1
Definition:is the identification of a disease prior to birth. This includes both the screening
and the diagnostic tests for congenital abnormalities & diseases of the fetus.
Indication:if there is suspicious
Family history: genetic disease with a known recurrence risk .
Past obstetric history: RhDalloimmunization
Serum screening tests: trisomy 21
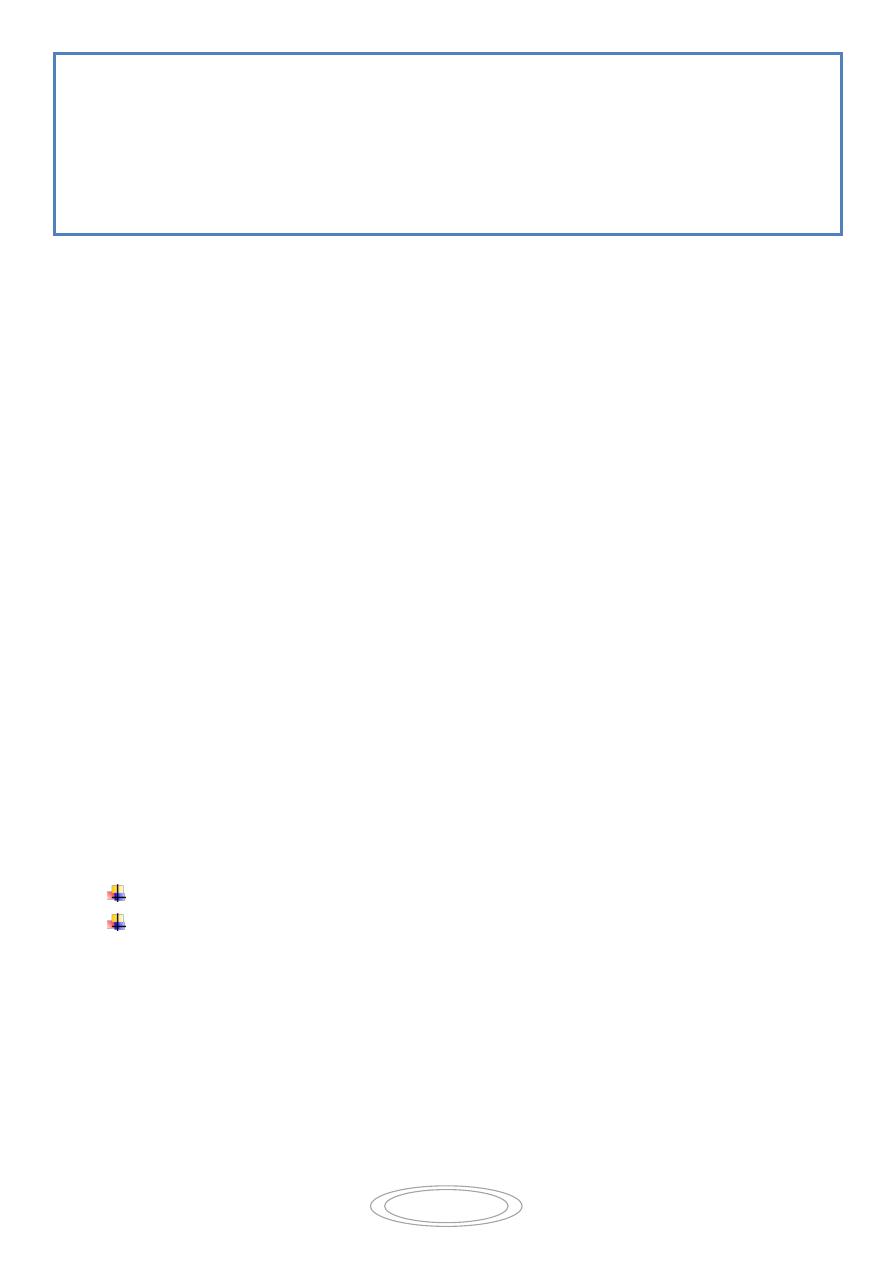
Ultrasound screening: 20 week anomaly scan.
