Unit 2: Bacteriology
131
Lecture 14 – Mycoplasma,
Chlamydia & Rickettsiae
Mycoplasmas (Mycoplasmas spp)
Mycoplasmas are groups of small, wall-less organisms.
They are the smallest free-living organisms (0.3μm in
diameter).
Important properties:
1) Mycoplasmas stain poorly with Gram stain.
2) The outer surface is a flexible three layer cell membrane;
hence the organisms can assume a variety of shapes.
3) It contain cholesterol in their bacterial membrane.
4) The colony frequently has a characteristic (fried egg)
shape, with a raised center & a thinner outer edge.
In human there are four important species:
1) Mycoplasma pneumoniae 2) M. Hominis
3) M. Genitalium 4) Ureaplasma urealyticum
Pathogenesis:
Pathogenic Mycoplasmas have flask-like or filamentous
shapes & have specialized polar tip structures that
mediate the adherence to host cells (ciliated & non
ciliated cells).
1) M. pneumoniae
Is transmitted from person to person by means of infected
respiratory secretions & cause atypical pneumonia. May
be ranged from asymptomatic infection to serious
pneumonitis.
Incubation period 1-3 weeks.
Symptoms:
Fever, headache, sore throat, & cough which is non-
productive .Complications are uncommon, but sometimes
hemolytic anemia, meningitis & pericarditis may occur
Diagnosis:
Culture: haert infusion peptone broth (with 2% agar &
30% human ascitic fluid or animal serum, pH 7.8).
Complement fixation (cf test).
Cold hemagglutination (at 4C
°
). After 3-4 weeks, titer of
1:128 or higher is an indicative of recent infection.
ELISA.
Treatment: Tetracycline & erythromycin.
2)
Mycoplasma hominis
: causes infections of uterine
tubes (salpingitis) & tubo-ovarian abscesses (in Women).
3)
Mycoplasma genitalium
: Associated with some
infections of chronic nongonococcal urethritis (in men).
4)
Ureaplasma urealiticum
: causes nongonococcal
urethritis in some men (may play role in male infertility).
Lung diseases in premature low birth-weight infants
(acquired during birth).
Cell Wall-defective Bacteria
L phase variants (L forms):
Are wall-defective bacteria that can replicate serially as
non-rigid cells & produce colonies on solid media.
Some of L phase variants are stable; others are unstable &
revert to bacterial parental forms .Wall-defective forms
are not genetically related to Mycoplasma.
Cell wall-defective bacteria result from:
Spotaneous mutation.
Effect of chemicals: penicillin & lysozyme.
They are important for the persistence of bacteria in
tissues & recurrence of infection after antimicrobial
treatment, as in causes of endocarditis.
