DISEASES OF THE MYOCARDIUM
Assistant Prof .Dr .Ghazi F. HajiCardiologist
Al-Kindy College of Medicine/Baghdad University


Definition
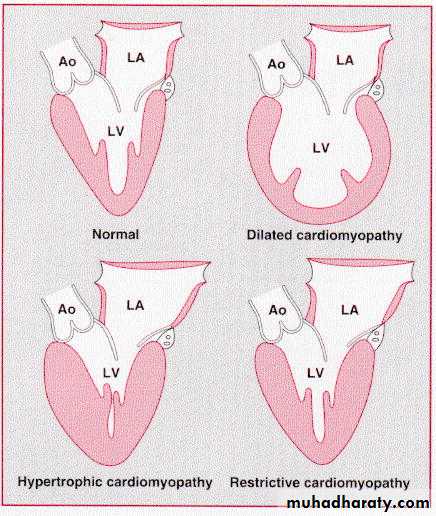
Disease primarily effect the heart muscles, as Myocarditis and CardiomyopathyDilated cardiomyopathy
Hypertrophic cardiomyopathyRestrictive cardiomyopathy
Mrs .Y 35y old female presented with flue like illness ,5days later she suffered from severe dyspnia,orthopenia,palpitation with mild diffuse chest discomfort;
On examination patient. tachypenic ,leg edema .pulse was small volume ,110 b/m ,JVP elevated and BP100/50 ;
On auscultation : heart sound was muffled,S1S1 normal ,there is S3 and apical systolic murmur. Mild Basal crackles in both lower zones .No pericardial rub ,No history of ischemia, valvular ,hypertension or congenital heart diseases.
What are the suspected differnitional diagnoses ?
How confirm the diagnosis?What is the epidemiology regarding this disease?
What are the treatment and prognosis?
Acute myocarditis
Acute inflammation of the cardiac musclesClassification; acute ,sub acute ,chronic .
Either focal or diffuse involvement of myocardium.Pathology of Myocardial damage :
1-Direct infected agent invasion of the myocyte lead to myocardial damage(necrosis )2-Auto immune response directed against the myocyte lead to further damage
Causes
1- Infectious agents :
Virus (coxacki B.HIV,Echovirus.infuenza )
Bacterial (staphylococcus.entrococcus,diphtheria)
-fungal -Chlamydia –Protozoal(chages disease)tryponosoma cruze—helminthes (trichinosis)
((Spirochetal (Lyme disease (Borrelia burgdorferi
Ricketisal
2-non infectious rheumatic fever (b hemolytic strp)
Radiation -autoimmune -systemic lupus erythematosus and rheumatoid arthritis :transplant rejection
Drugs and chemical agents(e.g. cocaine, lithium and anticancer drugs such as doxorubicin) or (e.g. penicillins and sulphonamides), lead ,carbon monoxide and Alcohol
CLINICAL FEATURES
@Presentation is variable and ranges from asymptomatic state to severe fulminate condition@Usually the patient give history of upper respiratory tract infection or flue like illness
@The true incidence unknown because most cases are asymptomatic
@ It is reversible disease and the prognosis excellentPhysical examination
Heart failure : Peripheral edema(signs of heart failure or pulmonary edema )
Small pulse volume ,Muffled heart sounds(soft s1s2)
A third heart sound ,A murmur of mitral regurgitation
Irregular beat:Tachycardia- atrial fibrillation
Chest paincardiomegaly
Investigation (young +new onset HF+ no ischemic ,valvular ,hypertension and congenital diseases ):# Blood
ECG: Sinus tachycardia
ST – T wave changes especially if pericardium involve
#Cardiac troponin and CPK may be elevated
#CXR- may be normal ,cardiomegaly ,pulmonary congestion
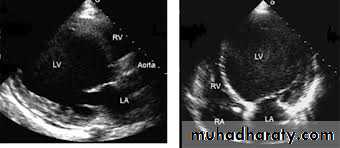
#Echocardiography may reveal left ventricular dysfunction that is sometimes regional (due to focal myocarditis),
#Endomyocardial biopsy -if the diagnosis is uncertain it can be confirmed by it.
