Physiological changes in laborDr Samar Dawood Sarsam
parturition• The term parturition include pre labor, labor and purperium
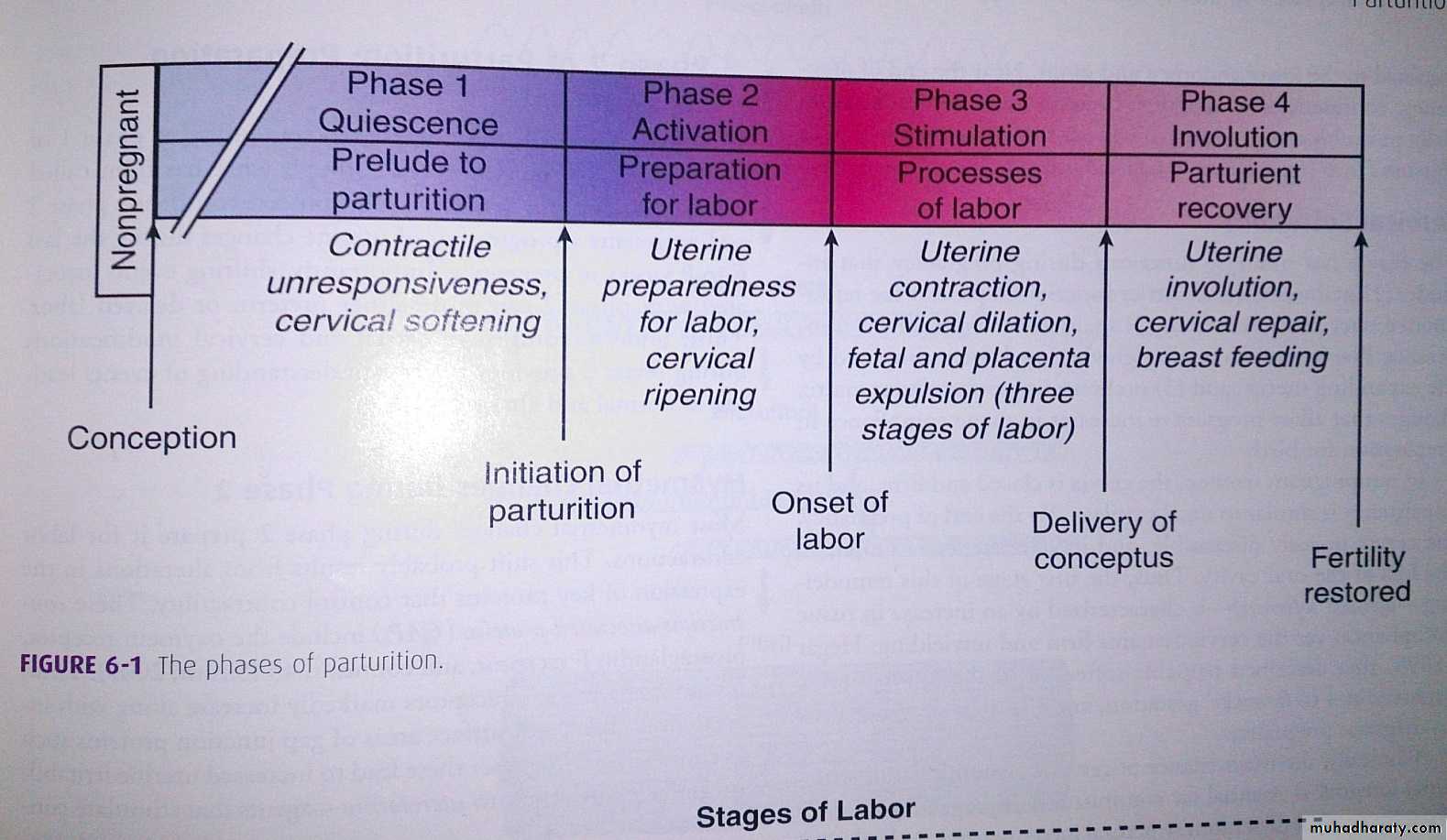
• Phases of parturition:
Phase 1: uterus quiescent, cervix softPhase 2: preparation for labor it is the progression of uterine changes during the last 6-8 weeks of pregnancy
Phase 3: labor
Phase 4: purperium
The mean duration of human singleton pregnancy is 280 days (40 weeks) from the first day of the last menstrual period. A term pregnancy is defined as the period from 259 to 293 days after the first day of the last menstrual period (37 to 41 completed weeks).
LABOR
The strict definition of labor is the onset of painful, regular uterine contractions more than one in ten minute with progressive cervical effacement and dilatation accompanied by descent of the presenting part.Or it is the process by which the fetus is expelled from the uterus.
