Cerebellum
Speech & Language
By
Dr. Mufeed Akram Taha
FIBMS Neurology
Kirkuk College of Medicine

The Cerebellum
The little brain, it helps to regulate movements
and posture, influences muscle tone, eye
movements and balance. The cerebellum is
especially vital to the control of very rapid
muscular activities such as running, typing,
playing the piano, and talking. Loss of this area
of the brain can cause almost total
incoordination of these activities even though
its loss causes no paralysis of any muscle.
Cerebellum has wide interconnections with
various parts of the NS and with the
peripheral sensory receptors.

Anatomical Functional Areas of the Cerebellum
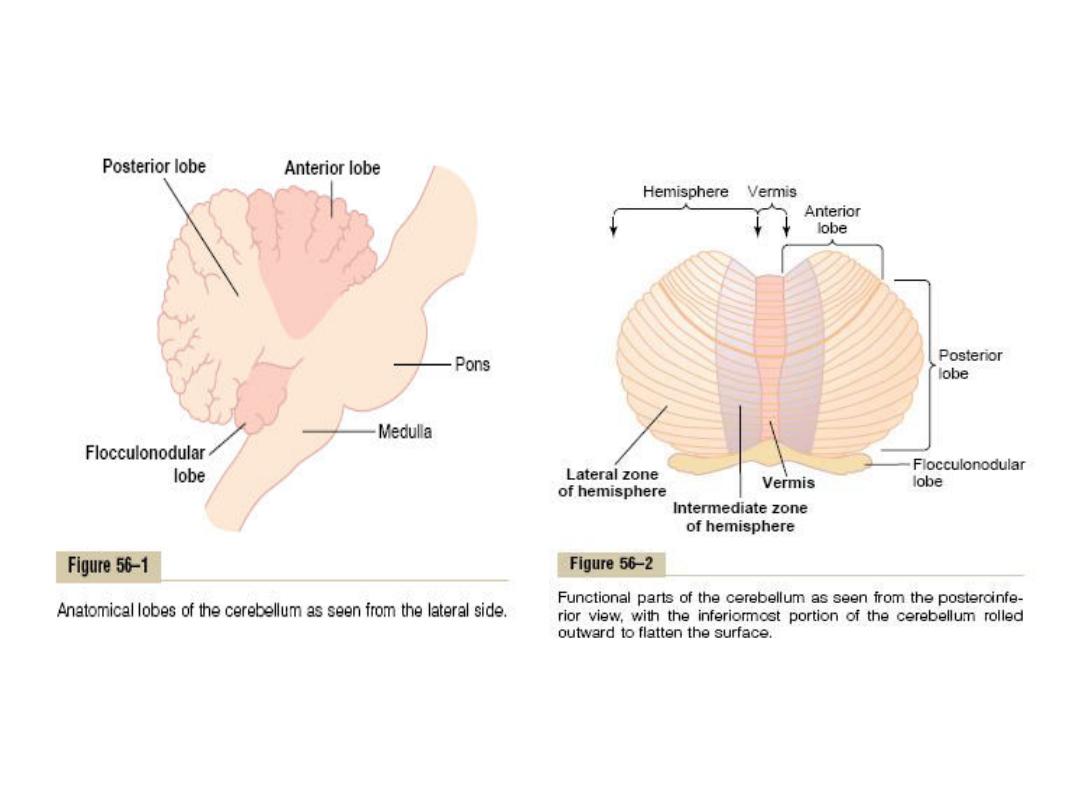
Anatomically, the cerebellum is divided into
three lobes:
(1) The anterior lobe,
(2) The posterior lobe
(3) The flocculonodular lobe. The
flocculonodular lobe is the oldest of all
portions of the cerebellum; it developed along
with (and functions with) the vestibular
system.