#MRITreatment
1-Avoid any strenuous activity –avoid alcohol,
2- Preferably complete bed rest ,till the ECG change return to normal
3-If there is evidence of heart failure ,then treat with the usual measure (salt restriction. diuretic ,ACE inhibitor)
4-Anti – arrhythmic drugs are given if arrhythmias develop
PrognosisFrequently the disease passed unnoticed as upper respiratory tract infection
Some patients develop ventricular dysfunction and might presented months or years later as DCM(dilated cardiomyopathy )
Mrs .Y received her treatment and she was completely normal .
Three years later she is begin complaining from frequent attack of palpitation , fatigue ,chest tightness , progressive SOB on exertion with mild orthopenia and once attack of PND .Her illness associated with increases in body weight ( edema);s3 s4 ,systolic murmur ,CXR cardiomegaly ,pleural effusion,for that she consults a physician .
What do you think the relevant question ask by him?
What is the provisional diagnosis?What are the causes and epidemiology of disease?
Cardiomyopathy
Disease that involve the myocardium directly and are not the result of hypertension ,congenital or valvular or arterial abnormalities
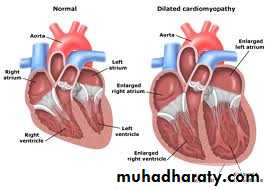
Dilated cardiomyopathy
This is characterized by dilatation and impaired contraction of the LV (systolic dysfunction)#dilated all chambers (ventricules >atrium)
Causes: In young
( myocarditis, selinum-calicum deficiency ,kawasaki disease)-In adult
( idopathic 50%,familial ,alcoholic ,myocarditis ,peripartum ,drugs like chemotherapy , tachycardia-induce cardiomyopathy , hyper-hypo thyroids, infiltrative like sarcodosis,hemochromatoasis.nuterional like thiamine deficiency ,calcium ,phosphate deficiency,eosnophilic like churg strauss)Epidemiology
@Middle age disease@Male affect more than female
@The cause usually unknown(idopathic 80%).
@Idopathic DCM differ from Ischemic cardiomyopathy
(DCM :Young, all chamber dilated , no pulmonary hypertension , mostly normal ECG)(ICM: not young ,not all chamber dilated ,pulmonary hypertension ,abnormal ECG)
@It run a progressive course ,
but reversible forms are found with alcohol abuse ,pregnancy ,thyroid diseases ,etc
Clinical features
1-Symptoms of congestive heart failure:Exertional dyspnea -Fatigue
Orthopenia -Paroxysmal nocturnal dyspnea
Peripheral edema
2- vague chest pain
3- arrhythmias :atrial fibrillation,vetricular arrhythmia different types but usually ventricle origin/may lead to sudden death
4- systemic embolization :
Patient may present with CVA, limb gangrene
It is dislodgement of mural thrombi from the dilated and poorly contractile ventricle
Physical examination
Features of congestive heart failure :Elevated JVP,
Peripheral edema
Bilateral basal crepitating .
Tender hepatomegaly
Cardiac examination :
Cardiomegaly
Soft heart sound
S3.s4 gallop
Murmurs of mitral and tricuspid regurgitation

Investigation
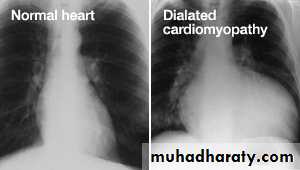
A- CHEST- CXR: 1-cardiomegaly with clear lung2-Pulmonary venous congestion
3-Pulmonary edema

B- Electrocardiograph (EKG,ECG)
May be normal ,T wave abnormality1-Arrhythmia :
sinus tachycardia-
atrial fibrillation .
