Obstetrics
Dr. Aseil
1
UTI in Pregnancy
Pathophysiology
Hormonal
Mechanical
Hypertrophy of the kidney
Hormonal
Progesterone relaxation of the smooth muscles of the whole tract
dilatation of the pelvis & ureter & Vasico-uretral reflux
stasis of urine predispose to infection
Mechanical
By gravid uterus, on :
Bladder wall get pushed up into the abdomen :
frequency of urination, Stress incontinence
ureter at pelvic brim obstruction of the ureters hydronephrosis.
Hydronephrosis & hydro- ureter is more in right side (50%)
because of dextro rotation of uterus to the right side.
Hypertrophy of the kidney
Structural Hypertrophy
Functional Hypertrophy:
Renal Blood Flow
GFR by 40%
urinary out put & urinary frequency
BU & serum creatinine
Glucosuria “sometimes due to filtration by the kid”
RBF & GFR over come tubular re-absorption threshould
loss of glucose, amino-acids&prot…etc Na and fluid retention.
# All these changes return back to normal 4 months after delivery:

Obstetrics
Dr. Aseil
2
PATHOGENESIS OF INFECTION –
1/The female urethra measures only 3 to 4 cm in length. Its proximity to the
vagina and rectum facilitates colonization of urine from the normal flora of the
gastrointestinal tract and vagina.Migration of organisms from the introitus into
the bladder.
2/Lower renal thresholds for excretion of glucose and amino acids during
pregnancy provide an excellent media for proliferation of microorganisms.
3/ the dilated urinary collecting system (ureters and bladder) predispose the
pregnant woman to the development of infection from asymptomatic
bacteriuria.
Types of UTI in pregnancy:
1. Asymptomatic bacteriuria
2. Cystitis
3. Pyelonphritis
Risk factors
– Risk factors for UTI in pregnancy include:
• History of recurrent UTI
• Multiparity , Advanced maternal age
• Lower socioeconomic status
• Anatomical abnormalities of renal system, urinary calculi
• Diabetes mellitus
• Bladder emptying problems e.g MS
MICROBIOLOGY
– The organisms causing UTI are similar in species and
virulence factors in pregnant and nonpregnant women, suggesting that the
basic mechanism of entry of bacteria into the urinary tract is the same.
Most common organisms:
Usually comes form the peri-anal area “G-ve
E.coli 80%
Klebsiella aerogenes
Proteus mirabilis
. Others: Pseudomonus, Staphylococcus aureus, enterobacter
Obstetrics
Dr. Aseil
3
ASYMPTOMATIC BACTERIURIA
– Asymptomatic bacteriuria refers to
the isolation of actively multiplying bacteria > or =100,000 single organism/mL
from a midstream-voided specimen in a woman without UTI symptoms.
Incidence: Asymptomatic bacteriuria: 8%,
Complications (if not treated)
Symptomatic UTI 40% of them will develop “frank cystitis” or
Pyelonephritis
Preterm labor. in ¼
Anemia.
IUGR.
Cystitis:
Incidence: 1%
Presentation:
Lower abdominal pain
Dysuria , Urgency ,Frequency , Haematuria
No systemic manifestations (fever,dehydration)
Occasionally may present as law back pain ,malaise &flu like symptoms.
Diagnosis:
pyuria(>7WBCs/ml) and urine culture, RBC Micro & Macro Hematuria
General Management of Asymptomatic Bacteruria & Cystitis
Hydration to wash the bacteria
Antibiotics:
Should do the urine culture first, and begin empiric antibiotic therapy.
Then adjust, continue, or suspend the treatment depending upon the final
culture results and the patient's response to therapy.
Types of Antibiotics given:
Amoxacillin(500mg PO TID)
Augmentin(1gPO BID)
Nitrofurantoin(50mg PO QID)
Cephalosporiens e.g cefixime
full coarse for7- 10 days
If persists (i.e. +ve culture), continue Ab daily till delivery as Nitrofurantoin OD
Obstetrics
Dr. Aseil
4
Pyelonephritis
Intro
Most serious complication in pregnancy
Risk factors include asymptomatic bacteriuia, previous history of
pyelonephritis, renal and collecting system anomalies, and renal calculi
Usually is ascending
50% unilateral on the right side25% bilateral
Incidence: 1 – 2%.