-The center of the cerebellum a narrow band called
the vermis, separated from the remainder of the
cerebellum by shallow grooves. In this area, most
cerebellar control functions for muscle movements
of the axial body, neck, shoulders, and hips are
located.
- Cerebellar hemisphere located on each side of the
vermis and is divided into an intermediate zone and
a lateral zone.
-The intermediate zone of the hemisphere is
concerned with controlling muscle contractions in
the distal portions of the upper and lower limbs,
especially the hands and fingers and feet and toes.

-The lateral zone of the hemisphere operates
at a much more remote level because this
area joins with the cerebral cortex in the
overall planning of sequential motor
movements.
- The axial portions of the body lie in the
vermis.
- The limbs and facial regions lie in the
intermediate zones of cerebellar
hemisphere.

The cerebellum receives information from:
[1] Spinal cord through the dorsal spinocerebellar
tracts which apprises the cerebellum of the
momentary status of dynamic and static muscle
length and muscle tension, positions and rates of
movement of the parts of the body, and forces
acting on the surfaces of the body. And the ventral
spinocerebellar tract which apprises the cerebellum
that the motor signals have indeed arrived at the
cord and it also apprises the cerebellum of the
intensity of the signals.
[2] Eyes and ears through tectocerebellar tract from
colliculi.
[3] Cerebral cortex through
corticopontocerebellar tract .Afferent fibres
from the temporal, parietal, occipital and
frontal lobes of the cerebral cortex pass
through the internal capsule and crus cerebri
and synapse in the pontine nuclei. From here,
the fibres enter the cerebellum through the
middle cerebellar peduncle and terminate in
the contralateral cerebellar hemisphere, the
largest source of mossy fibers which transmit
information about muscle movements
planned by cortex.
[4] Olivary nucleus through olivocerebellar. Afferent
fibres from the temporal, parietal, occipital and
frontal lobes of the cerebral cotrex pass through
the internal capsule and synapse in both the
ipsilateral and contralateral inferior olivary nuclei.
From here, the fibres enter the cerebellum through
the inferior cerebellar peduncle and terminate in
the contralateral cerebellar hemisphere. This tract
is the sole source of climbing fibers.
[5] Cuneate nucleus through cuneocerebellar tract
which transmite the same information as dorsal
spinocerebellar tract but from neck and upper
limbs.

[6] Vestibular nucleus through vestibulocerebellar
tract.
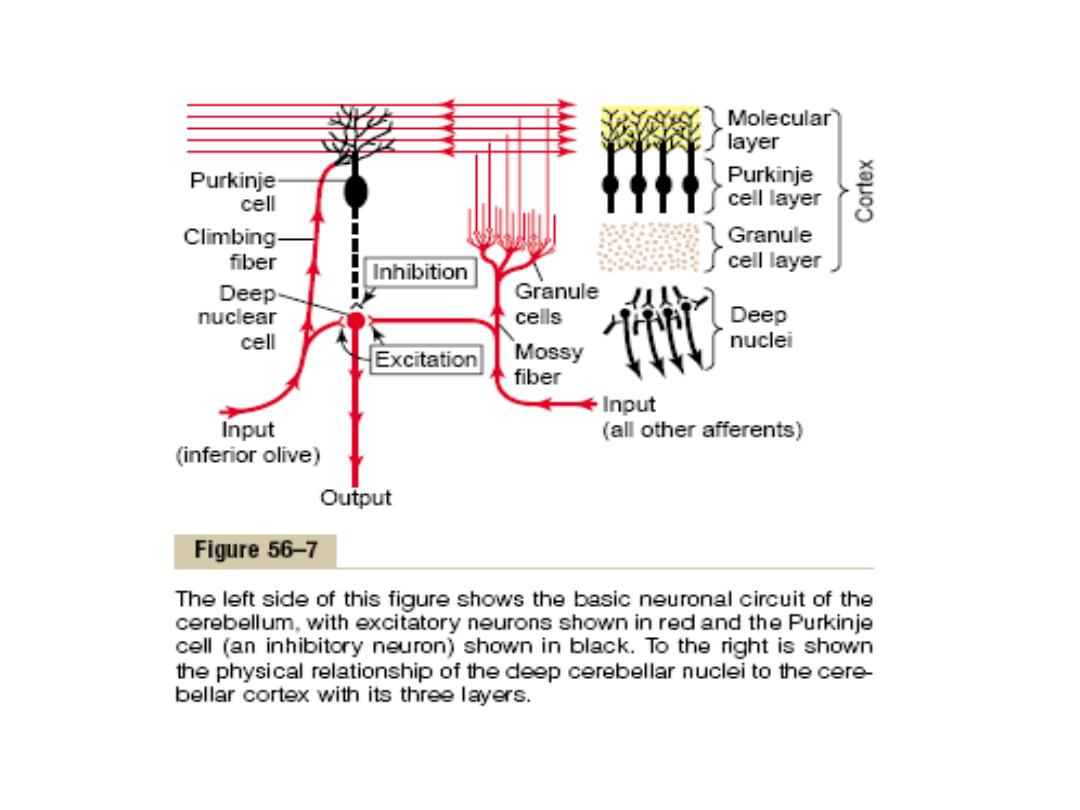
The ingoing pathways to the cerebellum arranged
into two main input fibers that pass to the
cerebellar cortex and these are climbing fibers
(originated from inferior olive of the medulla)
and mossy fibers (originated from many centers
in the brain stem and spinal cord). Both are
excitatory which send collaterals to the deep
nuclei and pass to the cortex