Purposes of antenatal diagnosis:
1. Termination of pregnancy as early as possible if lethal or severely handicapping
anomalies detected.
2. Intrauterine treatment for treatable conditions
3. Planning of delivery for non lethal conditions (Time, place & mode of delivery(
4. Prepare woman emotionally for the birth of a baby with a serious condition.
I- Prenatal Screening tests:
Should be simple, affordable, available, non-invasive , sensitive & specific.
initial screening begins when the female presents first for antenatal care or as part of
pre-conceptional counseling in pregnancy counseling clinic.
history
clinical examination (Polyhydramnios, oligohydramnios) .
Screening tests include :
1. Routine booking tests
2. Screening test for Down’s syndrome
3. Screening for haemoglobinopathies .
4. Maternal serum α- fetoprotein (MSAFP(
5. Ultrasound screening
PRENATAL DIAGNOSIS OF FETAL
ABNORMALITIES
2
MSAFP is a glycoprotein that is produced from the yolk sac and then from the liver
,excreted into the amniotic fluid via fetal urine, crosses the placenta into the maternal
circulation.
Conditions causing elevated MSAFP
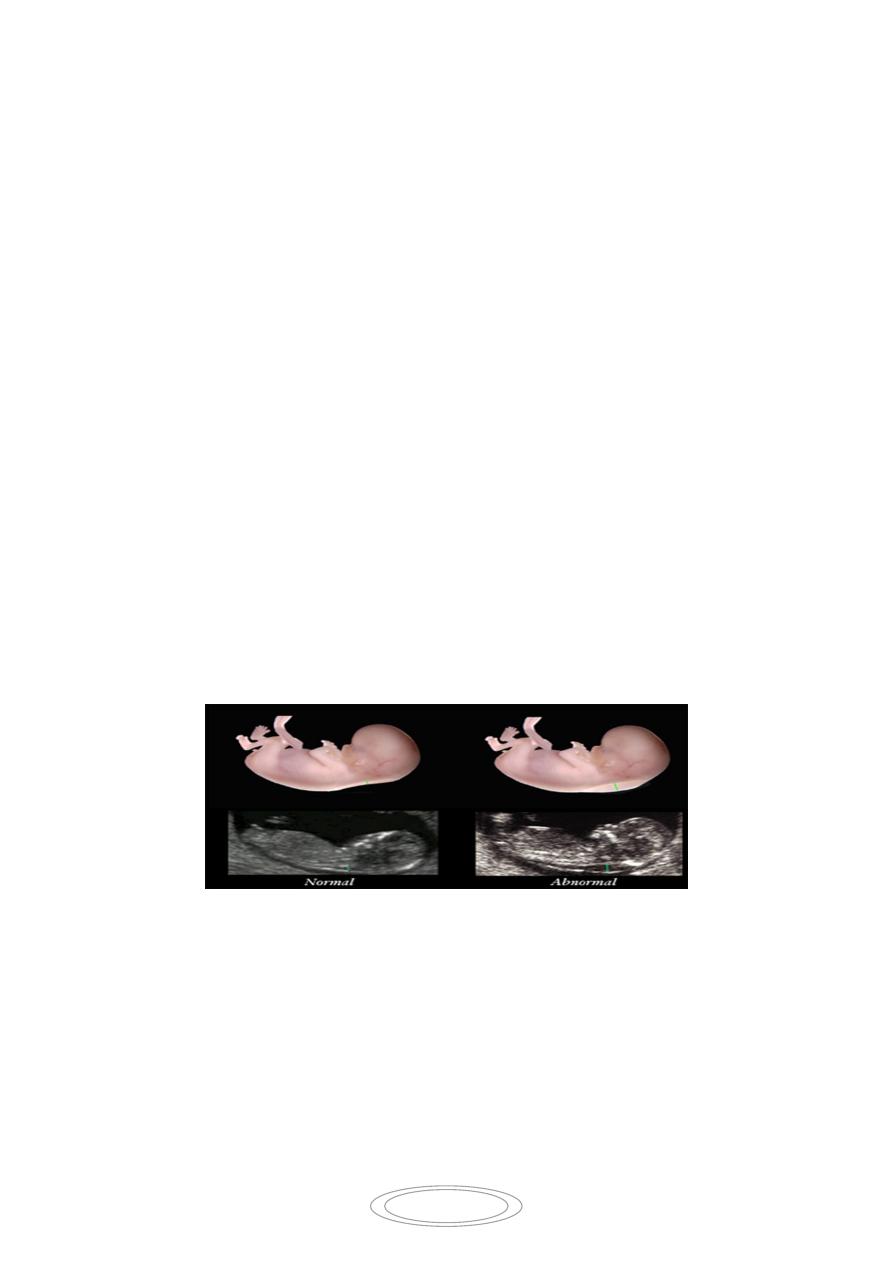
1- Open neural tube defects such as spina bifida, anencephaly.
