Unit 2: Bacteriology
80
Lecture 2 - Streptococcus and
Enterococcus
Streptococci are round to oval, Gram-positive,
nonmotile, nonsporing bacteria that form winding chains
(streptos [greek] = twisted) or diplococci. They do not
produce catalase. Most are components of the normal
flora of the mucosa. Some can cause infections in humans
and animals.
Classification.
The genera Streptococcus and Enterococcus comprise a
large number of species.
α
-, β-, ƴ-hemolysis.
Alpha-hemolysis
(
α-hemolysis). Colonies on blood agar
are surrounded by a green zone. This “greening” is
caused by H2O2, which converts hemoglobin into
methemoglobin.
Beta-hemolysis (β-hemolysis). Colonies on blood agar
are surrounded by a large, yellowish hemolytic zone in
which no more intact erythrocytes are present and the
hemoglobin is decomposed.
Nonhemolytic colonies have been termed gamma-
hemolytic
(
ƴ-hemolysis) .This (illogical) term indicates
the absence of macroscopically visible hemolytic zones.
Lancefield groups.
Many streptococci and enterococci have a polymeric
carbohydrate (C substance) in their cell walls called the
Lancefield antigen.They are classified in Lancefield
groups A-V based on variations in the antigenicity of this
antigen. Group A streptococci are nearly always beta-
hemolytic; related Group B can manifest alpha, beta or
gamma hemolysis. Most strains of S. pneumoniae are
alpha-hemolytic but can cause ß-hemolysis during
anaerobic incubation. Most of the oral streptococci and
enterococci are non-hemolytic. The property of hemolysis
is not very reliable for the absolute identification of
streptococci, but it is widely used in rapid screens for
identification of S. pyogenes and S. pneumoniae.
Streptococcus pyogenes (A Streptococci)
Morphology and culturing.
Gram-positive, round-to-ovoid cocci, 0.6-1.0
micrometer in diameter. Streptococci divide in one plane
and thus occur in pairs or (especially in liquid media or
clinical material ) in chains of varying lengths. The
metabolism of S. pyogenes is fermentative; the organism
is a catalase-negative aerotolerant anaerobe (facultative
anaerobe), and requires enriched medium containing
blood in order to grow. Group A streptococci typically
have a capsule composed of hyaluronic acid and exhibit
beta (clear) hemolysis on blood agar.
Fine structure.
The murein layer of the cell wall is followed by the
serogroup A carbohydrate layer, which consists of C
substance and is covalently bound to the murein. Long,
twisted protein threads that extend outward are anchored
in the cell wall murein: the M protein. A streptococci are
classified in serovars with characteristic M protein
chemistry. Like the hyaluronic acid capsules seen in some
strains, the M protein has an antiphagocytic effect.
The
surface of Streptococcus pyogenes is incredibly complex
and chemically-diverse. Antigenic components
include capsular polysaccharide (C-substance), cell
wall peptidoglycan and lipoteichoic acid (LTA), and a
variety of surface proteins, including M protein, fimbrial
proteins, fibronectin-binding proteins, (e.g. Protein F)
and cell-bound streptokinase.
The cytoplasmic
membrane of S. pyogenes contains some antigens similar
to those of human cardiac, skeletal, and smooth muscle,
heart valve fibroblasts, and neuronal tissues, resulting
in molecular mimicry and a tolerant or suppressed
immune response by the host.
Extracellular toxins and enzymes
.
The most important in the context of pathogenicity are:
1) Streptolysin O, streptolysin S. Destroy the membranes
of erythrocytes and other cells.
Streptolysin S is an
oxygen-stable leukocidin; Streptolysin O is an oxygen-
labile leukocidin. Streptolysin O acts as an antigen. Past
infections can be detected by measuring the antibodies to
this toxin (antistreptolysin titer).
2) Pyrogenic streptococcal exotoxins (PSE) A, B, C.
Responsible for fever, scarlet fever exanthem and
enanthem, sepsis, and septic shock. The pyrogenic
exotoxins are superantigens and therefore induce
production of large amounts of cytokines
Streptococcus
pyogenes is a
gram-positive
bacterium that
usually grows in
pairs or chains.