The cerebellum has two important structures:
[1]. External cerebellar cortex seperated by white
matter from the deep cerebellar nuclei.
The cerebellar cortex contains only 5 types of
neurons; Purkinje, granule, basket, stellete, and
Golgi cells. The axons of the Purkinje cells are
inhibitory (the neurotransmitter is gamma amino
butyric acid, GABA) and are the only output from
the cerebellar cortex pass to the deep nuclei. The
granule cells (excitatory cell) receive input from the
mossy fibers and send their bifurcated axons (called
parallel fibers) to synapse with other cells at the
cerebellar cortex.

The stellate and basket cells are inhibitory
interneurons, which synapse with purkinje cells.
Golgi cells are inhibitory interneurons, which
receive input from parallel fibers and from mossy
fibers and from Purkinje cells and send their
inhibitory axons synapse with granule cells.
[2]. Deep cerebellar nuclei which are dentate,
globose, emboliform, and fastigiel nuclei. Deep
nuclei receive excitatory inputs from the mossy
and climbing and inhibitory inputs from Purkinje
cells. The output of the deep cerebellar nuclei to
the brain stem and thalamus is always excitatory.
Therefore, almost all the cerebellar circuit seems
to be concerned solely with modulating or timing
the rate of excitatory output of the deep cerebellar
nuclei to the brain stem and thalamus.

The special features of the cerebellar neuronal
circuit are:
[1] There are no reverberatory pathways in the
cerebellar neuronal circuits, so that the input-
output signals are very rapid and never persist for
long periods of time.
[2] Another special feature is that many of the cells
of the cerebellum are constantly active, and the
deep nuclear cells continually send output signals
to the other areas of the motor system. A
decrease of the nuclear cell firing rate can
provide an inhibitory output signal from the
cerebellum while an increase in firing rate can
provide an excitatory output signal.

[3] All cerebellar cortical cells are inhibitory
except the granule cells which are excitatory.
[4] The climbing fiber inputs exert a strong
excitatory effect on single Purkinje cell
whereas mossy fiber inputs exert a weak
excitatory effect on many Purkinje cells via
the granule cells in addition to excitation of
other cells (basket and stellate cells which are
inhibitory to Purkinje cells, and Golgi cells
which inhibit the transmission from mossy
fibers to granule cells).