Labor is both a physical and emotional challenge for the mother.
Labor does not begin at a point, it is a transition from the physiology of late pregnancy to labor.
Myometrial contractions that do not cause cervical dilatation may be observed at any time during pregnancy called Braxton-Hicks contractions.
As the uterus undergoes preparation for labor, Braxton-Hicks contractions become painful called false labor.
Before painful uterine contractions begin the uterus must be prepared for labor.
During the first 36 to 38 weeks of gestation, the myometrium is unresponsive; after this prolonged period of quiescence a transitional phase is required.Mechanism responsible for initiating human parturition is still unknown.
approximately 28 percent of pregnancies deliver in the 40th and 41st week and 6 percent deliver at ≥42 weeks.Twelve percent of births in the United States occur before 37 weeks and are considered preterm.
-First- the duration of pregnancy seems to be influenced by the fetal genotype.
-Secondly -prostaglandins are involved.
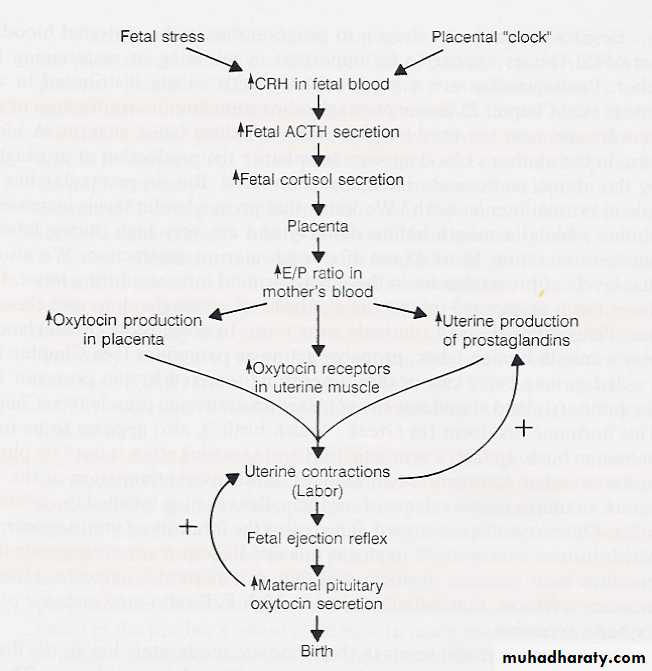
the existence of a 'placental clock', which is active from an early stage in human pregnancy and determines the length of gestation and the timing of parturition and delivery.
placental secretion of corticotrophin-releasing hormone (CRH) is a marker of this process and that measurement of the maternal plasma CRH concentration as early as 16-20 weeks of gestation identifies groups of women who are destined to experience normal term, preterm or post-term delivery.
CRH may act directly as a trigger for parturition in humans.
Fetal Endocrine Cascades Leading to Parturition:
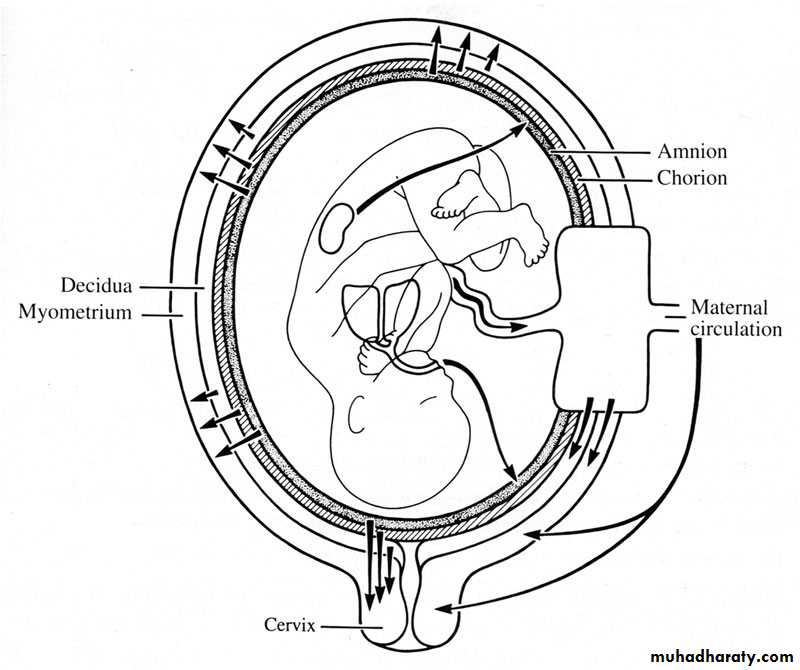
There is considerable evidence, however, that there is a placental-pituitary adrenal axis that may play a key role in the timing of human parturition. Activation of the human fetal hypothalamic-pituitary-adrenal axis is considered a critical component of normal parturition.Mechanism of initiation of labor may depend on an:
-interaction between the tissues of the fetus and the mother, namely the chorion and the deciduas.