Types of cell wall-defective bacteria:
1) Protoplast:
forms usually derived from G-positive
bacteria osmotically fragile.
2) Spheroplast
: forms usually derived from G-negative
bacteria (they retain some outer membrane material).
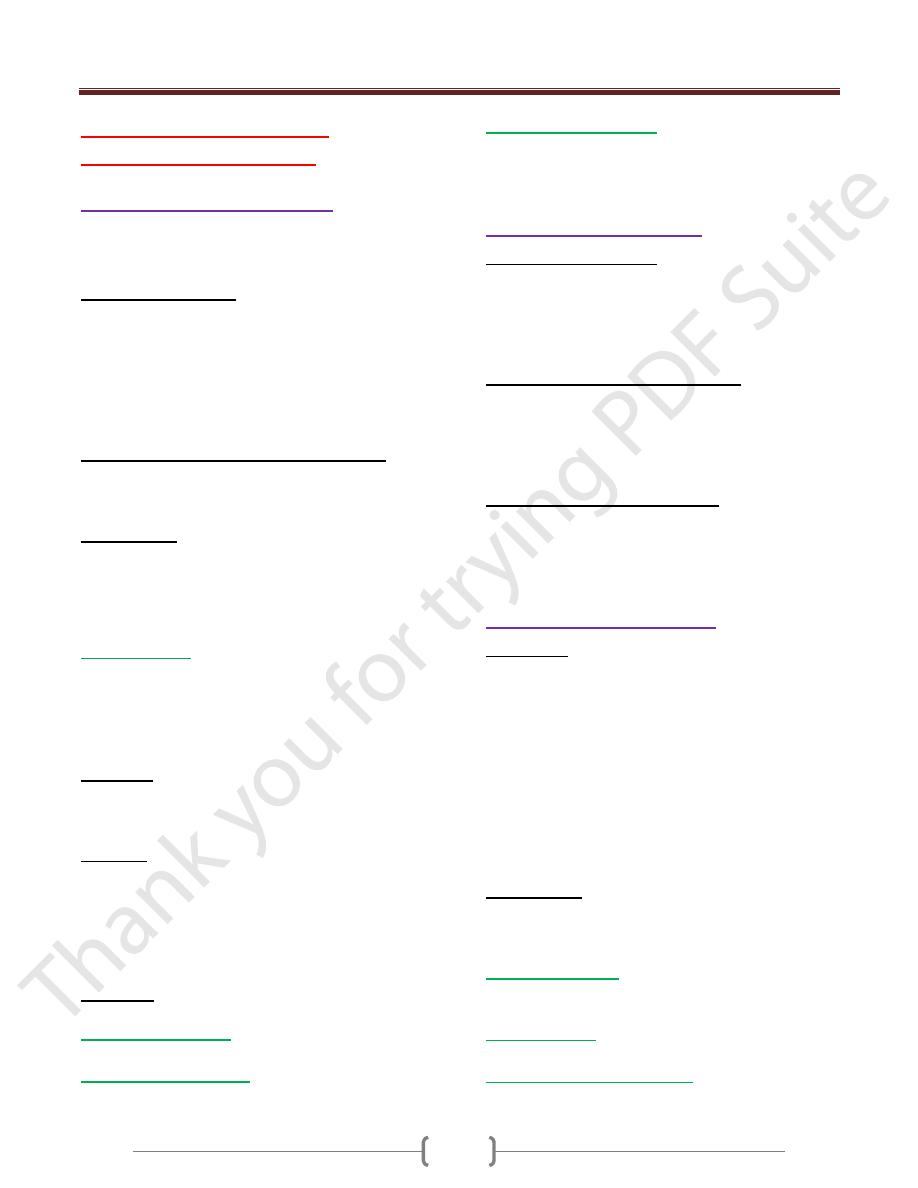
Chlamydiae (Chlamydia spp.)
Chlamydiae: are obligate intracellular bacteria, luck the
ability to produce sufficient energy to grow independently
& therefore can grow only inside host cell. Chlamydiae
have a replicative cycle different from that of all other
bacteria. Within cells site of replication appears as an
inclusion body, which can be stained & visualized
microscopically. These inclusions are useful in the
identification of these organisms in the clinical laboratory.
They have rigid cell wall but they don’t have typical
peptidoglycan. Their cell walls resemble those of G-
negative but luck muramic acid.
Pathogenesis:
Chlamydiae infect primarily epithelial cells of the mucous
membrane and the lungs.
Diseases:
1)
Chlamydia psittaci
: infects the lungs →human
psittacosis, this disease may be asymptomatic or produce
high fever & pneumonia.
2)
C. pneumoniae
→upper & lower respiratory tract
infections especially bronchitis & pneumonia.
3)
C. trachomitis types A, B&C
→trachoma (chronic
conjunctivitis endemic in Africa & Asia).
Unit 2: Bacteriology
132
Trachoma may recur over many years & may lead to
blindness but without systemic illness.
4)
C. trachomatis types D-K
→genital tract infections, which occasionally transmitted
to the eyes or the respiratory tract.
In men: it common cause of non-gonococcal urethritis,
which may progress to epididymitis, prostatitis or proctitis
In women: cervictitis develops & may progress to
salpingitis & pelvic inflammatory disease →this may
result infertility or ectopic pregnancy.
Infants borne to infected mothers often develop
mucopurulent eye infections (neonatal inclusion
conjunctivitis) 7-12 days after delivery. Some develop
chlamydial pneumonitis 2-12 weeks after birth.
C. trachomitis L1-L3 immunotypes
→lymphogranuloma venereum ,a sexually transmitted
disease with lesions on genitalian & in lymph nodes .
Diagnosis:
Group-specific Ag. (lipopolysaccharide) → complement
fixation test.
Species-specific & immunotype–specific Ag. (Protein)→
Immunofluorescence test .
Chlamydiae form cytoplasmic inclusions →stain with
Giemsa →immunofluorescence test .
Treatment:
Tetracyclines such as doxycycline & macrolides,such as
erythromycin & azithromycin .
Figure 17.2
Structural features of
Chlamydia.
