Unit 2: Bacteriology
114
Lecture 6 – Campylobacters &
Helicobacter
Campylobacters (Campylobacter spp.)
Found in animals (including domesticated) cause both
diarrheal & systemic diseases (wide spread of infections in
the world). The most important Spp.:
1. Campylobacter jejuni: 2. C. coli :
Common human pathogens (as common as Salmonella &
Shigella), are causing enteritis & systemic infection.
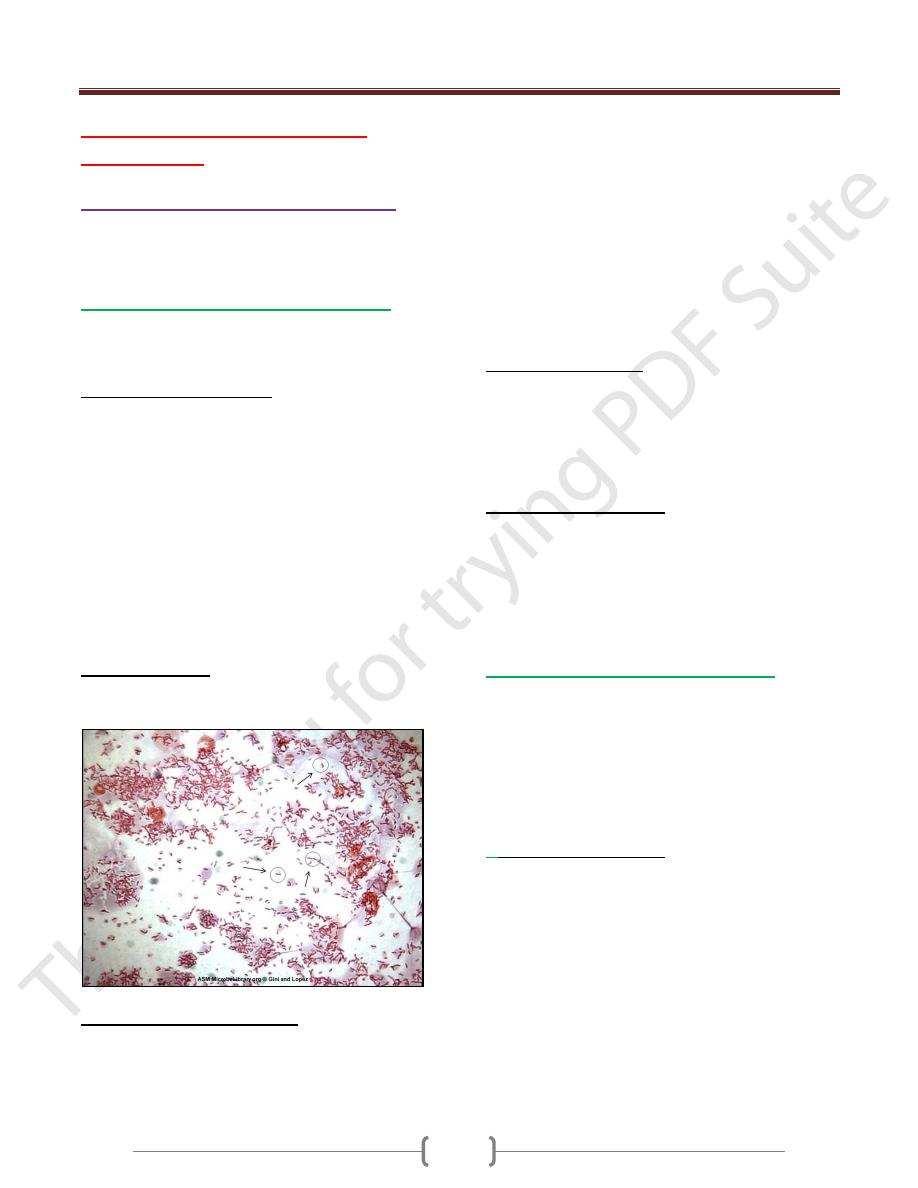
Morphology & Identification:
G – rods with comma, S, or gull-wing shapes, motile with
single polar flagellum.
Culture: selective media are needed (Skirrow’s medium &
Campy-Bac medium), in atmosphere 5% O
2
+10% CO
2
(by
using anaerobic jar with gas generating pack), temperature
42 C˚(inhibit most bacteria found in stool.
The colonies colorless or gray, may be watery & spreading
or round & convex (these 2 colonies types may appear on
one plate), oxidase + & catalase +, not ferment or oxidize
carbohydrates, nitrate reduction, H
2
S production. For
further identification of species hippurate test &
antimicrobial susceptibility test can be used.