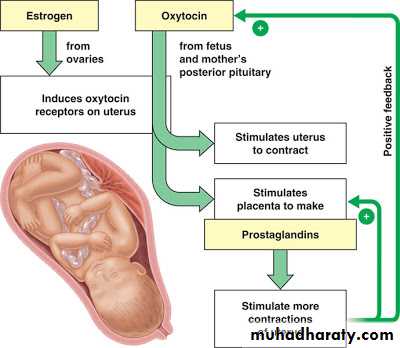
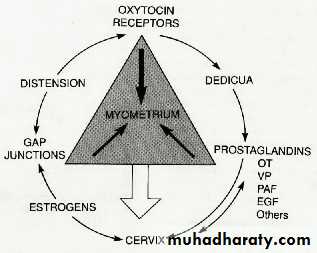
-Prostaglandin act by stimulating contractions and ripening and increasing sensitivity of the cervix to oxytocin
-steroid hormones, oxytocin, cytokines, platelet activating factor, endothelin-1 may stimulate prostaglandin synthesis.
-Corticotrophin releasing factor plays a role in initiation of labor.
Myometrial changes
Myometrial changes:
1-Increase in myometrial oxytocin receptors.2-Increase numbers and surface areas of myometrial cell gap junction proteins
Together these changes result in increased uterine irritability and responsiveness to uterotonins.
3-Another critical change that occurs is the formation of the lower uterine segment.
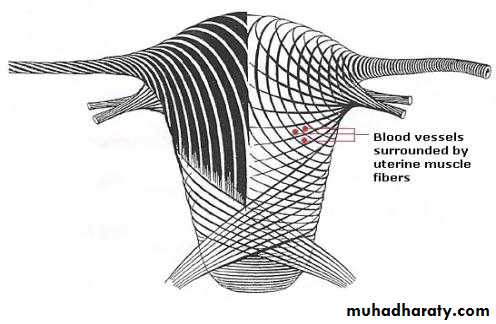
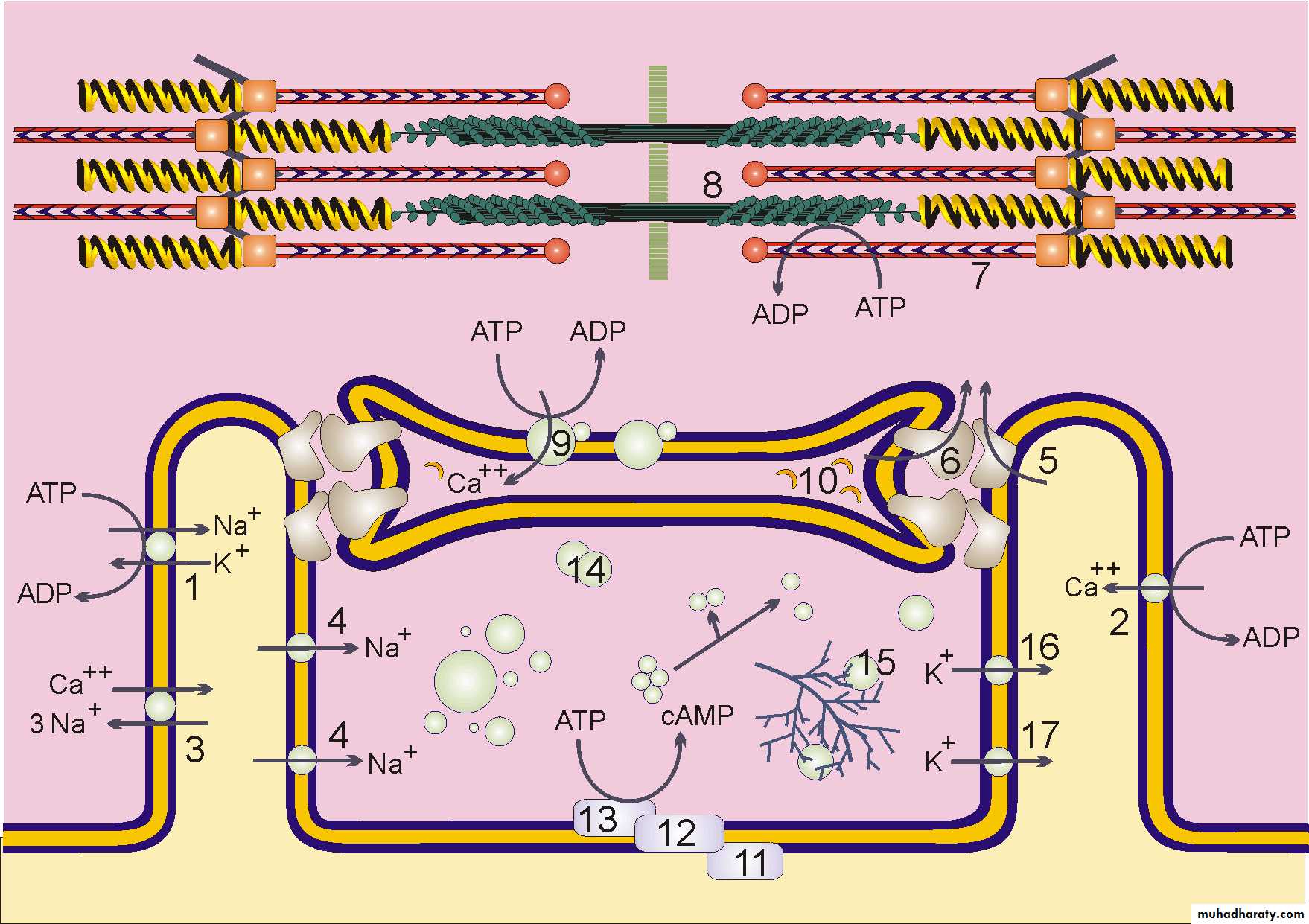
Myometrial cells contain filaments of actin and myosin.