Unit 2: Bacteriology
81
3) Streptokinase. Dissolves fibrin; facilitates spread of
streptococci in tissues.
4) Hyaluronidase. Breaks down a substance that cements
tissues together.
5) DNases. Breakdown of DNA, producing runny pus.
NADase is leukotoxic.
6) Streptodornases A-D possess deoxyribonuclease
activity; Streptodornases B & D possess ribonuclease
activity as well
7) Protease activity similar to that inStaphylococcus
aureus has been shown in strains causing soft tissue
necrosis ortoxic shock syndrome. This large repertoire of
products is important in the pathogenesis of S.
pyogenes infections. Even so, antibodies to these products
are relatively insignificant in protection of the host.
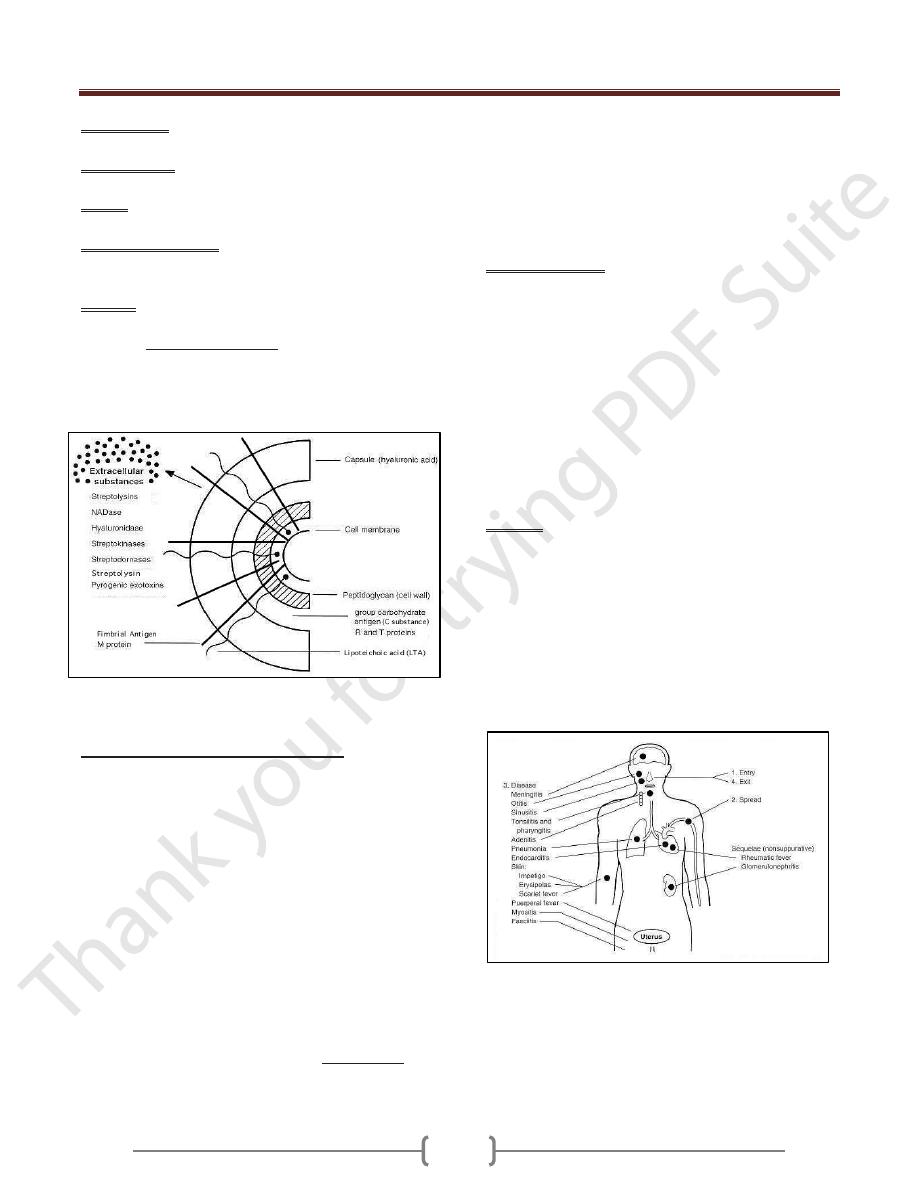
Cell surface structure of Streptococcus pyogenes and
secreted products involved in virulence.