2- Anterior abdominal wall defect (exomphalus)
3- Multiple pregnancy
4- Miscalculated gestational age
Low MSAFP is present in
1- Down’s syndrom
2- IUD.
Screening for Down’s syndrom
1- 1
- The combined test of an ULS scan to measure nuchal translucency& blood test for
the level of HCG & PAPP-A in maternal blood between 11-14w
2- 2
- Triple test of decreased MSAFP, decreased unconjugated oestriol, increased HCG.
The risk of Down’s syndrom increases with maternal age (at 35 years incidence is 1/250 , in
40 years it is 1/70 )& the individual risk is calculated by taking age related risk &adjusting
this up or down based on these tests.
II- Diagnostic tests:
The need for diagnostic test arise following a high risk screening test. This include non-
invasive tests & invasive procedures which may carry some risk , but this should be
balanced by the usefulness of the information obtained by them.
Non-invasive tests:
3
1- ULS scanning for structural fetal abnormalities e.g. NTD, gastroschisis, cystic
adenomatoid malformation of lung , renal abnormalities.
2- Maternal blood for viral serology if features on ULS are suggestive of infection e.g.
hydrops or ventriculomegaly or if there is history of exposure
3- Free fetal DNA can be extracted from maternal blood to determine fetal blood group
in cases of alloimmunization , or determine the sex of fetus in x-linked disorders
4- recently prenatal diagnostic test for aneuploid pregnancies by extracting fetal RNA
from maternal blood.
Invasive techniques:
Amniocentesis:
Chorionic villus sampling (CVS(.
Fetal blood sampling.
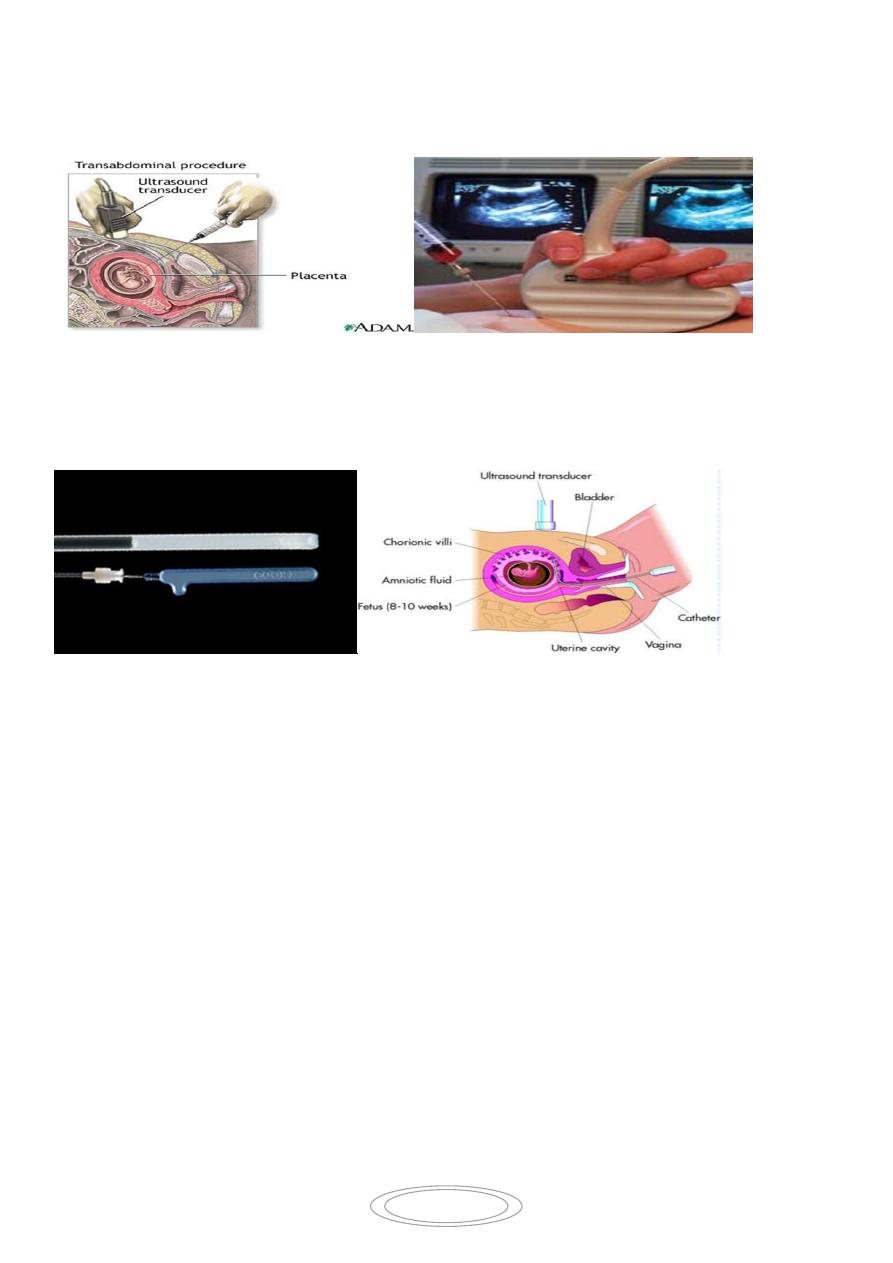
A-Chorionic villus sampling:
4
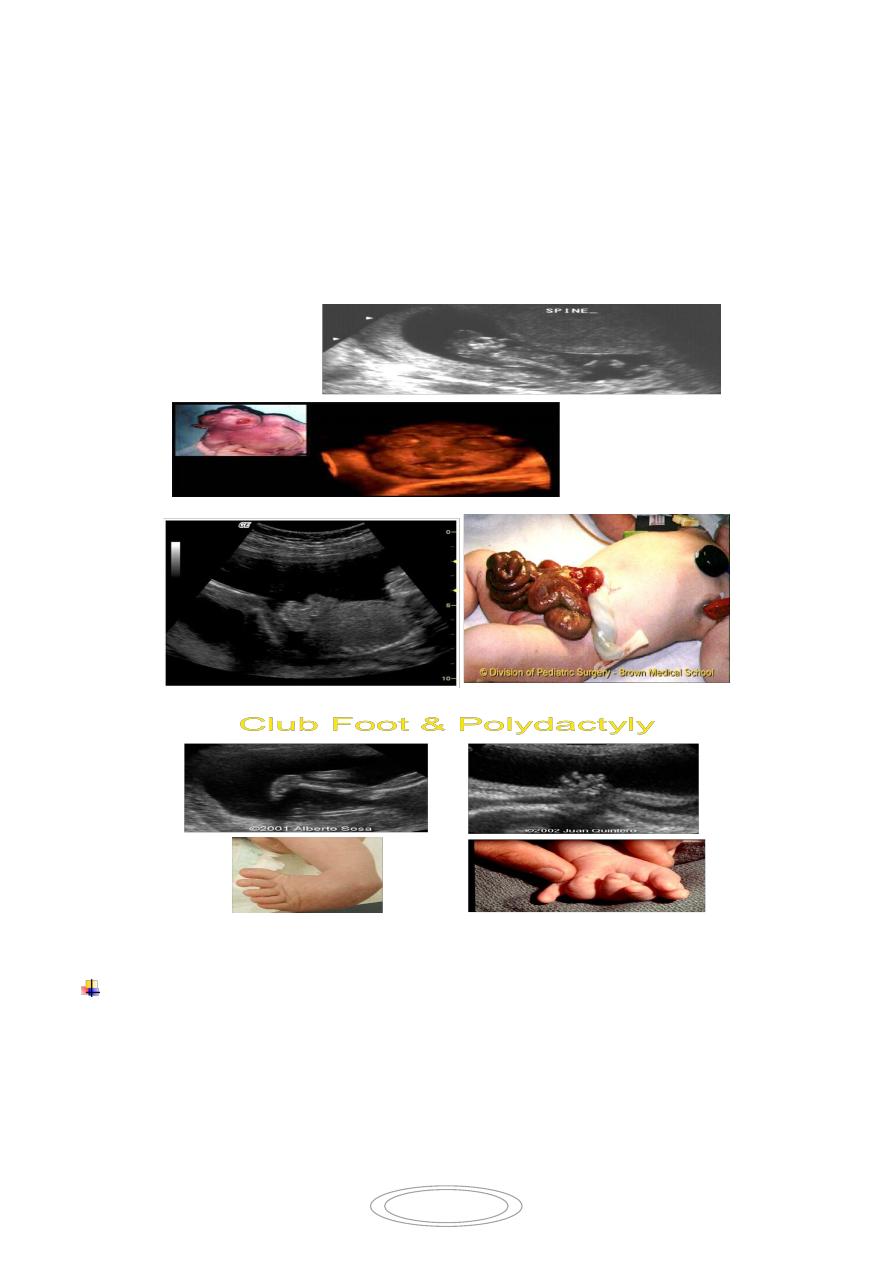
Taking a sample of fetal villous trophoblast cells in 1st trimester (after 10w(.
percutaneoustransabdominal by passing a needle under ULS guide through the
abdomial wall into the placenta.
Or by passing a fine catheter or biopsy forceps into the placenta