---the interaction of myosin and actin is essential to muscle contraction. While their separation brings relaxation.---An increase in intracellular free calcium ions result in increase contractility
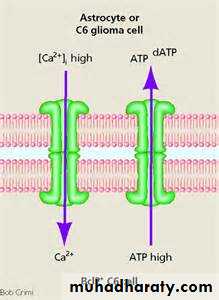
Smooth muscle contraction is regulated primarily by the reversible phosphorylation of myosin triggered by an increase in sarcoplasmic free Ca2+ concentration ([Ca2+]i).
Myometrial cells Are laid down in a mesh of collage.
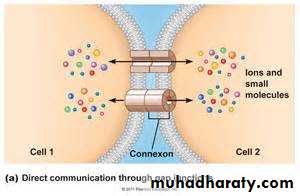
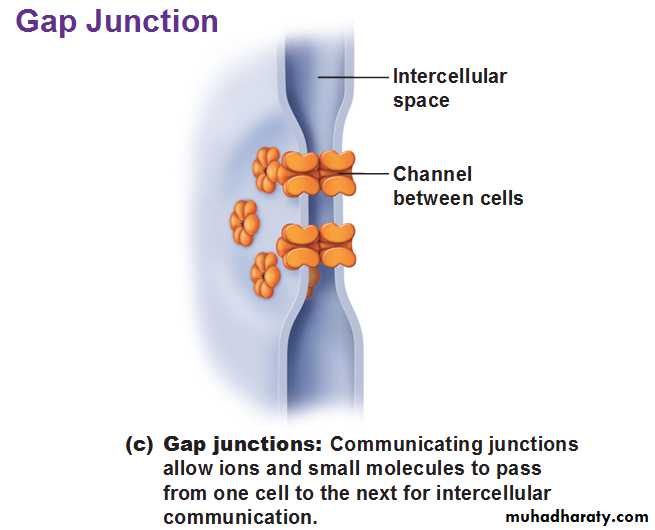
There is a cell to cell communication system by means of Gap Junctions which facilitates the passage of metabolic products and electrical current between the cells.These gap junctions increase in size and number with the actual labor and disappear afterwards. (Prostaglandin stimulate their formation).
Prostaglandins and oxytocin increase intracellular free calcium.
