1
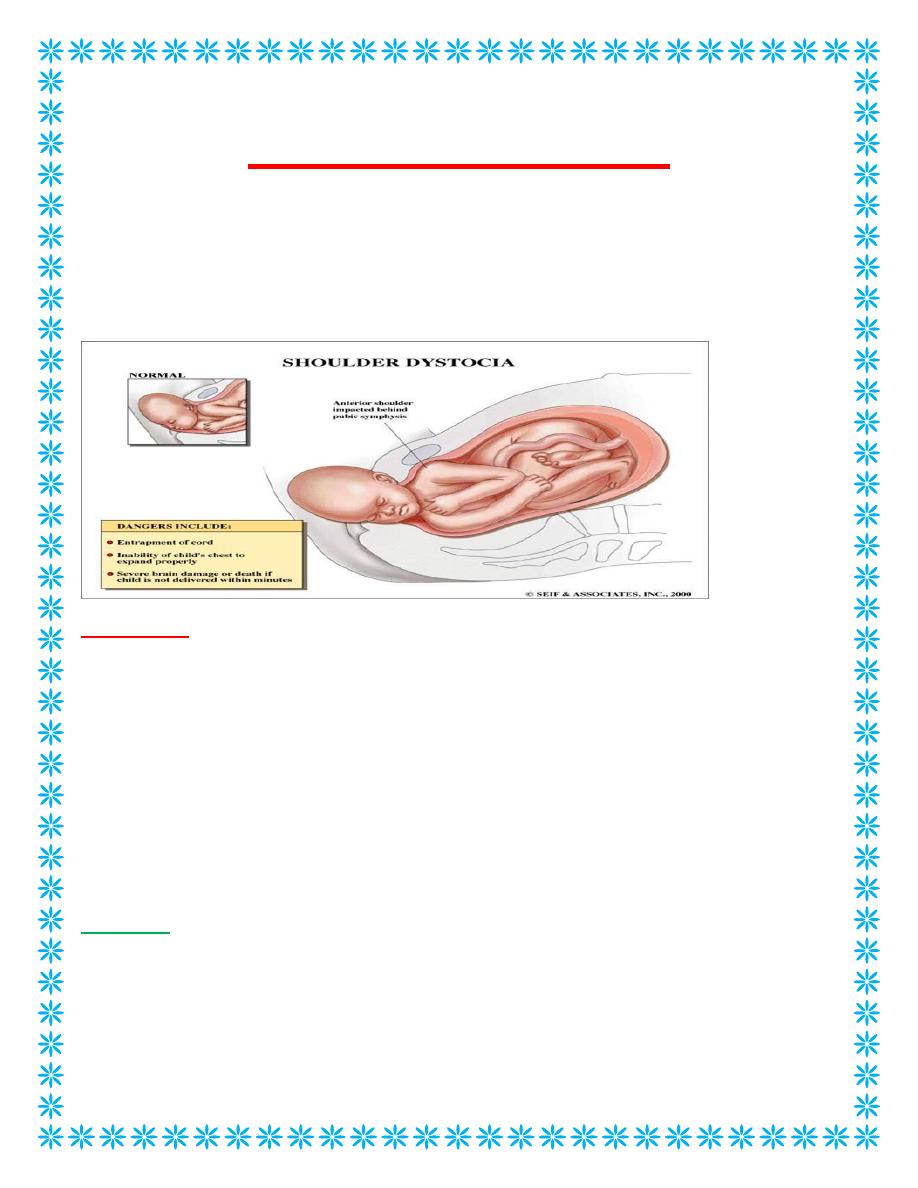
Shoulder Dystocia
A delivery that requires additional manoeuvres to release the shoulders after gentle
downward traction has failed. Shoulder dystocia occurs when either the
anterior
or, less
commonly, the
posterior fetal shoulder
impacts against the maternal symphysis or sacral
promontory.
Incidence :-
Is approximately 0.6% in UK
Risk factors
Shoulder dystocia is more common when associated with condition that create a large
baby in association with a small pelvis. So, gestational diabetes, especially when
uncontrolled or undiagnosed where the baby is bigger than it’s expected normal weight or
postdates where the baby has more opportunity for additional growth.
Forceps or vacuum may cause an abnormal descent of the body into the pelvis and
prevent the body from rotating to enter the pelvis. The signs of shoulder dystocia are
prolonged second stage or bobbing of the head – where the head retracts back after active
pushing.