ventricular ectopic
2-Low voltage
3-Conduction defect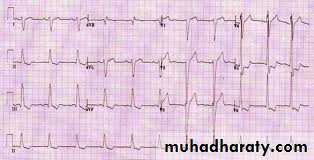
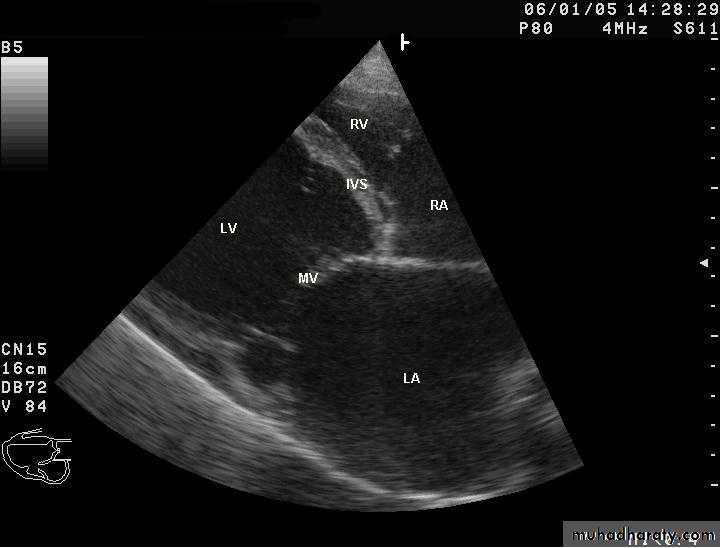
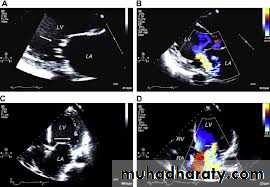
C- Echocardiography :
1- LV dilatation2-Mitral and tricuspid regurgitation
3-Reduce ejection fraction -systolic dysfunction
4- Other

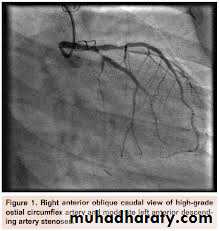
D-Cardiac catheterization :(normal coronary arteries ) to exclude coronary artery disease
E-MRI
F-Viral serology
H- End myocardial biopsy-Not necessaryUseful in some secondary types as infilterative diseases



Treatment
1-Rest 2-Salt restriction3-Anti failure drugs :aspirin,ACE inhibitor/angiotensine 11 receptor blocker? B-blocker/diuretic /digitalis
4-Anticoagulant –heparin – LMWH-oral anticoagulant
5-antiarrhythmitic drugs (amidarone),Implantable cardioverter defibrillation(ICD)Some patients may be considered for implantation of a cardiac defibrillator and/or cardiac resynchronisation therapy(CRT)
6- Immunsupression drugs-azothioprine/cyclosprine
7- LVAD-(left ventricular assistant device),
8-Cardiac transplantPrognosis
@55% die within 3-5 years. the prognosis is variable and cardiac transplantation may be indicated.@Patients with dilated cardiomyopathy and moderate or severe heart failure may be at risk of sudden arrhythmic death.
peripartum cardiomyopathy –
heart failure in last months of pregnancy or within 5 months of delivery
No obvious cause ,no ischemia or evidence of heart diseases before pregnancy; it common in woman over 30y multiparous ,multiply pregnancy ,hx of preclampcia
Aetiology : may be viral
Mortality 50%


Quiz
1-Enumerate the types of cardiomyopathy ?2-Normal cardiac size with signs and symptoms of heart failure might seen in ---------------------
3- mention 3 difference in signs and symptoms between left side and right side heart failure ?
2o years old boy presented with palpitation and dizzy spell when he was playing basketball, he had family history of sudden death , his young brother dead at age 25y and another one has mitral systolic murmur discovered on routine examination.
On examination ,patient look well ,normal vital signs but there is apical murmur on auscultation, the murmur increase by valsalva maneuver and decrease by squatting position.
What is the diagnosis?
What is the epidemiology of disease?
What are the types ?
What are the DD regarding ECHO finding?
How diagnosed and how managed ?