While agents that cause an increase in the intracellular concentration of cyclic adenosine monophosphate (cAMP) and decrease intracellular free calcium like (beta adrenergic compounds and calcium channel blockers ) promote uterine relaxation.The probability of uterine pacemaker is still not proven
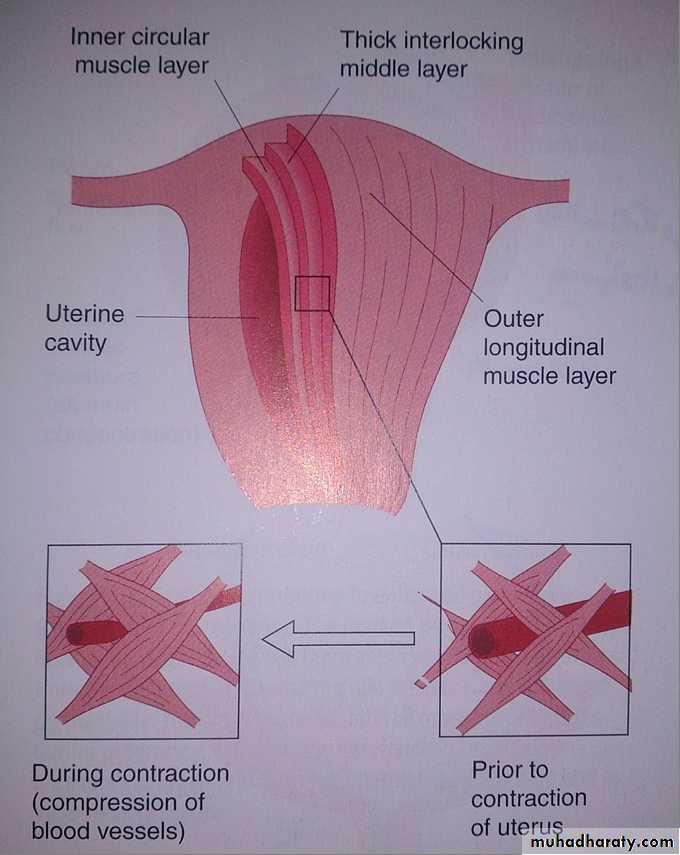
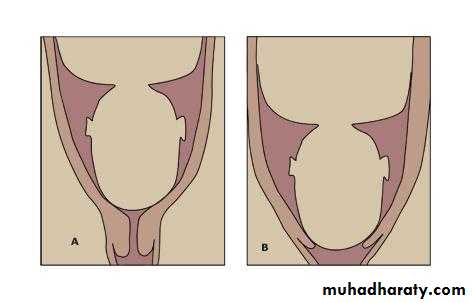
FORMATION OF DISTINCT LOWER AND UPPER UTERINE SEGMENTS.
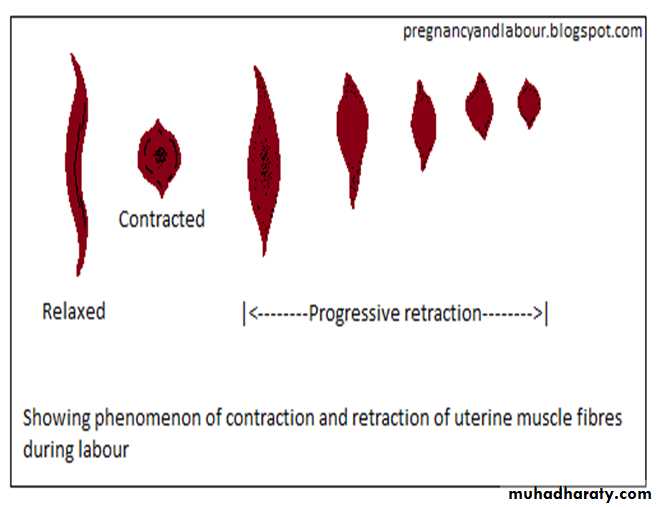
Retraction is a major feature of uterine contractility, it is progressive shortening of the uterine smooth muscle cells of the upper portion of the uterus as labor progresses.
After the cells contract they relax but they do not return to their original length.
During active labor:
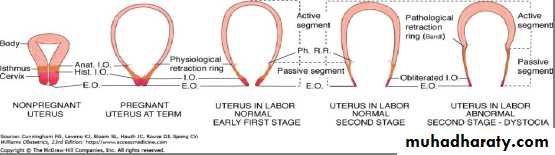
The actively contracting upper segment becomes thicker as labor advances.The lower or passive segment of the uterus and the cervix are relatively inactive compared with the upper segment. It subsequently develops into a much more thinly walled passage for the fetus.
As a result of the lower segment thinning and concomitant upper segment thickening, a boundary between the two is marked by a the physiological retraction ring.
When the thinning of the lower uterine segment is
extreme, as in obstructed labor, the ring is very prominent, forming a pathological retraction ring. This is an abnormal condition, also known as Bandl’s ring, This effect on the musculature of the lower segment and on the cervix is an important factor in cervical taken up into the lower segment and cervical dilatation.