Although many factors have been associated with shoulder dystocia, unfortunately none
of them are clinically useful predictors
Antenatal
Maternal
– Diabetes
– Short Stature
– Previous shoulder dystocia
– Obesity
– Pelvic anomalies
2
Fetal
– Fetalmacrosomia
– Postmaturity
Intrapartum
– Prolonged second stage
– Prolonged active phase of first stage
– Instrumental birth
– Induction of labour
– Augmantation by oxytocin
RISK FACTORS FOR SHOULDER DYSTOCIA
Although fetal macrosomia is the main risk factor 50% of shoulder dystocias occur in
infants of normal Wt
Complications of Shoulder Dystocia
Maternal
– Postpartum hemorrhage
– 3
rd
or 4
th
degree perineal tears
– Rectovaginal fistula
– Symphyseal separation
– Uterine rupture
Fetal
– Brachial plexus palsy
– Clavicle fracture
– Fracture of the humerus
– Fetal hypoxia
• With or without permanent neurologic damage
– Fetal death
Shoulder dystocia will still the obstetric nightmare
Clinical Manifestations
• Turtle neck sign following birth of the baby’s head. The baby’s head will retract
back against the perineum
• Routine manoeuvres for delivery of shoulders during next contraction after
delivery of the head fails.
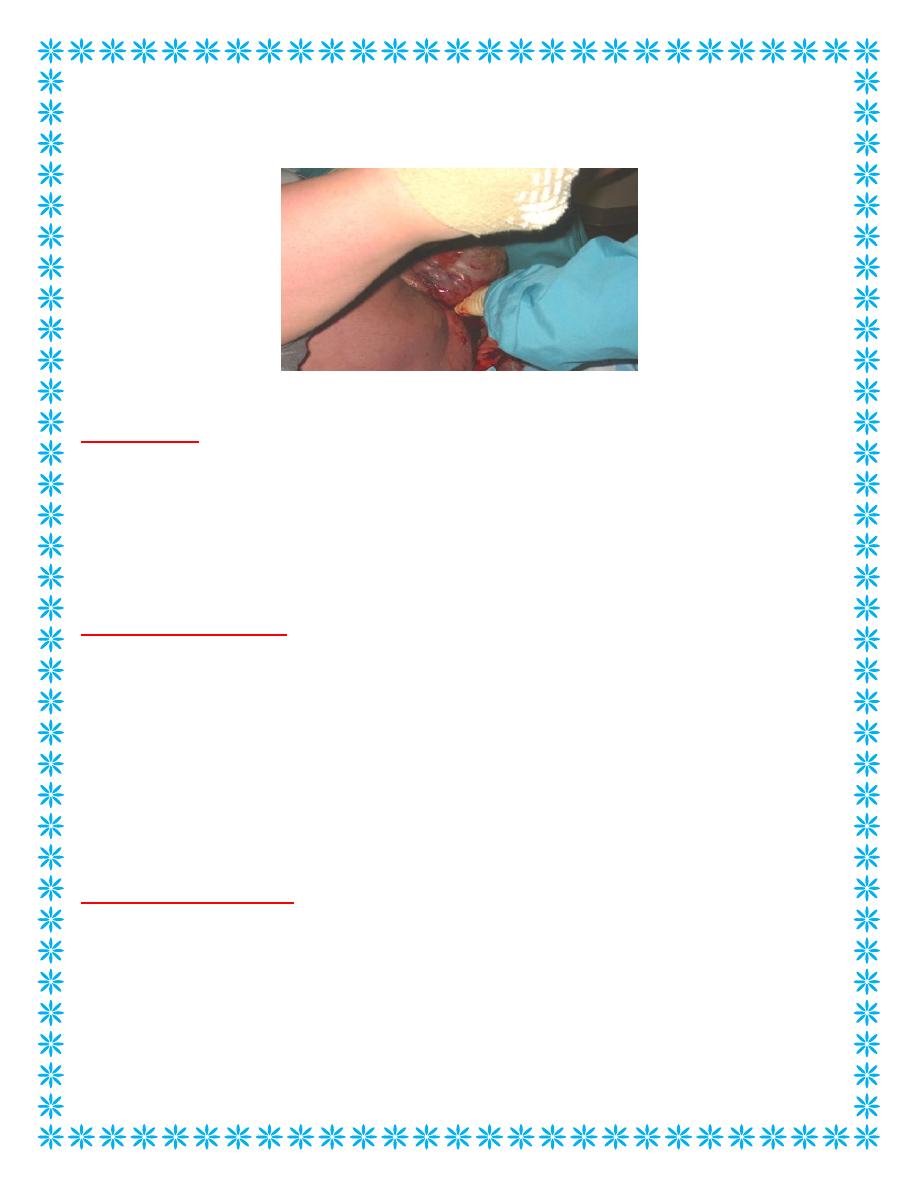
3
Shoulder Dystocia
The turtle sign
Management
• Manoeuvres aim to
– Increase the functional size of the pelvis (McRoberts)
– Decrease the biacromial diameter (Suprapubic Pressure Rubins I)
– Change the relationship of the biacromial diameter with the bony pelvis
(Woodscrew)
HELPERR pneumonic
• H – Help
– Call for assistance,anaesthetis,paediatrition
• E – Evaluate for episotomy
• L – Legs (McRobert’s Maneuver)
• P – Pressure (suprapubic)
• E – Enter the vagina
• R – Remove the posterior arm
• R – Roll the patient
– To hands and knees
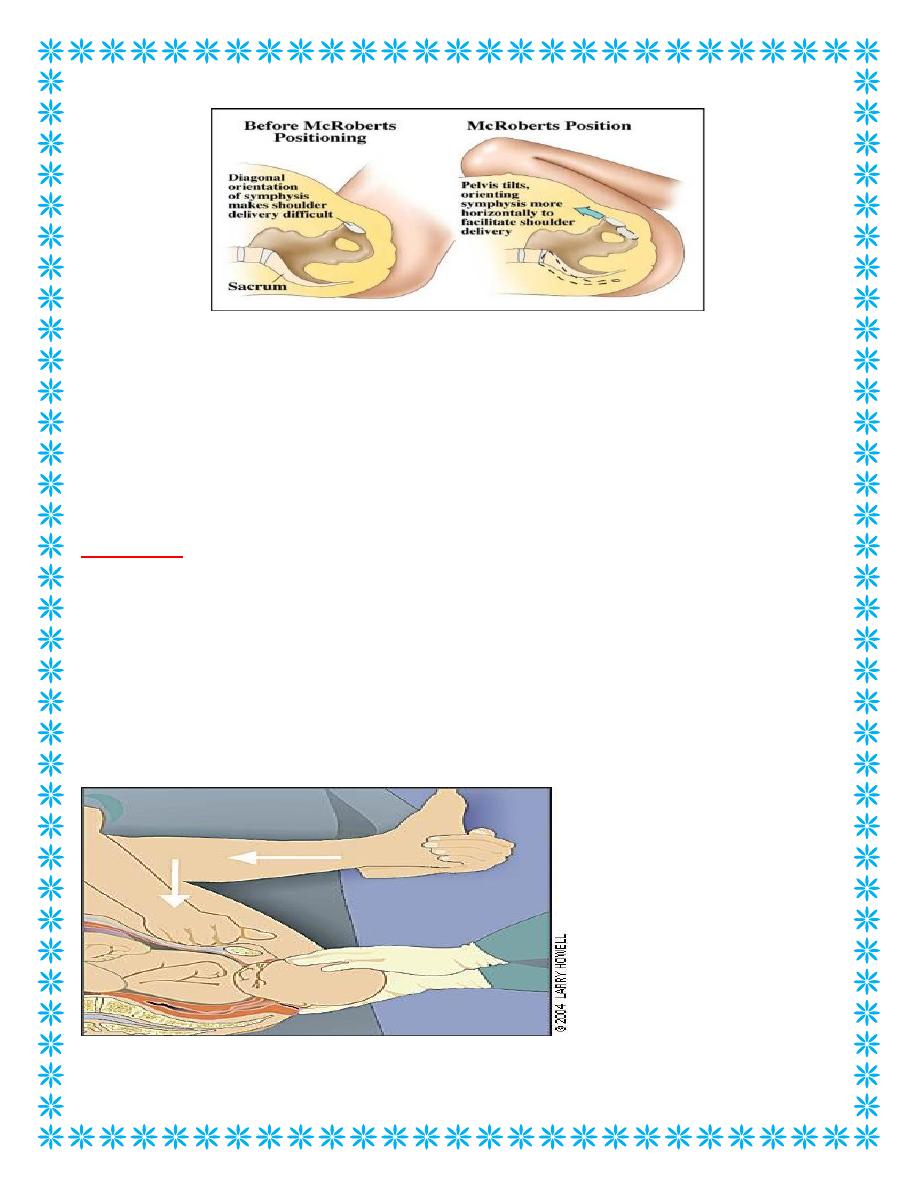
McRoberts’ manoeuvre
• The McRoberts’ manoeuvre is flexion and abduction of the maternal legs at hip,
positioning the maternal thighs on her abdomen.
