Primary biliary cirrhosis (PBC)
It is an autoimmune liver disease that generally affects middle-aged women . PBC is characterized by ongoing inflammatory destruction of the intralobular bile ducts, which leads to chronic cholestasis and biliary cirrhosis, with consequent complications such as portal hypertension and liver failure.• Features:
• Jaundice with pruritus(cholestasis) – deposition of bile acids and bile salts in skin.• Malabsorption – bile salts do not enter S.I.
• Skin xanthomas – due to hyperlipidemia & impaired excretion of cholesterol( characterized by hypercholesterolemia)and xanthelasma on eye lids.Also associated with darkening of skin (bronz skin).
• Increased serum alk. phos. – released due to detergent action of retained bile salts on hepatocyte membrane.
• Deficiency of fat soluble vitamins (A, D or K).
• Diagnostic test is +ve AMA (antimitochondrial antibody).

Skin xanthomas
TREATMENT:URSODEOXYCHOLIC ACID: Treatment with liflelong UDCA leads to rapid improvement in liver biochemical test levels and a decrease in the histologic severity.
• Replacement of fat soluble vitamins (A, D or K).
• Liver transplantation is effective in the treatment of decompensated PBC.
• NOTE: Both AIH and PBC can overlap on each other or can be associated with other systemic immune disease like Sjogren's syndrome and thyroid disease.
• Obliterative fibrosis of intrahepatic and extrahepatic bile ducts
• Male dominant
• Associated with ulcerative colitis
• Jaundice, cirrhosis + increased incidence of cholangiocarcinoma
• DX: ERCP
• RX: URSO , may need THERAPEUTIC ERCP ( dilation or stenting).
• can overlap with AIH.
Circulatory Disorders
Pre-hepatic Obstruction to Blood Flow• Obstruction of blood flow to the liver (i.e., hepatic artery and portal vein)
• Hepatic artery thrombosis with infarction• Causes: liver transplant rejection or vasculitis due to polyarteritis nodosa
• Portal vein thrombosis
• Causes: pylephlebitis (inflammation of portal vein, usually due to acute AP), polycythemia vera, hepatocellular CA (invasion of portal vein)
Circulatory Disorders
Intrahepatic Obstruction to Blood Flow• Obstruction to sinusoidal blood flow
• Causes:• cirrhosis
• centrilobular hemorrhagic necrosis
• peliosis hepatis
• sickle cell disease
Circulatory Disorders
Intrahepatic Obstruction to Blood Flow
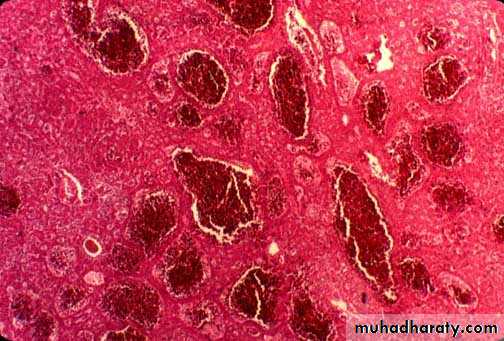
• Centrilobular hemorrhagic necrosis
• Most often due to left-sided HF and right-sided HF• LHF decreased cardiac output hypoperfusion of liver ischemic necrosis of hepatocytes around central vein
• RHF back-up of systemic venous blood into central veins and sinusoids
Circulatory Disorders
Intrahepatic Obstruction to Blood Flow• Centrilobular hemorrhagic necrosis
• Enlarged liver with mottled red appearance (“nutmeg” liver) congestion of central veins and sinusoids)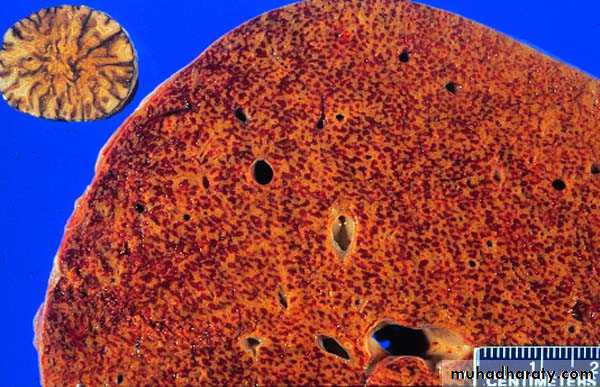

Circulatory Disorders
Intrahepatic Obstruction to Blood Flow• Peliosis hepatis
• Sinusoidal dilatation due to blood
• Causes: anabolic steroids; Bartonella henselae
Circulatory Disorders
Post-hepatic Obstruction to Blood Flow• Obstruction of blood flow out of the liver (e.g., hepatic vein)
• Causes:• Hepatic vein thrombosis (Budd-Chiari syndrome)
• Veno-occlusive disease
Circulatory Disorders
Post-hepatic Obstruction to Blood Flow• Budd-Chiari Syndrome
• Thrombosis of the major hepatic vein causing extreme blood retention in the liver• Causes:
• Polycythemia vera – most common
• Oral contraceptive pills
• Hepatocellular carcinoma invasion of hepatic vein

Circulatory Disorders
Post-hepatic Obstruction to Blood Flow• Budd-Chiari Syndrome
• Clinical:• Enlarged, painful liver
• Portal hypertension, ascites, splenomegaly
• High mortality rate
• Laboratory: increased transaminases, increased PT