Pathogenesis and clinical pictures.
Streptococcus pyogenes is one of the most frequent
pathogens of humans. It is estimated that between 5-15%
of normal individuals harbor the bacterium, usually in the
respiratory tract, without signs of disease. As normal
flora, S. pyogenes can infect when defenses are
compromised or when the organisms are able to penetrate
the constitutive defenses. When the bacteria are
introduced or transmitted to vulnerable tissues, a variety
of types of suppurative infections can occur.
Streptococcal diseases can be classified as either acute,
invasive infections or sequelae to them.
Acute
diseases associated with Streptococcus pyogenes occur
chiefly in the respiratory tract, bloodstream, or
the skin. Streptococcal disease is most often a respiratory
infection (pharyngitis or tonsillitis) or a skin infection
(pyoderma). Some strains of streptococci show a
predilection for the respiratory tract; others, for the skin.
Generally, streptococcal isolates from the pharynx and
respiratory tract do not cause skin infections. S.
pyogenes is the leading cause of uncomplicated
bacterial pharyngitis and tonsillitis commonly referred to
a strep throat. Other respiratory infections
include sinusitis, otitis,and pneumonia. Infections of the
skin can be superficial (impetigo) or deep (cellulitis).
Invasive infections. Invasive streptococci cause joint or
bone infections, destructive wound
infections (necrotizing fasciitis)
and myositis, meningitis and endocarditis . The pathogens
enter through traumas or microtraumas in the skin or
mucosa and cause invasive local or generalized infections.
The rare cases of severe septic infection and necrotizing
fasciitis occur in persons with a high-risk MHC II allotype.
In these patients, the PSE superantigens (especially
PSEA) induce large amounts of cytokine by binding at the
same time to the MHC II complex and the b chain of the
T cell receptor. The excess cytokines thus produced are the
cause of the symptoms.
Sequelae. Two post streptococcal sequelae, rheumatic
fever and glomerulonephritis, may follow streptococcal
disease, and occur in 1-3% of untreated infections. These
conditions and their pathology are not attributable to
dissemination of bacteria, but to aberrent immunological
reactions to Group A streptococcal antigens. Scarlet
fever and streptococcal toxic shock syndrome are
systemic responses to circulating bacterial toxins.