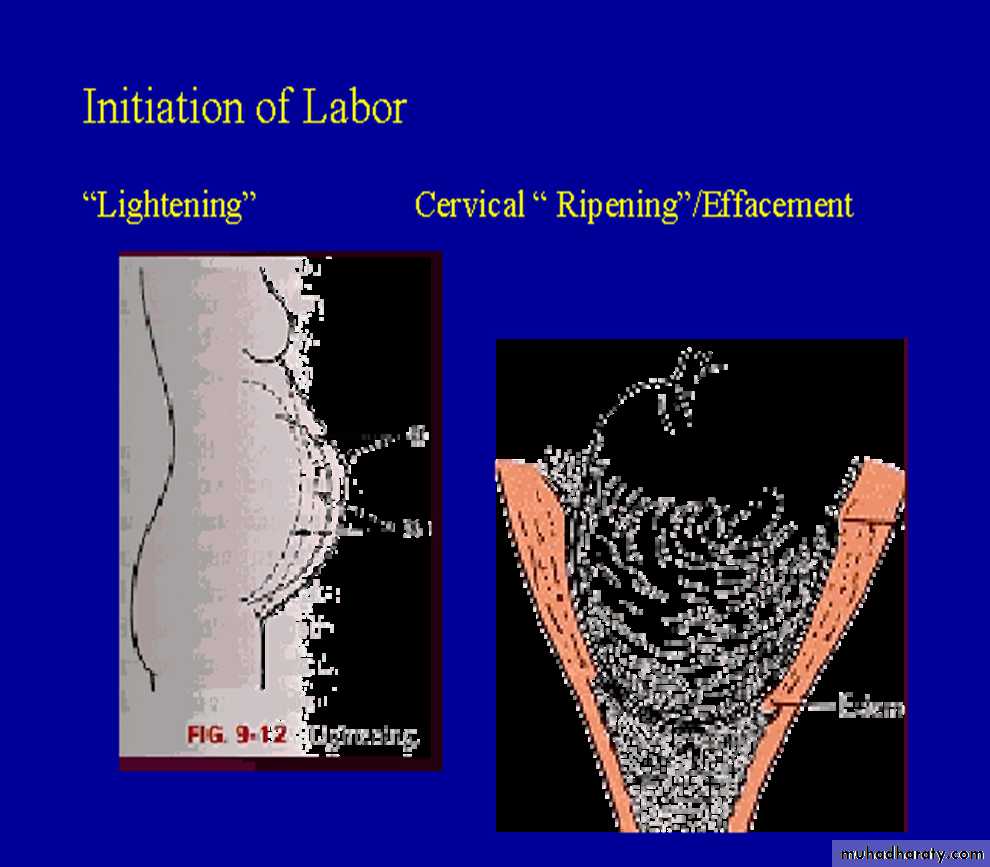
Cervical Changes:
There are three principal structural components of the cervix:
collagen, smooth muscle, and the extracellular matrix.Two complementary changes occur to its connective tissues as the cervix softens:
-increase in collagen breakdown and a rearrangement of the collagen fiber bundles.
-changes in the relative amounts of the various glycosaminoglycans, particularly hyaluronic acid, a compound associated with the capacity of the cervix to retain water.
The result of these changes:
-cervical thinning-softening
-and relaxation, which allow the cervix to initiate dilatation.
Effacement causes expulsion of the mucus plug as the cervical canal is shortened.
Fetal Descent.
In many nulliparous, engagement of the fetal head is accomplished before labor begins, and further descent does not occur until late in labor this event referred to as lightening..In others in whom engagement of the fetal head is initially not so complete, further descent occurs during the first stage of labor.
Clinical Onset of Labor.
In some women, the forceful uterine contractions that effect cervical dilatation, fetal descent, and delivery begin suddenly and seemingly without warning.
In other women, a rather dependable sign of the initiation of labor is the spontaneous discharge of a small amount of blood-tinged mucus from the vagina.
This event represents the extrusion of the mucus plug that had filled the cervical canal during pregnancy, and is referred to as "show" or "bloody show."
TRUE & FALSE LABOR
Rupture of membranes:Confirmation of rupture of membranes (ROM) may include physical examination, laboratory testing, and ultrasonography.
Vaginal Bleeding
Fetal Movement: fetal well-being must be ascertained.
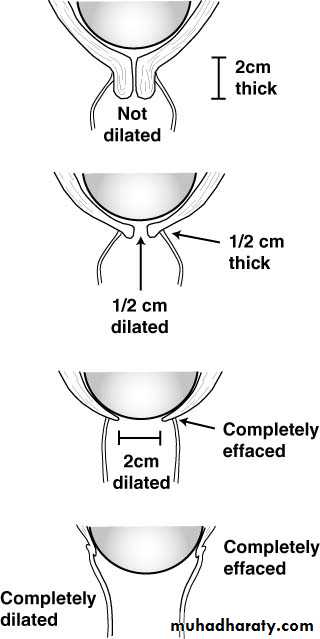
Cervical Effacement. The degree of cervical effacement usually is expressed in terms of the length of the cervical canal compared with that of an uneffaced cervix. When the length of the cervix is reduced by one half, it is 50-percent effaced.
When the cervix becomes as thin as the adjacent lower uterine segment, it is completely, or 100-percent, effaced.