Hypertrophic cardiomyopathy
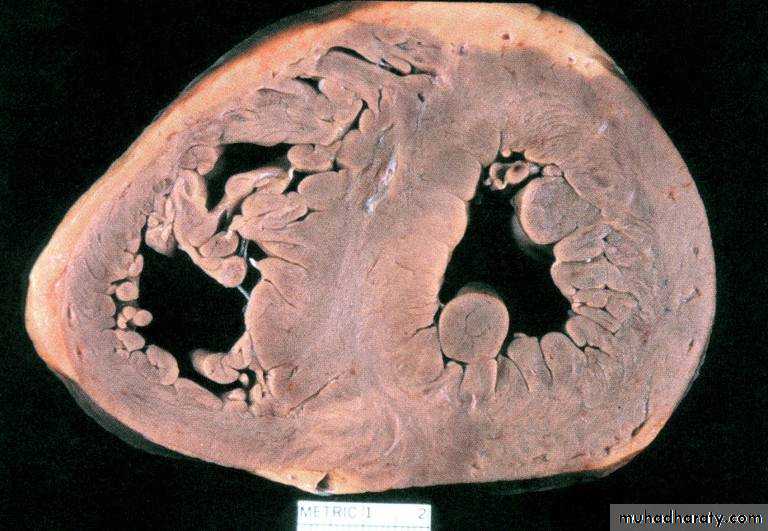
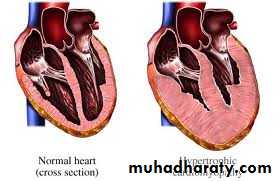
# Hypertrophic cardiomyopathy (HCM) is a disease in which the heart muscle (myocardium) becomes abnormally thick — or hypertrophied ventricular. This thickened heart muscle can make it harder for the heart to pump blood :
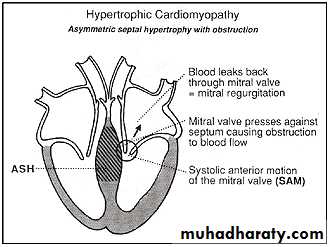
#These changes lead to abnormal movement of anterior lateral leaflet of mitral valve – this movement call (SAM)systolic anterior motion which cause mitral regurgitation.
That lead to narrowing of the subaortic area and it will lead to impede the out flow tract.
(hypertrophy obstructive cardiomyopathy (HOCM))
#(1:500 of the general population )
A familial disease ,50% of cases is transmitted as autosomal dominant trait(There are three common groups of mutation with different phenotypes) Beta-myosin heavy chain mutations ,Troponin mutations , Myosin-binding protein C)
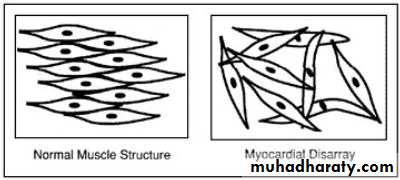
The myocardial disarray
The ventricle is stiff
and non- complaint ,that lead
to impaired ventricular filling –
diastolic dysfunction
Variants of HCM
1-Asymmetric hypertrophy-ASH- (septum and ant. wall): 70 %.2-Basal septal hypertrophy: 15- 20 %.
3-Concentric LVH: 8-10 %.4-Apical : < 2 % (25 % in Japan/Asia): characteristic giant T-wave inversion laterally
Differnitioal diagnosis regarding clinical finding is aortic stenosisDD regarding Thickening of LV wall :
Athletic heart
cardiac amyloidoses
Noonan’s syndrome
Friedreich ataxia
Fabry disease
LV-non compaction
.