Glomerulonephritis is an immune complex disease and
acute rheumatic fever may be a type II immune disease.
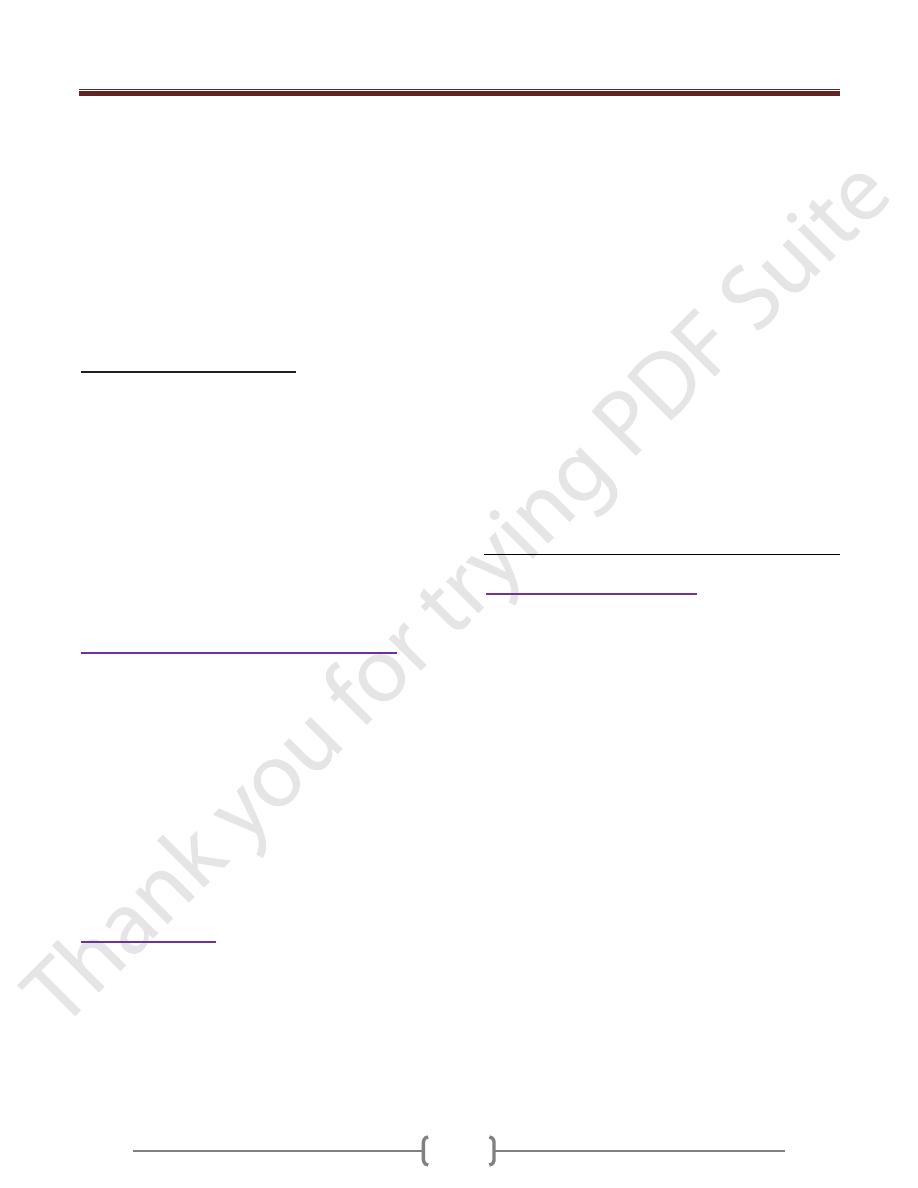
Fig: Pathogenesis of Streptococcus pyogenes infections
Unit 2: Bacteriology
82
Diagnosis
What is involved in diagnosis is detection of the pathogen
by means of microscopy and culturing. Group A antigen
can be detected using particles coated with antibodies that
precipitate agglutination (latex agglutination,
coagglutination). Using these methods, direct detection
of A streptococci in tonsillitis is feasible in the medical
practice. However, this direct detection method is not as
sensitive as the culture. Differentiation of A streptococci
from other β-hemolytic streptococci can be realized in the
laboratory with the bacitracin disk test, because A
streptococci are more sensitive to bacitracin than the other
types.
Therapy.
The agents of choice are penicillin G or V. Resistance is
unknown. Alternatives are oral cephalosporins or
macrolide antibiotics, although resistance to the latter can
be expected. In treatment of septic shock, a polyvalent
immunoglobulin is used to inactivate the PSE.
Epidemiology and prophylaxis.
Infection frequency varies according to geographical area,
season, and age. Humans are the only pathogen reservoir
for S. pyogenes. Transmission is by direct contact
(smear infection) or droplets. The incubation period is
one to three days. The incidence of carriers among
children is 10–20%, but can be much higher depending
on the epidemiological situation. Carriers and infected
persons are no longer contagious 24 hours after the start
of antibiotic therapy. Microbiological follow-up checks of
patients and first-degree contacts are not necessary
(exception: rheumatic history). In persons with recurring
infections or with acute rheumatic fever in their medical
histories, continuous penicillin prophylaxis with a long-
term penicillin is appropriate (e.g., 1.2 million IU
benzathine penicillin per month).
Streptococcus pneumoniae (Pneumococci)
Morphology and culturing
Pneumococci are Gram-positive, oval to lancet-shaped
cocci that usually occur in pairs or short chains. The cells
are surrounded by a thick capsule. When cultured on
blood agar, S. pneumoniae develop a-hemolytic colonies
with a mucoid (smooth, shiny) appearance (hence “S”
form). Mutants without capsules produce colonies with a
rough surface (“R” form). Antigen structure.