transvaginal
transcervical.
Indications for CVS-:
1- karyotyping
2- DNA analysis for sinle gene defects as in thalassaemia and sickle cell anaemia
3- inborn error of metabolism
4- chorionic tissue examination for organisms such as rubella or toxoplasma
complications: miscarriage 2% , limb defects.
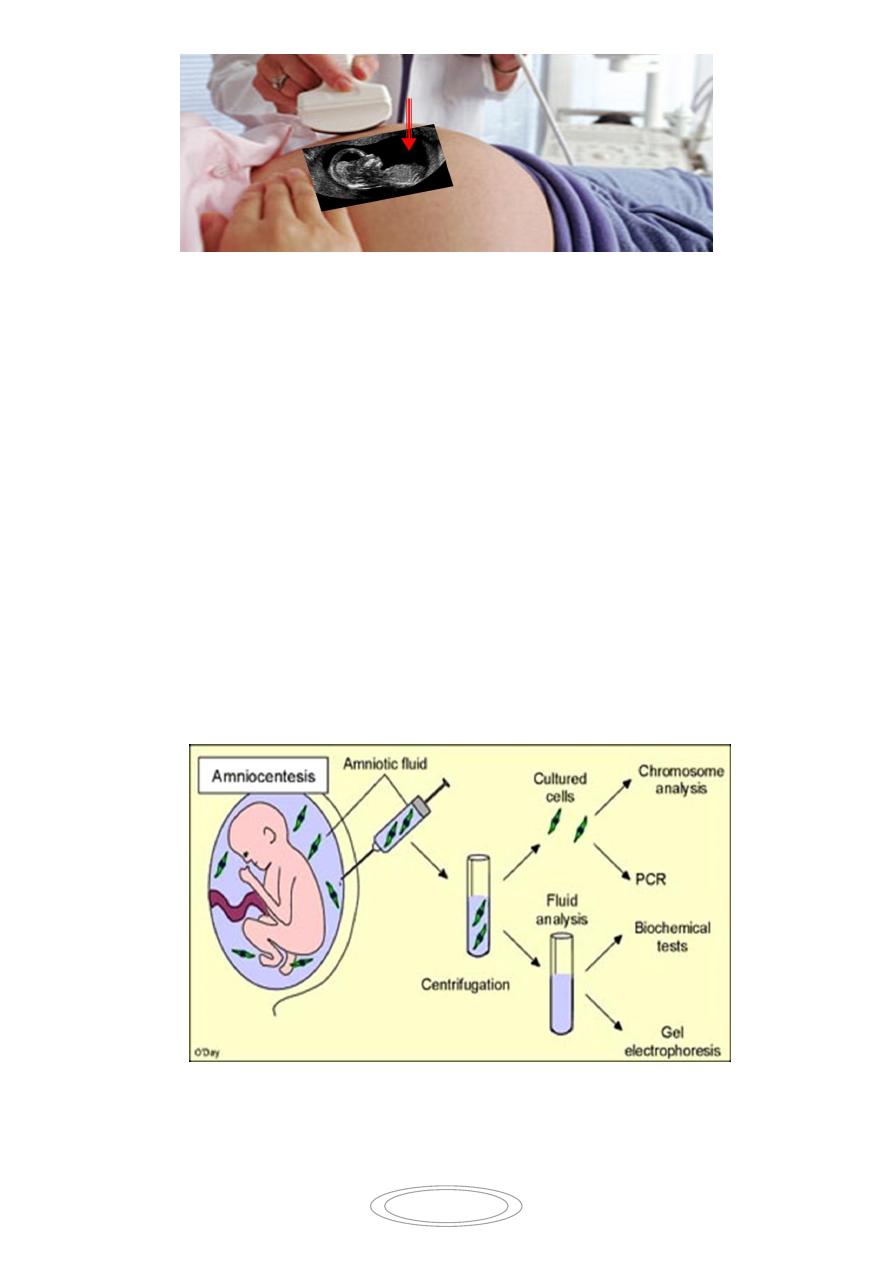
B- Amniocentesis:
Amniotic fluid contains aminocytes& fibroblasts shed from fetal membranes skin& fetal
genitourinary tract. this is done by the transabdomenal insertion of a needle using local
anesthesia into the amniotic sac under US guide and aspiration of amniotic fluid (15-
20ml)for karyotyping (aneuploidies) ,cell culture (genetic disorders) &biochemical studies .
5
Indications :
1- karyotyping for aneuploidies.
2- Genetic disorders & single gene disorders.
3- Spectrophotometric tests for hemolytic disease
4- Biochemical tests e.g AFP to detect NTD
5- lung maturity
6- Tests for viral infections e.g.CMV.
complications: miscarriage 1% , leaking liquor, fetal distress, amnionitis, ,
talipesequinovarus& Rh isoimmunization.
Types of Amniocentesis:
Late – second trimester after 15 weeks.
Early – earlier than 15 weeks gestaion.

6
C- fetal blood sampling (cordocentesis(:
A needle is passed under ULS guidance into the umbilical cord at the point of its
insertion into the placenta.
It can be performed from 20 weeks gestation & onward.
Indications :
1- karyotyping
2- hemoglobinopathy: thalassaemia and sickle cell anaemia
3- diagnosis of trans placental infection by measuring fetal IgM .
4- diagnosis and treatment of Rh incompatibility
5- check fetal platelet count when alloimmune thrombocytopenia is suspected.
complications: miscarriage(2-5%) , fetal hemorrhage.
Methods of chromosomal evaluation:
Non invasive:
Fetal cells from maternal blood
preimplantation embryos (PGD(
Invasive:
amniotic fluid (amniocentesis(
placenta (chorionic villus tissue(
Fetal blood