Clinical manifestations
The course is variable .may be asymptomatic and run in benign courseAngina on effort -Dyspnoea on effort -Syncope on effort (dizzy spell) -Sudden death
#Fatigue
#Angina pectoris
due to increase o2 demand
by hypertrophied muscles
Physical examination
@Jerky pulse*Rapidly raising carotid arterial pulse@Palpable left ventricular hypertrophy
Double or triple impulse at the apex (palpable fourth heart sound due to left atrial hypertrophy)
@Midsystolic murmur at the base*Harsh systolic murmur in the left sternal border due to subaortic obstruction ;this murmur increase by standing ,valsalva maneuver ,decrease by sitting and squatting
@Pansystolic murmur (due to mitral regurgitation) at the apex
@4th heart soundLaboratory evaluation
$ECG:The ECG :1-normal or
2-left ventricular hypertrophy or
3-pseudo-infarct pattern(Q wave due to old myocardial infarction)or
4-deep T-wave inversion,
5-Arrhythmias- (atrial and ventricular )
$Echo:
important in diagnosis :
1- LV hypertrophy 2- small LV cavity 3- SAM 4-ASH 5-impaired diastolic relaxation
6- mitral regurgitation 7- subaortic gradient if obstructed
$CXR: usually normal.
$Cardiac catheterization
$Genetic testing may facilitate diagnosis
Treatment
*Avoid competitive exercise to decrease the incidence of sudden death*Pharmacological therapy
*Surgical myectomy*Alcoholic septal ablation
*Dual chamber pacemaker (DDD)Pharmocological therapy
Beta-blockers, calcium antagonists (e.g. verapamil) and disopyramide : used to relive angina ,decrease the incidence of syncopal attack and decrease the risk of arrhythmia@Digoxin and vasodilators may increase outflow tract obstruction (should be avoided)
*Amidarone : antiarrhythmic -- use to reduce supraventricular and ventricular arrhythmia and to decrease sudden death
dronaderone :non-iodinated and thus causes little anti-thyroid effect
(S.E: thyroid disease, lung fibrosis, brown skin discoloration- (cataract, prolong QT interval
*Anticoagulant If atrial fibrillation present
*Surgery :Outflow tract obstruction can be improved by partial surgical resection (myectomy) to improve symptoms in symptomatic patient who not responsive to medical therapy*By Catheterization : iatrogenic infarction of the basal septum (alcoholic septal ablation) using a catheter-delivered alcohol solution.
*Permanent pacemaker (DDD) Pacing the ventricle from the right ventricular apical lead position allows the apical segments to contract prior to the basal segments and helps with ventricular emptying before the outflow obstruction can occur--Chronic pacing may result in remodeling of the ventricle, such that there is widening of the left ventricular outflow tract to further decrease the gradient
*An ICD(Implantable cardioverter defibrillation) should be considered in patients with clinical risk factors for sudden death (ventricular arrhythmia,cardiac arrest)
Risk factors for sudden death in hypertrophic cardiomyopathy
1-A history of previous cardiac arrest or sustained ventricular tachycardia2-Recurrent syncope
3-An adverse genotype and/or family history
4-Exercise-induced hypotension
5-Non-sustained ventricular tachycardia on ambulatory ECG monitoring
6-Marked increase in left ventricular wall thickness

43 year old female with Hodgkin's lymphoma treated with radiation and chemotherapy. Presents with worsening SOB, weight gain(edemia) and fatigue.
JVP elevated and tender hepatomegaly ,Echo reveals normal size ventricles with biatrial dilatation
What is the diagnosis?
What are the causes?What are the investigations?
What are the lines of treatment?