Cervical Dilatation. This measurement is determined by estimating the average diameter of the cervical opening by sweeping the examining finger from the margin of the cervical opening on one side to that of the opposite side.
Position of the Cervix. The relationship of the cervical os to the fetal head is categorized as posterior, mid position, or anterior.
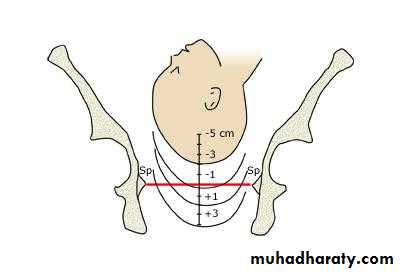
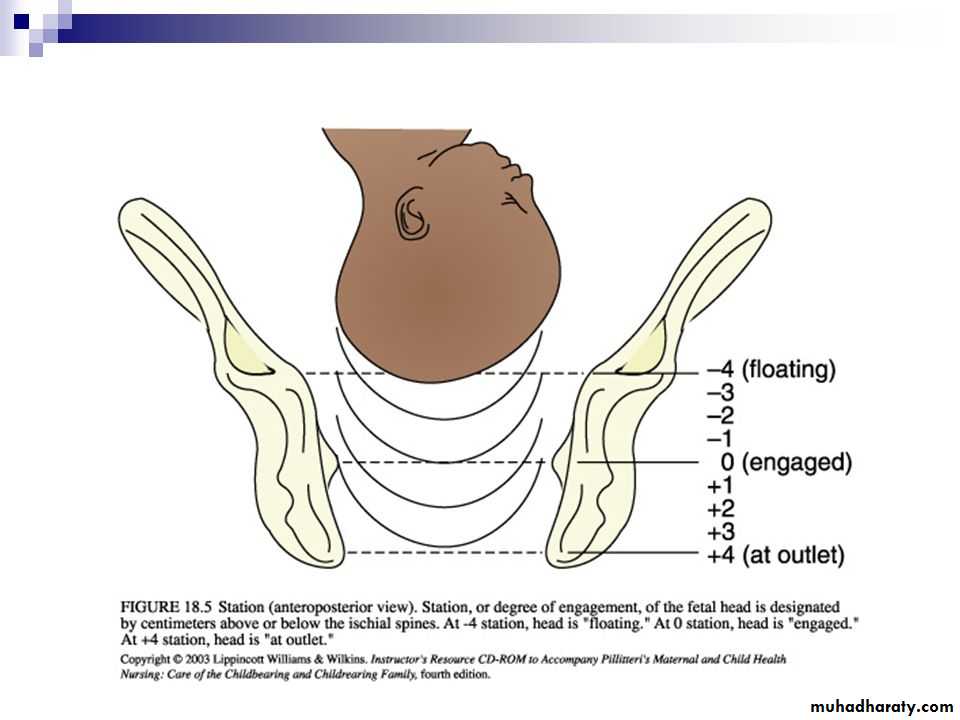
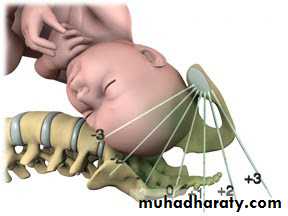
Station. The level of the presenting fetal part in the birth canal is described in relationship to the ischial spines, which are halfway between the pelvic inlet and the pelvic outlet.
Stages of Labor
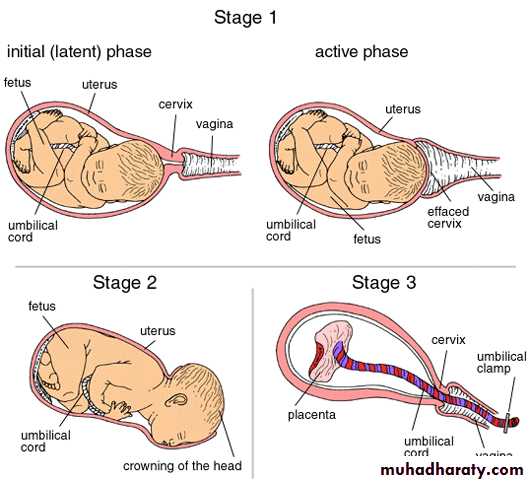
First Stage of LaborBegins when uterine contractions are of sufficient frequency, intensity and duration to bring about effacement and progressive dilatation of the cervix
Further divided into latent and active phases
Latent phase, rate of cervical dilatation is slow (up to 3cm)
Active phase, rate of dilation is about 1cm/hr in primi and up to 2 cm in multip.