Pneumococci are classified in 90 different serovars based
on the fine chemical structure of the capsule
polysaccharides acting as antigens. This capsule antigen
can be identified using specific antisera in a reaction
known as capsular swelling.
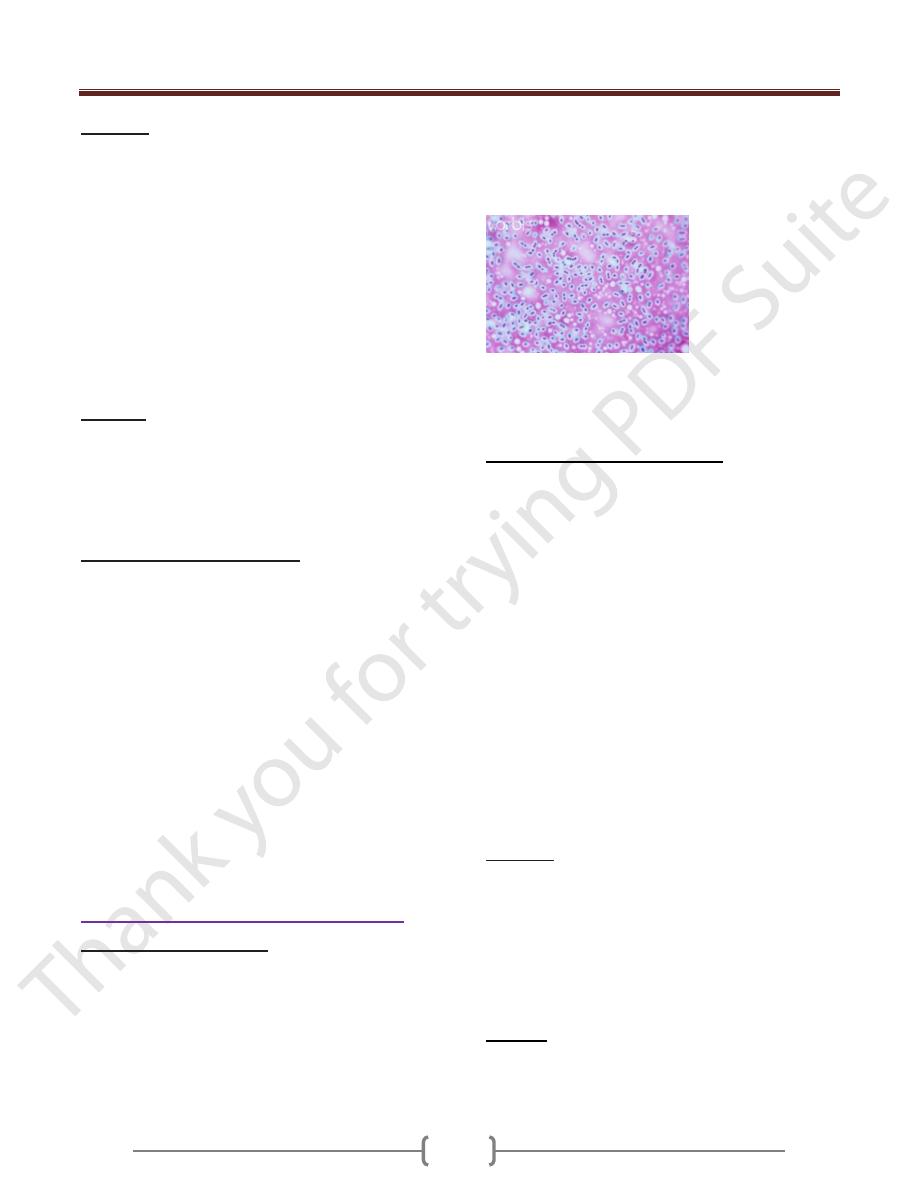
Streptococcus pneumoniae (also called Diplococcus
pneumoniae) bacteria may occur singly, in pairs or
diplococci form, and in chains . Capsule stain light
micrograph at a magnification of X1000.