• It flattens the lumbo-sacral spine, rotates the maternal pelvis cephalad so the pubis
will slip overe the shoulder.
4
Take this chance to demonstrate on the pelvis. Adduction of the shoulders is an action
that brings the shoulders closer together at the front of the body in order to reduce the
size of the shoulders. This is an automatic response we all perform when we
walkthrough tight spots and need to shrink our shoulders.
Continue McRoberts while this is being performed. This can be difficult as it doesn’t
help access to with the woman’s legs in McRoberts so the person performing suprapubic
pressure may need to stand up on something or kneel on the side of the bed
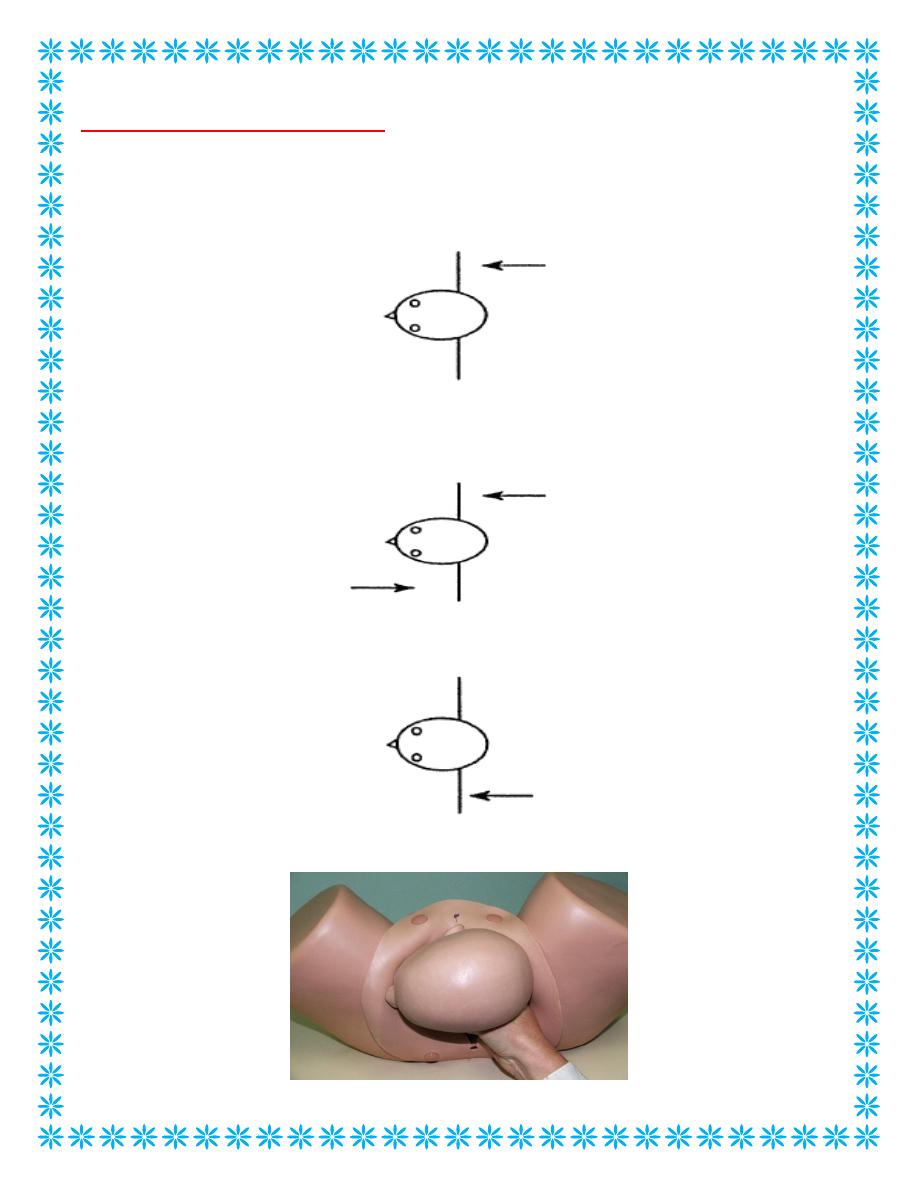
HELPERR
• Pressure – suprapubic
– Continuous pressure downward over the posterior aspect of anterior
shoulder to facilitate adduction of the fetal shoulders and reduce the
biacromial diameter.