A. Schematic drawing
B. Electron micrograph
Unit 2: Bacteriology
133
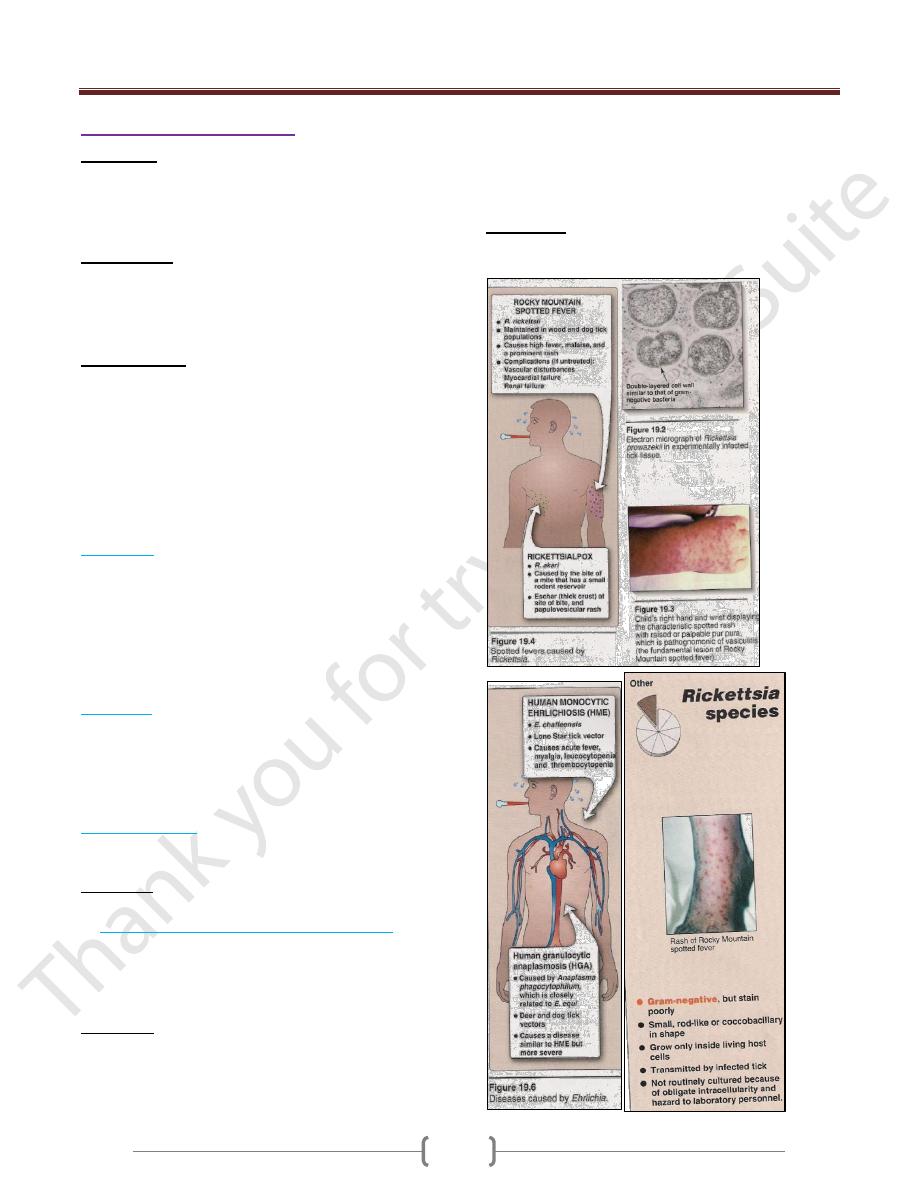
Rickettsiae (Rickettsia spp.)
Rickettsiae: are small obligate intracellular bacteria (they
are unable to produce suffecint energy to replicate
extracellular). They transmitted by the bite of the
arthropods (except for Q fever from cattle, sheep & goats).
Morphology:
Rickettsiae are pleomorphic ,coccobacilli ,gram-negative.
They are visible under light microscope when stained
with Giemsa's stain (purple).
Pathogenesis:
The human pathogens include: Rickettsia, Coxiella,
Orientia,& Ehrlichia.
The typical lesions caused by rickettsiae are a
vasculitis, particularly in the endothelial lining of the
vessel wall where the organism is found. Damage to the
vessels of the skin result →rash & hemorrhage caused by
increased capillary permeability (endotoxin?).
There are four important rickettsial diseases:
A) Typhus:
There are several forms of typhus: epidemic, endemic
(Rickettsia typhi by flea from rodents) & scrub typhus
(Orientia by mite from rodents).
Symptoms: Chills, fever, headache & influenza like
symptom
Louse bite →macular rash on the trunk →spread
peripherally →sever meningoencephalitis.
B) Q fever:
Caused by Coxiella burnetii. The main organ involved in
Q fever is lungs.