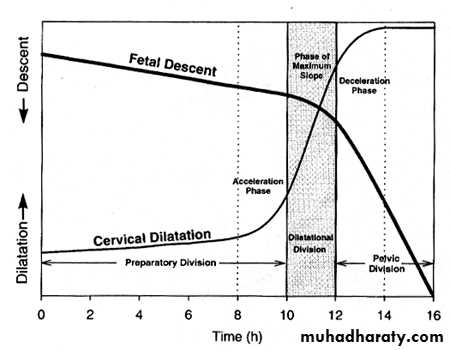
Acceleration, transition and deceleration parts refer to the rate of cervical dilation
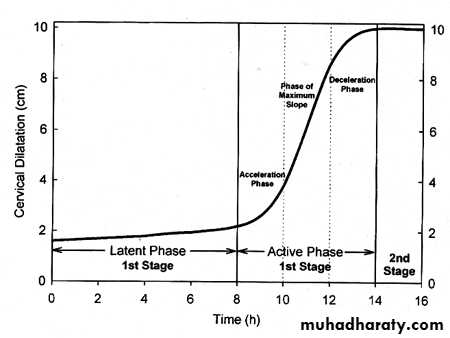
Second Stage of Labor
Begins when dilatation of the cervix is complete and ends with delivery of the fetusDuring active phase and 2nd stage, fetal head descends relative to the mother’s pelvis, noted by location of fetal head in relation to ischial spines of maternal pelvis (Friedman curve). The curve is used to predict labor arrest.
It is subdivided into two phases:
1-no maternal urge to pushSagittal suture in transverse position
2-urge to push
Sagittal suture in AP position
Third Stage of Labor
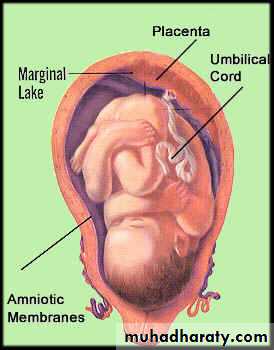
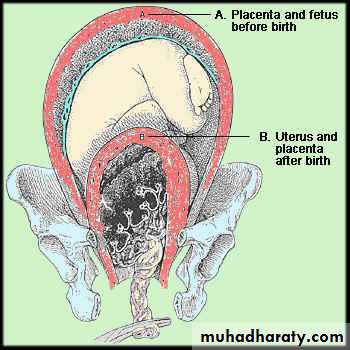
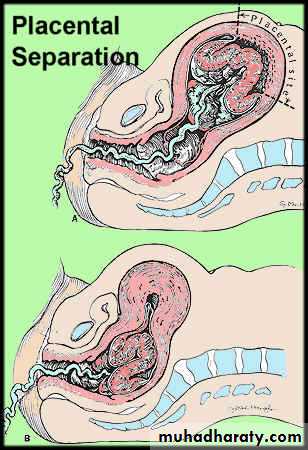
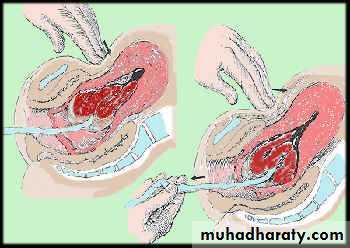
Interval between delivery of the fetus and delivery of the placentaDuring this stage the placenta separates and is expelled, typically between 5 and 30 min
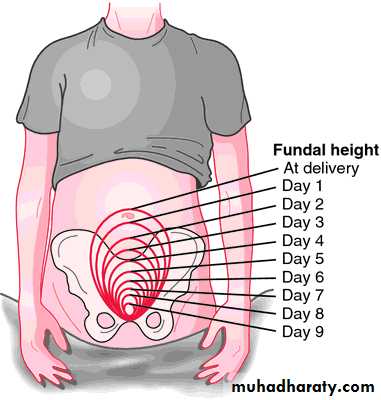
Involution
The involution state is assessed by looking at the fundal height and consistency of the uterine fundus plus the character and amount of lochia every 4-6 hours postpartum.The uterus is obviously stretched during pregnancy. Once finished with the birthing process, the fundus of the uterus may rise but them decreases in height by 1 cm per day. By one week postpartum, the fundus may no longer be palpable through the abdomen and the entire size of the uterus is about the size of a grapefruit, round and smooth but firm.
lochia
Lochia, the discharge during the first weeks following birth, indicates the process of uterine lining healing and the amount gradually decreases over time.During the first few days postpartum, a moderate amount of dark red discharge. This is called lochia rubra.
During the next few days, the lochia becomes more serous and pink and decreases in amount. This is called lochia serosa.
Finally during 7-10 days postpartum, the lochia becomes pale yellow-white and is even in a more decreased amount. This is called lochia alba and may continue for 2-3 more weeks.
Placental site healing