– After 30 seconds a rocking motion of the hands can be tried to achieve the
same outcome.
McRoberts / Suprapubic pressure
5
Enter vagina(internal maneuvers)
• Rotate anterior shoulder(Rubin II):Apply pressure to posterior aspect
of anterior shoulder to adduct the shoulders then push them into the
diagonal
• Wood’s screw maneuver: Apply pressure to the anterior aspect of the
posterior shoulder while continuing to rotate the anterior shoulder
also.
• Reverse Wood’s screw maneuver: an attempt to rotate the baby in
opposite direction.
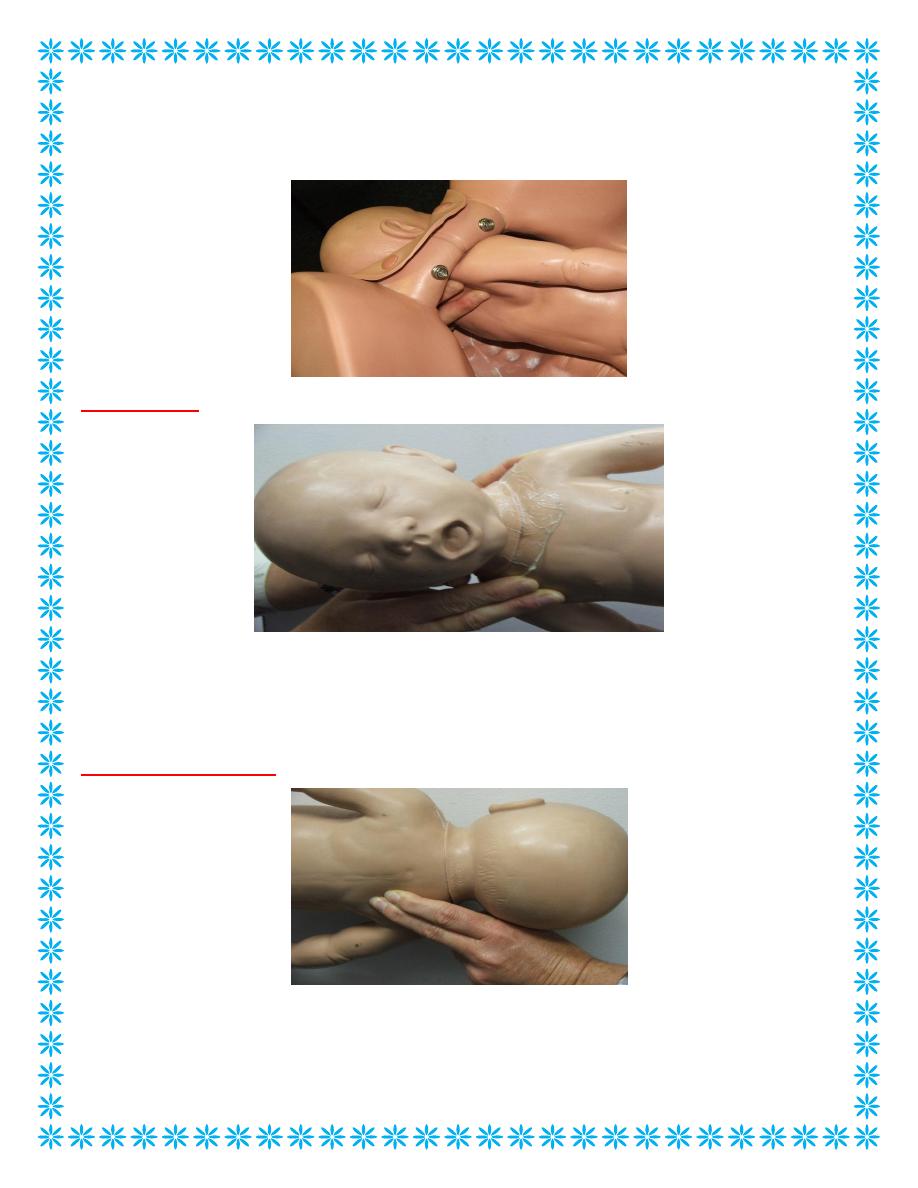
6
Your hands must enter from below the fetal head, like a scouts salute, as there is no room
above the head for your hands to enter. Encourage everyone to get down low, perhaps
kneeling on the floor to perform this manoeuvre.