Pathogenesis and clinical pictures
The capsule protects the pathogens from phagocytosis
and is the most important determinant of pneumococcal
virulence. Unencapsulated variants are not capable of
causing disease. Other potential virulence factors include
pneumolysin with its effects on membranes and an IgA1
protease. The natural habitat of pneumococci is provided
by the mucosa of the upper respiratory tract. About
40–70% of healthy adults are carriers. Pneumococcal
infections usually arise from this normal flora
(endogenous infections). Predisposing factors include
primary cardiopulmonary diseases, previous infections
(e.g., influenza), and extirpation of the spleen or
complement system defects. The most important
pneumococcal infections are lobar pneumonia and
bronchopneumonia. Other infections include acute
exacerbation of chronic bronchitis, otitis media,
sinusitis, meningitis, and corneal ulcer. Severe
pneumococcal infections frequently involve sepsis.
Diagnosis
The laboratory diagnosis includes detection of the
pathogen in appropriate test samples by means of
microscopy and culturing. Pneumococcus can be
differentiated from other a-hemolytic streptococci based
on their greater sensitivity to optochin (ethyl hydrocuprein
hydrochloride) in the disk test or their bile solubility. Bile
salts increase autolysis in pneumococci.
Therapy
Penicillin is still the antibiotic of choice. There have been
reports of high-frequency occurrence of strains resistant to
penicillin (South Africa, Spain, Hungary, USA). These
Unit 2: Bacteriology
83
strains are still relatively rare in Germany, Switzerland,
and Austria (5–10%). Macrolide antibiotics are an
alternative to penicillins, but resistance to them is also
possible. Penicillin resistance is not due to penicillinase,
but rather to modified penicillin-binding proteins
(PBPs) to which penicillins have a lower level of affinity.
PBPs are required for murein biosynthesis.
Biochemically, penicillin resistance extends to
cephalosporins as well. However, certain cephalosporins
(e.g., ceftriaxone) can be used against penicillin-resistant
pneumococci due to their higher levels of activity.
Epidemiology and prophylaxis
Pneumococcal infections are endemic and occur in all
seasons, more frequently in the elderly. Humans are the
natural pathogen reservoir. The vaccine (product
Pneumovax®) is available for immunization purposes, it
contains 25mg of the purified capsule polysaccharides of
each of 23 of the most frequent serovars. Eighty to ninety
percent of all isolated pneumococci have antigens
contained in this vaccine, which is primarily indicated in
persons with predisposing primary diseases. There is also
a seven-valent conjugate vaccine that is effective in
children under two years of age . Exposure prophylaxis is
not necessary.
Streptococcus agalactiae (B Streptococci)
B streptococci occasionally cause infections of the skin
and connective tissues, sepsis, urinary tract infections,
pneumonia, and peritonitis in immunocompromised
individuals. About one in 1000 neonates suffers from a
sepsis with or without meningitis. These infections
manifest in the first days of life (early onset type) or in
the first weeks of life (late onset type). In the early onset
form, the infection is caused intrapartum by B
streptococci colonizing the vagina. Potential
predisposing factors include birth complications,
premature birth, and a lack of antibodies to the capsule in
mother and neonate.
Oral Streptococci
Most of the oral streptococci of the type often known as
the viridans group have no group antigen. They usually
cause α-hemolysis, some c-hemolysis as well. Oral
streptococci are responsible for 50–70% of all cases of
bacterial endocarditis, overall incidence of which is one to
two cases per 100 000 annually. The origins of
endocarditis lie in invasion of the vascular system through
lesions in the oral mucosa. A transitory bacteremia
results. The heart valves are colonized and a biofilm is
formed by the organism. Predisposing factors include
congenital heart defects, acute rheumatic fever, cardiac
surgery, and scarred heart valves. Laboratory diagnosis of
endocarditis involves isolation of the pathogen from
blood cultures. Drug therapy of endocarditis is carried
out with either penicillin G alone or combined with an
aminoglycoside (mostly gentamicin). Bactericidal
activity is the decisive parameter. S. mutans, S. sanguis,
and S. mitis are, besides Actinomyces viscosus and A.
naeslundii, responsible for dental caries .These
streptococci can attach to the proteins covering the tooth
enamel, where they then convert sucrose into extracellular
polysaccharides (mutan, dextran, levan). These sticky
substances, in which the original bacterial layer along
with secondary bacterial colonizers are embedded, form
dental plaque. The final metabolites of the numerous
plaque bacteria are organic acids that breach the
enamel,allowing the different caries bacteria to begin
destroying the dentin.