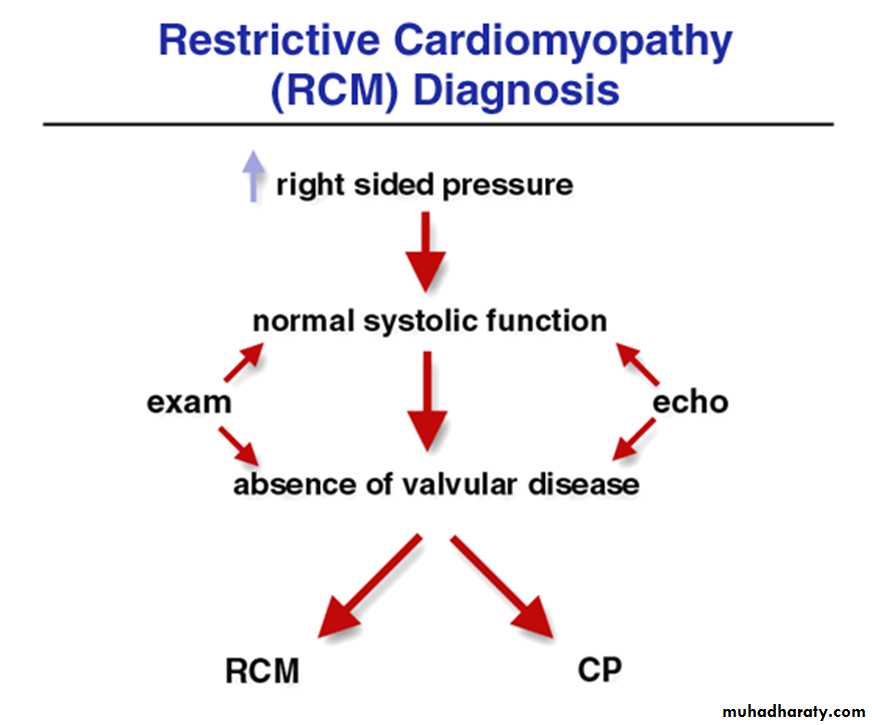
Restrictive cardiomyopathy
@Due to excessive rigidity of the ventricular wallImpaired ventricular diastolic filling(diastolic dysfunction)
Fibrotic or infiltrated
myocardiumNon-dilated ventricles
with dilated atria
Normal systolic function
with impaired ventricular
filling (diastolic dysfunction)
@Bilateral atrial hypertrophy – dilatation– atrial fibrillation – atrial thrombosis– systemic embolization
CAUSES
MyocardialllNon-infiltrative:
Idiopathic
Familial
Hypertrophic
Scleroderma
Infiltrative:
Amyloid
Sarcoid
Gaucher’s
Storage disease
HemochromatosisGlycogen storage disease
Fabry’s
Endomyocardial fibrosis
Hypereosinophilic syndrome
Carcinoid
Metastatic malignancy
Radiation
Chemotherapy toxicity
Clinical manifestationMost important features :
$ Exercise intolerance and dyspnea
$Elevated JVP prominent descend of Y wave .kaussmol s sign might be positive$Dependent edema
$Ascite$Pulsatil ,Tender hepatomegaly
$Weakness –fatigueInvestigation
#ECG:– 1-non specific ST wave changes-2-arrhythmia(atrial fibrillation)
#ECHO : although ventricul not dilated ;the
1-atrium is dilated – Ventricul not dilated2-diastolic dysfunction- reduce ventricular volume
#CXR : may be normal
pleural effusion
#Catheterization:
#CT or MRI# Endomyocardial biopsy is useful in diagnosis of secondary causes
Treatment
Prognosis is badNo defintive treatment
Treatment is usually symptomatic
Anticoagulant to prevent thromoembolismCardiac transplantation is the only definitive treatment
Arrhythmogenic right ventricular cardiomyopathy
*It is inherited as an autosomal dominant trait and
right ventricular myocardium are replaced with fibrous and fatty tissue
*Clinical problems are v .arrhythmias, sudden death and right-sided cardiac failure.
*The ECG typically wide QRS complex and inverted T waves in the right precordial leads.*MRI is a useful diagnostic tool
*Patients at high risk of sudden death can be offered an ICD.Atrial myxoma
Primary tumour rare but secondary metasetasis to pericarduim is common (most primary tumour is benign 70% like atrial myxoma )$Commonly arise in the LA attached by a pedicle to the interatrial septum.It Close mitral valve ,some time superimposed by thrombus
$diagnosis :
History :pyrexia of unknown aetiology, syncope, arrhythmias or emboli. features suggestive of a connective tissue disorder, including a raised ESR
Clinical :produce finding like mitral stenosis (loud s1 ,diastolic murmur and tumor plop)
Echocardiography: confirm the diagnosisTreatment : surgery -fewer than 5% of tumors recur.