Symptoms: fever, severe headache, cough & other
influenza like Symptoms & pneumonia .Combination of
pneumonia & hepatitis should be suggested in Q fever.
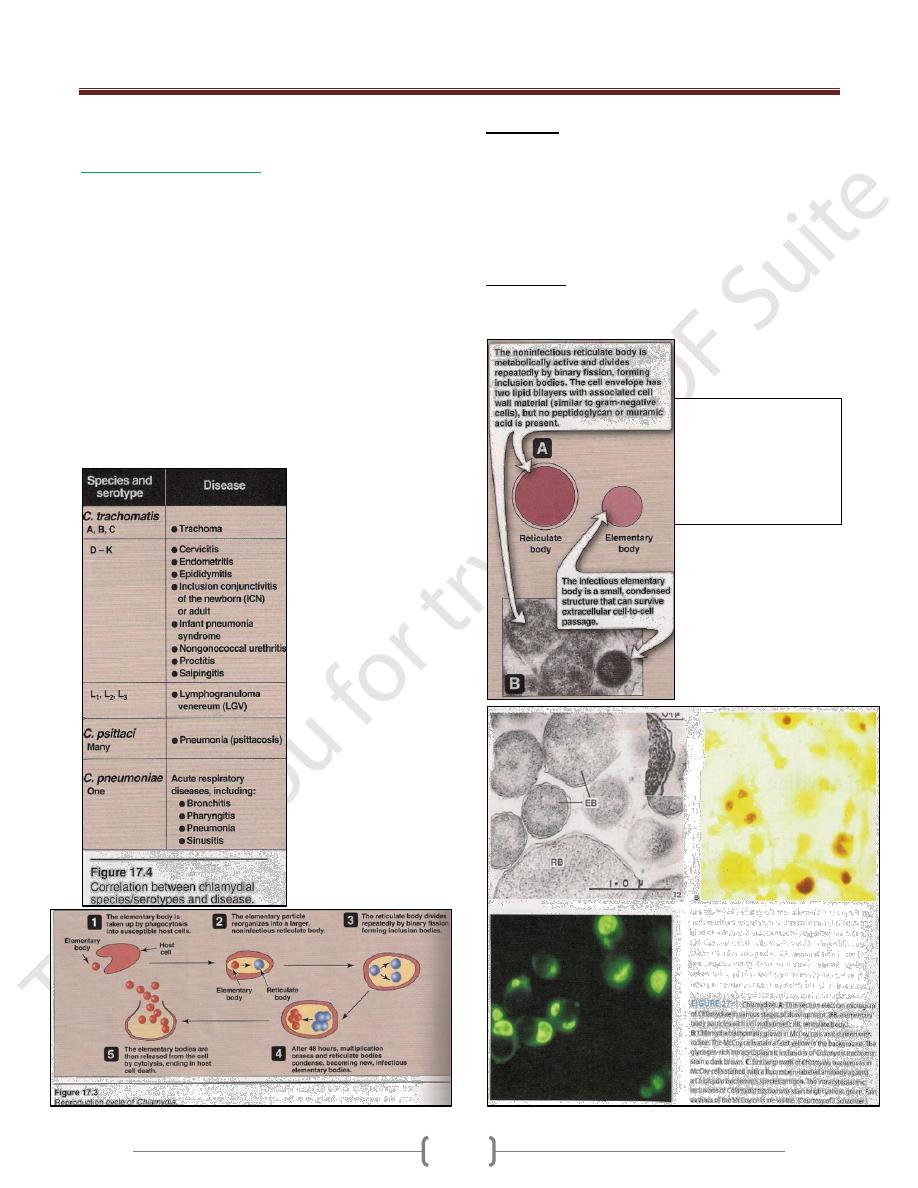
C) Spotted fevers:
1) Rocky Mountain spotted fever caused by R. rickettsii
2) Rickettsial pox caused by R. akari
Symptoms: Typical rash, which appears 2-6 days, later
begins with macules & progress to petechia.
D) Human monocyte or granulocyte ehrlichiosis:
Caused by Ehrlichia transmitted by tick from dear, dogs,
mice & other mammals.
Symptoms: Fever, headache and atypical WBC's.
Diagnosis:
Rickettsiae can be growing in cell culture or
emberyonated eggs; this is hazardous procedure that is not
available in all laboratories.
Serological test: Weil-Felix, this test is based on the
cross-reaction of an Ag present in many rickettsiae with
the O Ag polysaccharide found in Proteus vulgaris (OX-
2, OX-19 & OX-K).
Treatment:
Tetracycline &chloramphenicol as a second choice.