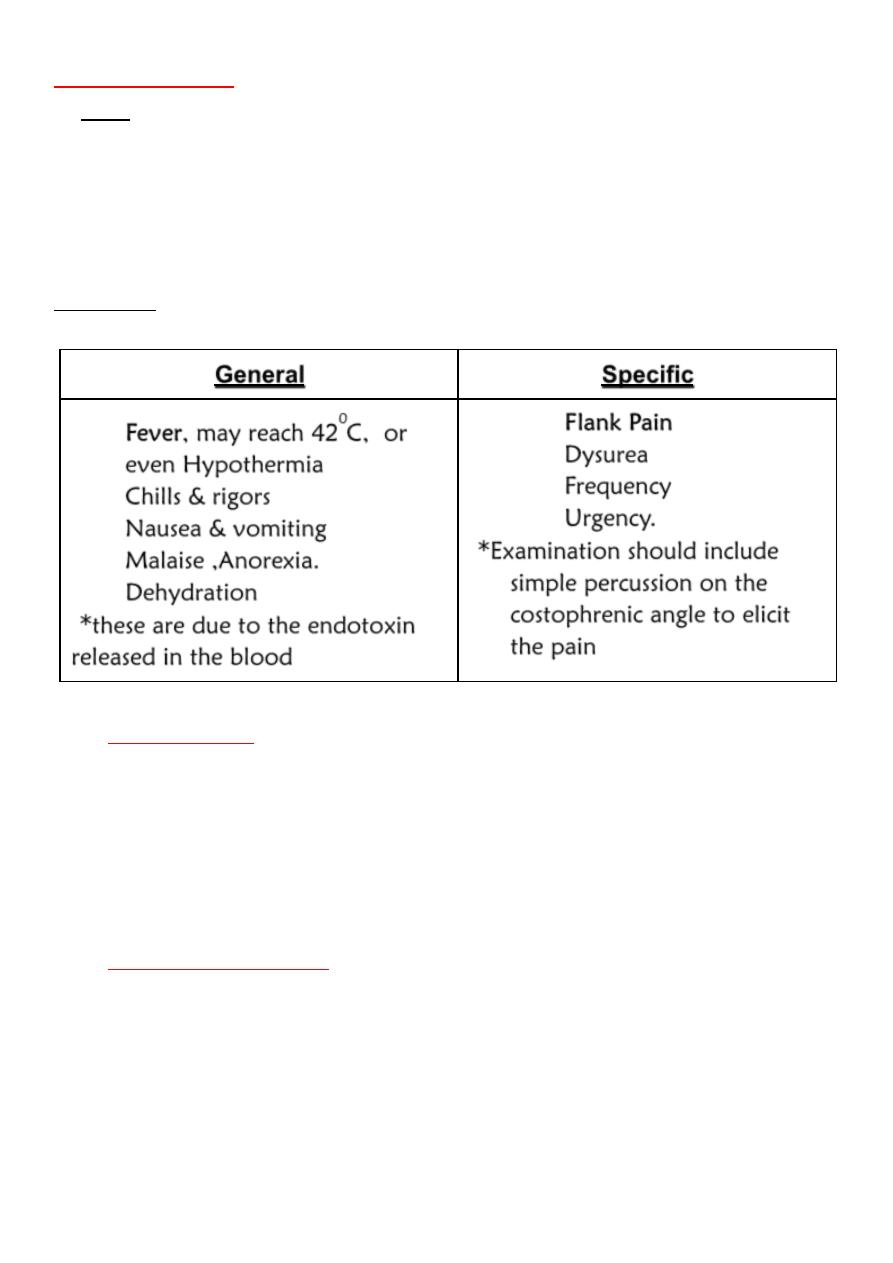
Specific
General
1.
Flank Pain
2.
Dysurea
3.
Frequency
4.
Urgency.
*Examination should include
simple percussion on the
costophrenic angle to elicit
the pain
1.
Fever, may reach 42
0
C, or
even Hypothermia
2.
Chills & rigors
3.
Nausea & vomiting
4.
Malaise ,Anorexia.
5.
Dehydration
*these are due to the endotoxin
released in the blood
Investigations:
CBC anemia , thrombocytopenia
RFT GFR & Creatinine clearance, serum creatinine
MSU Significant bacteruria, Proteinurea ,RBC cast,
Urine culture to isolate the organism (mostly E.coli).
Baby must be monitored with CTG & ULS
Differential Diagnosis:
Labour
Chorioamnionitis
Acute abdomen as Appendicitis
Ectopic pregnancy “usually present early”
Abruption placenta esp. Concealed type
Fibroid
Obstetrics
Dr. Aseil
5
Complications:
Fetal
the incidence of abortion.
the incidence of prematurity.
the incidence of prenatal morbidity and mortality
Maternal
Septic shock , ARDS
Renal insufficiency
Perinephric abscess
Management
Admit to hospital & Bed rest.,opiate analgesia
Rehydration.
Antibiotics:
Empirical treatment with IV antibiotics
Ampicllin 1g/6hr
Cloxacillin
3rd generation cephalosporins
Shift to oral Ab after 24-48 hr when she is afebrile for acourse of 14
days
Repeat culture after 2 weeks , Low dose antimicrobial prophylaxis,
such as nitrofurantoin (50 to 100 mg PO 2 times daily), and periodic
urinary surveillance for infection are recommended for the
remainder of the pregnancy to prevent a recurrence.
If still no response after 48hr parental therapy then have to
investigate the patient with ULS&IVP to exclude perinephric absces
or stones.