Woods screw
Leaving the hand in with fingers on the anterior shoulder, the second hand is placed with
fingers against the front of the posterior shoulders. The aim of this manoeuvre is to to
rotate the shoulders into the obliques diameter.
Reverse Woods screw
This is the position of the hands for performing the reverse Woods Screw Manoeuvre for
30 secs. The fingers that were previously placed on the anterior shoulder are now slipped
down to the posterior shoulder and the other hand is removed. The aim of this
7
manoeuvre is to try to push the posterior shoulder in the opposite direction to the woods
screw, pushing the shoulders into the opposite oblique diameter hopefully freeing the
posterior shoulder to facilitate birth.
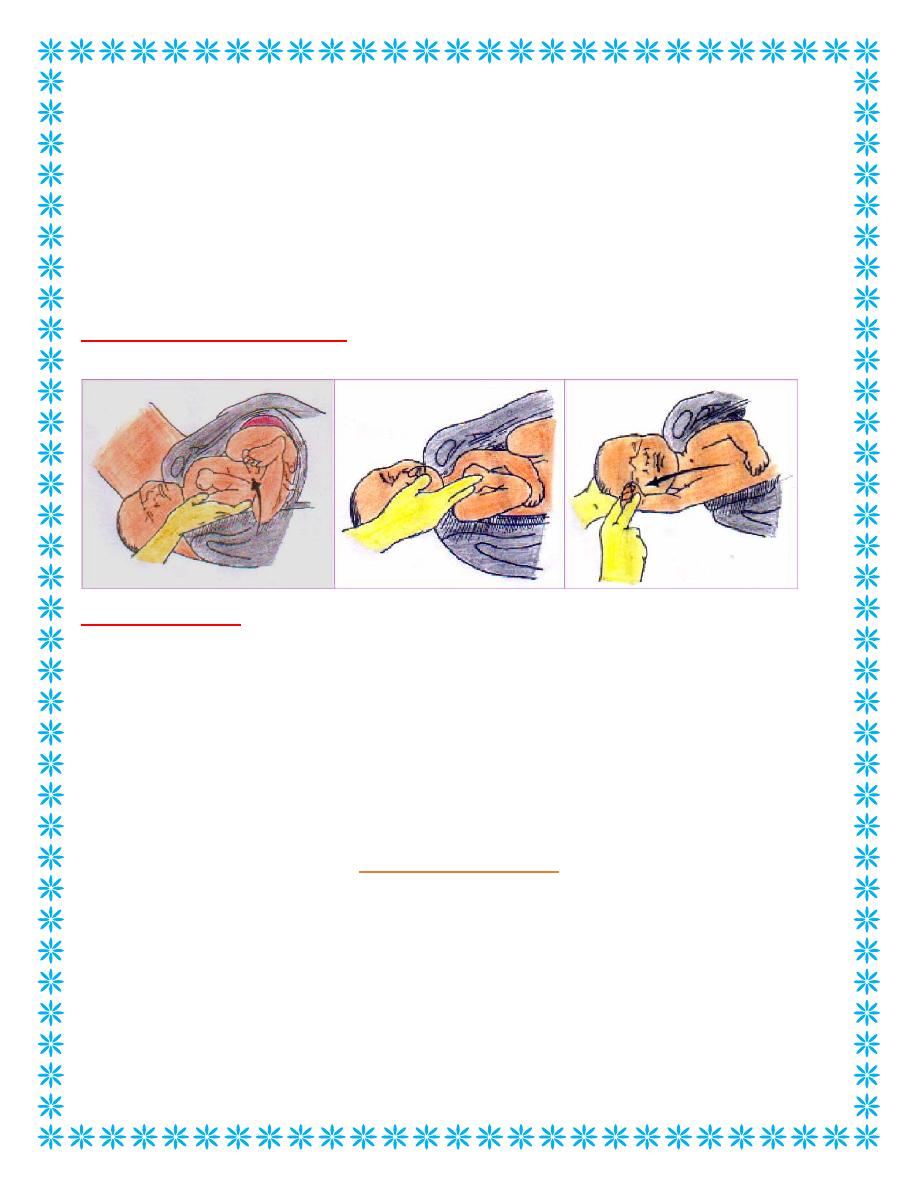
Shoulder dystocia
• Remove posterior arm:passingahand in front of the post.shoulder&deliver the post
arm by swinging it infront of fetal chest.