Antigenic structure:
Have LPS with endotoxic activity.-Cytopathic extracellular
toxins & enterotoxins (not well defined).
Pathogenesis & Clinical Findings:
The infection due the oral route from food, drink, or contact
with infected animals or its products.
C.jejuni is susceptible to gastric acid (10
4
organisms is
necessary).
The organism multiplies in the small intestine, invade the
epithelium & produce inflammation that results in the
appearance of red & white blood cells in the stool (may
invade the bloodstream). Localized tissue invasion with the
toxic activity, responsible for the enteritis.
Acute crampy abdominal pain, diarrhea (may be bloody),
headache, malaise & fever. The illness is self-limited to 5-8
days (may be longer). May resolve without antimicrobial
therapy.
Therapy shortens the duration of fecal shedding of bacteria.
C.jejuni is susceptible to erythromycin.
Diagnostic Lab. Tests:
Specimens: Diarrheal stool.
Smear: Gram-stained smears of stool→ gull-wing shaped.
Dark-field or phase contrast microscopy → darting motility
of this bacterium.
Culture: Selective media is the definitive test.
Epidemiology & Control:
Campylobacter enteritis resembles other acute bacterial
diarrheas (Sh. dysenteriae).The source of infection, food
(milk) or contact with infected animals or humans & their
excreta.
Outbreaks from a common source (unpasteurized milk).
Require puplic health control measures.
3. Campylobacter fetus subspecies fetus:
Opportunistic pathogen cause systemic infection in
immunocompromised patiens.The portal of entry
G.I.T→bacteremia & systemic infection (may be
diarrhea).Have a surface array proteins(S protein),which
form a capsule-like structure on the surface of the
organism, correlated with the ability of the bacteria to
cause bacteremia.
4.
Other campylobacters:
C.lari
(in seagulls) &
C.upsaliensis
(in dogs), both causes
diarrhea in humans.
Unit 2: Bacteriology
115
Helicobacter pylori
Antral gastritis, duodenal (peptic) ulcer disease, gastric
ulcers & gastric carcinoma.
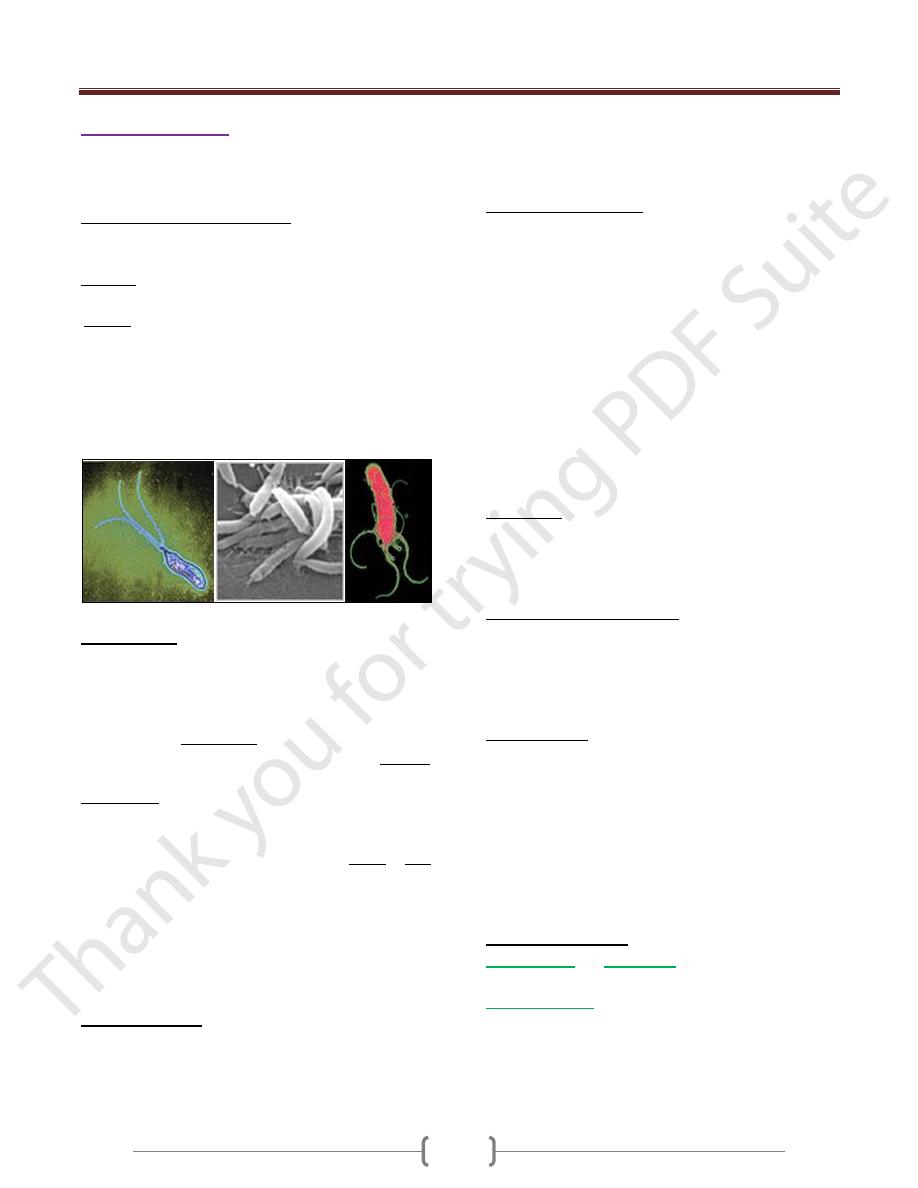
Morphology & Identification:
Spiral-shaped or curved G-rods has multiple flagella at one
pole (actively motile).
Culture: grows in (3-6) days at 37C˚ in microaerophilic as
C.jejuni .
Media:
1) Skirrow’s media
2) Chocolate media.
3) Other selective media with vancomycin, nalidixic acid, &
amphotericin.
The colonies are translucent & small (1-2 mm in diameter),
Oxidase +, Catalase + & strong producer of urease.
Pathogenesis:
H.pylori found deep in the mucus layer near the epithelial
surface (at pH 6-7 because gastric mucus is relatively