The main functions of cerebellum
1 - Planning, programming and timing of sequential
pattern of the motor activities. Cerebellum in
association with motor and sensory cortex and
basal ganglia are planning, programming and timing
for the next movement at the same time that the
present movement is occurring.
In cerebellar dysfunction, this capability is seriously
disturbed especially for rapid movements, which
can lead to extreme incoordination and failure of
progression of the purposeful movements of the
hands, fingers and feet a condition called
Dysdiadochokinesia in which jumbled movements
occur instead of normal coordinated movements in
addition, speech is affected, a condition called
dysarthria.

2
— Monitors, compare, and makes corrective
adjustments in the motor activities elicited by other
parts of the brain.
3
— The cerebellum functions with the spinal cord and
brain stem to control postural and equilibrium
movements. Cerebellum is especially important in
controlling the balance between agonist and
antagonist muscle contractions during rapid
changes in body positions as dictated by the
vestibular apparatuses. this is achieved by the
predictive function of the cerebellum who analyzes
the information dictated from peripheral sensory
receptors

(especially from the muscles. Joints, and skin surface)
and vestibular nuclei about the rate and direction
of movement of each part of the body and
compute these information to predict the position
of these parts of the body within the next 15-20
msec and therefore, provide almost instantaneous
correction of postural motor signals as necessary
for maintaining equilibrium even during extremely
rapid motion, including rapidly changing directions
of motion.
Cerebellar dysfunction causes extreme disturbance of
equilibrium during performance of rapid motions
than during stasis.

4
— Cerebellar control of the muscle spindles: Cerebellum
receives extreme amount of information from the
muscle spindles via the dorsal spinocerebellar tracts.
Inturn, from cerebellum, signals are transmitted into the
brain stem and motor cortex to stimulate the gamma
efferent fibers that innervate the muscle spindles
themselves. This pattern of arrangement forms a
cerebellar stretch reflex or negative stretch reflex.
When the muscle is already contracted, any sudden
release of the load on the muscle that allows it to
shorten will elicit reflex muscle inhibition rather than
reflex excitation to oppose the shortening of the muscle
in the same way that the positive stretch reflex opposes
lengthening of the muscle.

Loss of the cerebellar component of the stretch reflex
will result to an effect called rebound in which, if a
person with cerebellar disease is asked, to pull
upward strongly on an arm while the physician
holds it back at first and then lets go, the arm will fly
back until it strikes the face instead of being
automatically stopped.
5- Cerebellum also plays a role in predicting other
events besides movements of the body. For
instance, the rates of progression of both auditory
and visual phenomena can be predicted.
An example, a person can predict from the changing
visual scene how rapidly he is approaching an
object.

6- Control of ballistic movements. Many rapid
movements of the body, such as the movements
of the fingers in typing, the movements of the
eyes when reading or when looking at successive
points along a road when a person is moving in a
car where the eyes jump from one position to
the next. These movements occur so rapidly that
it is not possible to receive feedback information
either from the periphery to the cerebellum or
from the cerebellum back to the motor cortex
before the movements, are over. These
movements are called ballistic movement.

Cerebellar lesions
1- Incoordination of movements:
*Like gait ataxia, dysmetria (inability to reach a target smoothly).
*Intention tremor: tremor on approaching the target
*Dysdiadochokinesia: difficulty in performing rapid repeatitive
movements of the limbs like typing.
2- Loss of muscle tone (Hypotonia):
This occur when the lesion involve the deep cerebllar nuclei, because
discharge from these are have excitatory effect on other motor area.
3- Nystagmus:
Mean oscillation of the eye ball usually laterally but may be rotatory. It is
due to to defect in postural fixation of the eye movement.
4- Speech defect:
This generally take the from of dysarthric speech in which each syllable is
pronounced as through it was a word.

Speech and Language
Language and Speech are Coordinated in
Specific areas of Association Cortex:
The ability to communicate by language, verbally
and in writing, is one of the most difficult
Cognitive functions to study because only
humans are capable of these skills. Thus, our
knowledge of language processing in the brain
has been inferred from clinical data by
studying patients with aphasias (disturbances
in producing or understanding the meaning of
words) following brain injury, surgery, or other
damage to the cerebral cortex.

