisol, with maintenance of aldosteron )
hyponatremia and postural hypotension with normal K+
pallor due to lack of melanocyte stimulation by B-Lipotrophic hormone
-TSH (Secondary hypothyroidism)
apathy and cold intolerance
2. Acute presentation
* acute glucocorticoid deficiency ppt by infection or injury
* in secondary apoplexy.
Investigations :
ACTH deficiencyShort ACTH stimulation test Insulin tolerance test only if uncertainty in interpretation of short ACTH stimulation test (e.g. acute presentation)
LH/FSH deficiency
In the male, measure random serum testosterone, LH and FSH
In the pre-menopausal female, ask if menses are regular
In the post-menopausal female, measure random serum LH and FSH (which would normally be > 30 mU/L)
TSH deficiency
Measure random serum T4
Note that TSH is often detectable in secondary hypothyroidism, due to inactive TSH isoforms in the blood
Growth hormone deficiency
Only investigate if growth hormone replacement therapy is being contemplated
Measure immediately after exercise
Consider other stimulatory tests
2-posterior pituitary hormone deficiency :
Cranial diabetes insipidus
Only investigate if patient complains of polyuria/polydipsia, which may be masked by ACTH or TSH deficiency
Exclude other causes of polyuria with blood glucose, potassium and calcium measurements
Water deprivation test or 5% saline infusion test
Management :
A-Chronic hormone replacement therapy:1. Cortisol replacement (hydrocortisone )
2. Thyroid hormone replacement (thyroxin 100-150 microgram)
3. Sex hormone replacement (restore normal sexual function and prevent osteoporosis)
4. GH Replacment
- daily subcutaneous self injection of GH to children and adolescents before epiphysis fusion
- can be given in some adults
-monitoring by measurement of serum insulin like growth factor (IGF-1)
-Side effects Na retention with peripheral edema ad carpal- tunnul syndome
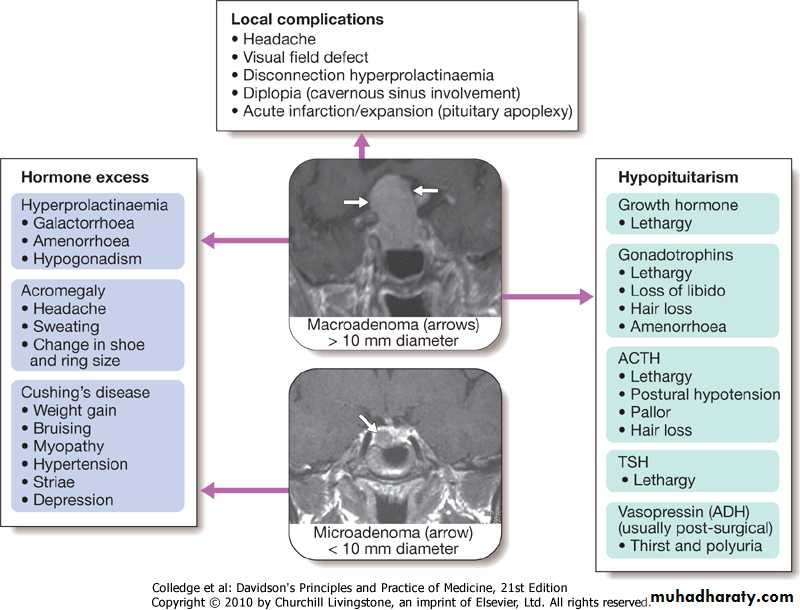
B- Identify hormone excess :
Hyperprolactinemia ,
Acromegaly ,
Cushing’s syndrome
PITUITARY TUMOUR :
Way of presentation:
Mass effect depending on size and location
- most intraseller tmors are macroadenoma
- majority of extrasellar tumors are craniophryngiomas
- most paraseller masses are meningiomas
Incidentally by CT or MRI
Clinical presentation :
1-Headache2-Visual field defect
*bitemporal hemianopia, or upper quadrianopia (optic chiasma compression)
* unilateral loss of acuity or scotoma (optic n compression due to supraseller extension of tumour)
*homonymous hemianopia (optic tract compresion)
3- Optic atrophy by fundoscopy
4- Diplopia and strabismus (compression on 3rd, 4th, and 6th cranial n due to lat extension to cavernous sinus)
5-Acute onset hypopituitarism due to apoplexy(bleeding into cystic lesion, or tumour infarct)
6-Non hemorrhagic infarction in a normal pit
)Obstetric hmg (Sheehan's syndrome
DM
Inc intracranial pressure
Investigations :
MRI or CT scan for suspected patients
Biopsy for definite diagnosis (at time of operation)
Management :
Treatment of associated hypopituitarism
Urgent management for visual pathway pressure (within 4 months)
*measure prolactin first if >5000 mU/L with suspicion of macroprolactinoma then trial of dopamine agonist surgery
Surgical approach
* Trans-sphenoidal approach via nostrils in most cases
* Trans-frontal via craniotomy for suprasellar t
* Repeat pit function tests 4-6 wk following surgery
* Repeat imaging after few months
External radiotherapy
*for radiosensitive tumours,
*avoid in emergency condition
*risk of hypopit in 50-70%
*impair cognitive functions, cause vascular changes, induce primary brain tumours
For nonfunctioning tumours
*repeated imaging