Enterococcus (Enterococci)
Enterococci are a widespread bacterial genus normally
found in the intestines of humans and other animals. They
are nonmotile, catalase-negative, and characterized by
group antigen D. They are able to proliferate at 45 °C, in
the presence of 6.5% NaCl and at pH 9, qualities that
differentiate them from streptococci. As classic
opportunists, enterococci show only low levels of
pathogenicity. However, they are frequently isolated as
components of a mixed flora in nosocomial infections .
Ninety percent of such isolates are identified as E.
faecalis, 5–10% as E. faecium. Among the most
dangerous enterococcal infections is endocarditis, which
must be treated with a combination of an aminopenicillin
and streptomycin or gentamicin. Therapeutic success
depends on the bactericidal efficacy of the combination
used. The efficacy level will be insufficient in the
presence of high levels of resistance to either
streptomycin (MIC >1000 mg/l) or gentamicin (MIC
>500 mg/l) or resistance to the aminopenicillin.
Enterococci frequently develop resistance to antibiotics.
Strains manifesting multiple resistance are found mainly
in hospitals, in keeping with the classic opportunistic
character of these pathogens. Recently observed
epidemics on intensive care wards involved strains that
Unit 2: Bacteriology
84
were resistant to all standard anti-infective agents
including the glycopeptides vancomycin and teicoplanin.
Gram-Positive, Anaerobic Cocci
Gram-positive, strictly anaerobic cocci are included in the
genera Peptococcus and Peptostreptococcus. The only
species in the first genus is Peptococcus niger, whereas
the latter comprises a number of species. The anaerobic
cocci are commonly observed in normal human flora. In a
pathogenic context they are usually only encountered as
components of mixed florae together with other anaerobes
or facultative anaerobes. These bacteria invade tissues
through dermal or mucosal injuries and cause subacute
purulent infections. Such infections are either localized
in the head area (cerebral abscess, otitis media,
mastoiditis, sinusitis) or lower respiratory tract
(necrotizing pneumonia, pulmonary abscess,
empyema). They are also known to occur in the abdomen
(appendicitis, peritonitis, hepatic abscess) and female
genitals (salpingitis, endometriosis, tubo-ovarian
abscess). Gram-positive anaerobic cocci may also
contribute to soft-tissue infections and postoperative
wound infections.
Summary:
Streptococci are Gram-positive, nonmotile, catalase-
negative, facultatively anaerobic cocci that occur in
chains or pairs. They are classified based on their
hemolytic capacity (α-, β-, ƴ-hemolysis) and the
antigenicity of a carbohydrate occurring in their cell walls
(Lancefield antigen).b-hemolytic group A streptococci
(S. pyogenes) cause infections of the upper respiratory
tract and invasive infections of the skin and subcutaneous
connective tissue. Depending on the status of the immune
defenses and the genetic disposition, this may lead to
scarlet fever and severe infections such as necrotizing
fasciitis, sepsis, or septic shock. Sequelae such as acute
rheumatic fever and glomerulonephritis have an
autoimmune pathogenesis. The α-hemolytic pneumococci
(S. pneumoniae) cause infections of the respiratory tract.
Penicillins are the antibiotics of choice. Resistance to
penicillins is known among pneumococci, and is
increasing. Laboratory diagnosis involves pathogen
detection in the appropriate material. Persons at high risk
can be protected from pneumococcal infections with an
active prophylactic vaccine containing purified capsular
polysaccharides. Certain oral streptococci are responsible
for dental caries. Oral streptococci also cause half of all
cases of endocarditis. Although enterococci show only
low levels of pathogenicity, they frequently cause
nosocomial infections in immunocompromised patients
(usually as elements of a mixed flora).