Delivery of the posterior arm.
Shoulder dystocia
• Roll pt on to all fours:to increase the anterio-posterior diameter of the inlet.
Last resort measures
– Fracture clavicle
– Zavanelli maneuver
– Symphysiotomy
All- Fours Manoeuver
It consists of placing the patient onto her hands and knees
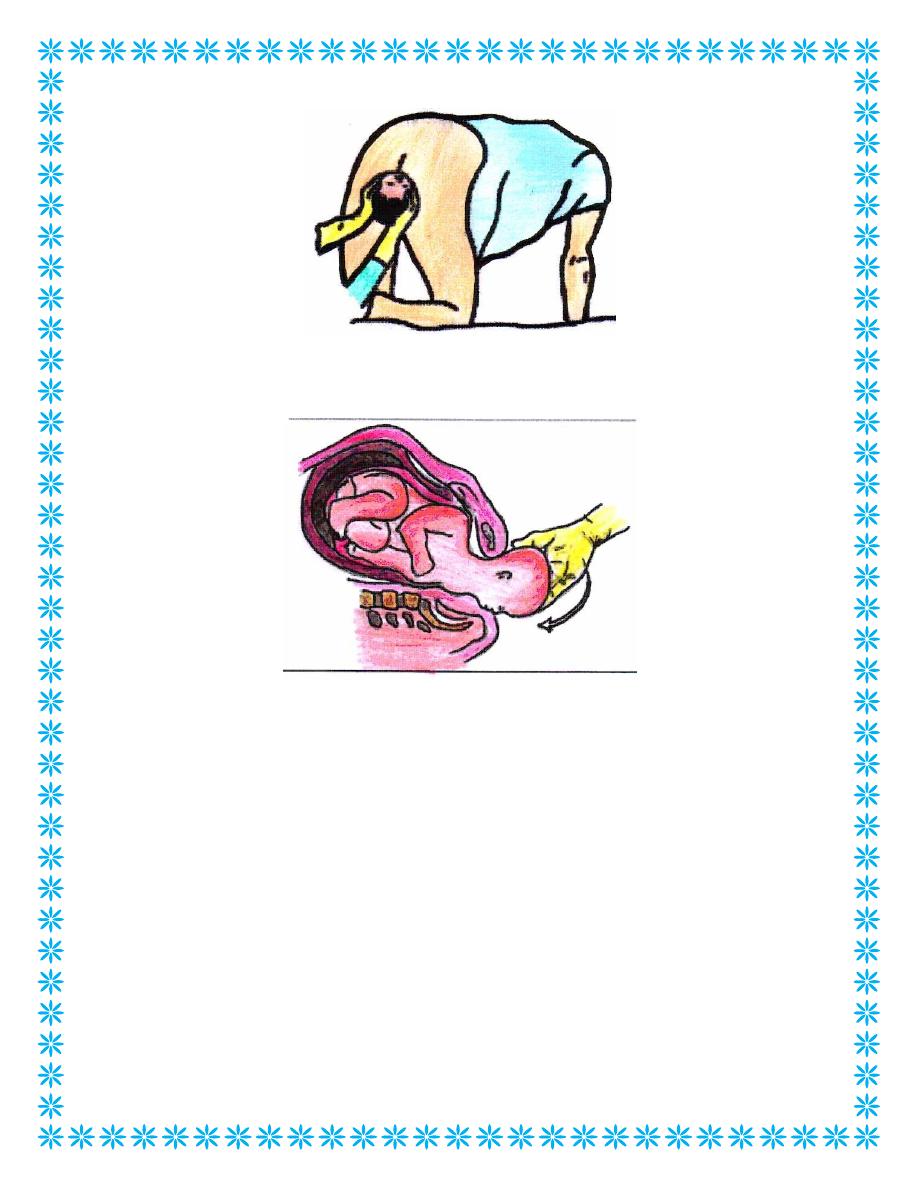
8
2.Flexion of the head, Returning it to the vagina with upward constant firm
pressure, followed by CS