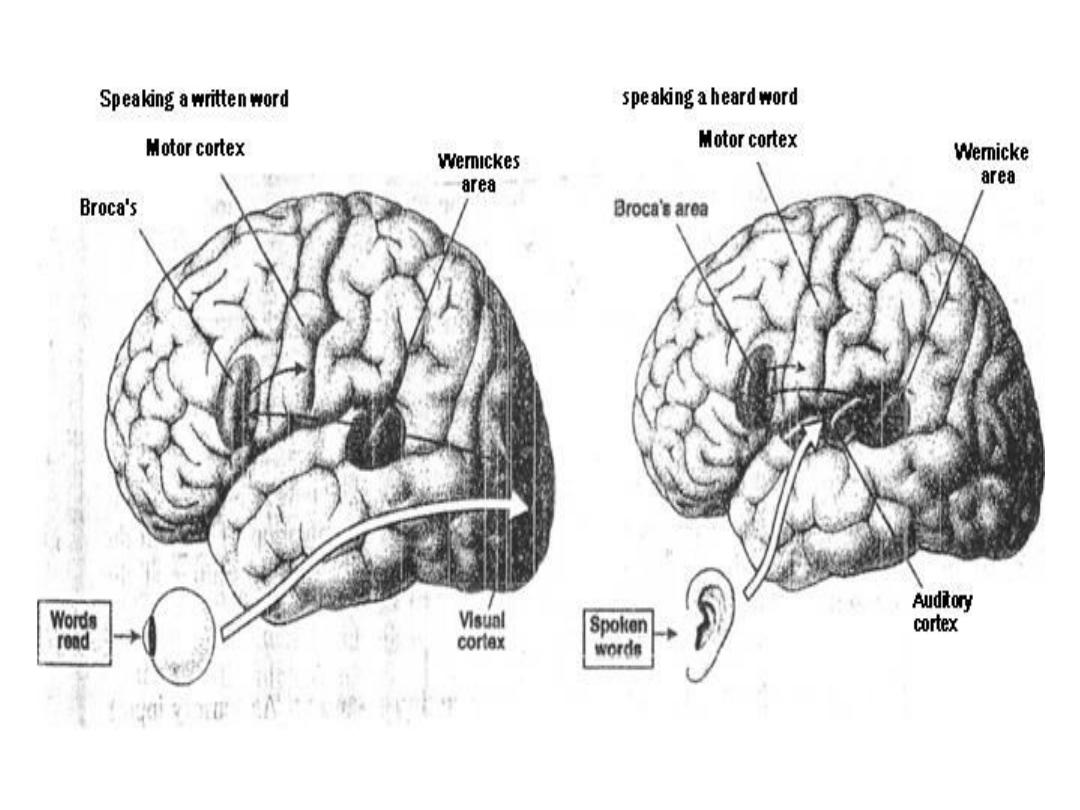
Two areas appear to play an important role in
language and speech:
Wernicke's area in the upper temporal lobe, and
Broca's area in the frontal lobe, Both of these areas
are located in association cortex adjacent to cortical
areas that are essential in language communication.
Wernicke's area is in the parietal-temporal-occipital
association cortex, a major association area for
processing sensory information from the somatic
sensory, visual and auditory cortices. Broca's area is
in the prefrontal association cortex adjacent to the
portion of the motor cortex that regulates
movement of the muscles of the mouth, tongue and
throat (i.e. the structures used in the mechanical

Production of speech). A fiber tract, the arcuate
fasciculus, connects Wernicke's area with Broca's
area to coordinate aspects of understanding and
executing speech and language skills. Clinical
evidence indicates that Wernicke's area is essential
for comprehension, recognition, and construction of
words and language, whereas Broca's area is
essential for the mechanical production of speech.
Patients with a defect in Broca's area show evidence
of comprehending a spoken or written word but
they are not able to say the word. In contrast,
patients with damage in Wernicke's area can
produce speech, but the words they puts together
have little meaning.
Thank you