impermeable to acid & has buffering capacity, on the lumen
side the pH is low 1-2, while on the epithelial side the pH is
high 6-7) & it is quite motile even in mucus able to find its
way to the epithelial surface. H.pylori produces a protease,
which reduces the ability of acid to diffuse & production of
active urease, which release ammonia & that cause further
buffering of acid.
H.pylori causes gastritis & hypochlorhydria & duodenal
ulceration-→ invade the epithelial cells also toxins & LPS
& ammonia → damage the mucosal cells (antimicrobial
therapy → clearing bacteria & improvement of gastritis &
duodenal ulcer).
Destruction of the epithelium is common, and glandular
atrophy may occur, H.pylori thus may be a major risk factor
for gastric cancer
Clinical findings:
Acute infection of upper gastrointestinal illness with nausea
& pain, vomiting & fever (duration less than 1-2 weeks).
This bacterium may persist for years, decades or even a
lifetime.
90% of patients with duodenal ulcers & 50-60% of gastric
ulcers have H.pylori infection. It may have a role in gastric
carcinoma & lymphoma.
Diagnostic Lab. Tests:
Specimens: Gastric biopsy(gastroscopy) → histological
exam. & culture.
Blood → determination serum antibodies.
Smear: Biopsy stained by Giemsa stain→ curved or
spiraled organisms.
Culture: Selective & differential media.
Serology: The role of Abs tested is limited (serums Abs
can persist even if the infection eradicated).
Detection of H.pylori Ags in stool, a test of cure.
Special rapid test: to detect urease activity in biopsy
material or in vivo by
13
C- or
14
C-labeled urea ingested by
the patient & then detection of labeled CO
2
in the patient’s
exhaled breath.
Immunity:
Patients infected develops IgM, subsequently, IgG & IgA
(persist systemically & at the mucosa in high titer in
chronically infected persons).
Treatment: Triple therapy:
Metronidazole + bismuth subsalicylate or bismuth
subcitrate +amoxicillin or tetracycline for 14 days.
Proton pump inhibitor + amoxicillin & calithromycin or
amoxicillin + metronidazole.
Epidemiology:
Acute epidemic gastritis is a common source for H.pylori.
Transmission of H.pylori by person-person & intrafamilial
culstring of infection.
H.pylori is present on the gastric mucosa of less than 20%
of persons under age 30, 40-60% of persons age 60
(including asymptomatic).
In developing countries, the prevalence of infection may be
80% or higher.
Other Helicobacters
H. fennelliae
and
H. cinaedi
can cause either diarrheal
or extraintestinal disease.
Arcobacter spp
. Are uncommon enteric pathogens.