Unit 4: Virology
211
Lecture Half 7+8 - RNA non
enveloped viruses
A- Picornaviruses
They are small nonenveloped viruses composed of an
icosahedral nucleocapsid and a SS RNA genome of
positive polarity.
They replicates in the cytoplasm of cells.
The picornavirus family includes 2 groups of medical
importance:
The Enteroviruses and rhinoviruses. Enteroviruses
include: Poliovirus, Coxackie viruses, Echoviruses, and
Hepatitis A virus.
I- Enteroviruses
1- Poliovirus
Disease: poliomyelitis which is an acute infectious
disease that in its serious form affects the central nervous
system.
Important properties
The host range is limited to primates, i.e., humans and
nonhuman such as apes and monkeys. This limitation is
due to the binding of the viral capsid protein to a receptor
found only on primate cell membrane.
There are three serologic (Antigenic) types based on
different antigenic determinants on the outer capsid
protein .There is little cross reaction.
Replicative cycle
1) The virion interact with specific cell receptor on the cell
membrane and then enter the cell
2) After uncoating, the genome RNA functions as mRNA
and is translated into one very large polypeptide called
non capsid viral protein. This polypeptide is cleaved by a
virus –encoded protease in multiple steps to form both the
capsid and non-capsid protein, including the RNA
polymerase that synthesizes the progeny RNA genomes.
3) Replication of the genome occurs by synthesis of a
complementary negative strand, which then serve as the
template for the positive strands. Some of these positive
strands function as mRNA to make more viral proteins,
and the remainder become progeny virion genome RNA.
4) Assembly of the progeny virions occurs by coating of the
genome RNA with caps proteins.
5) Virus released from the cell upon death of the cell.
Transmission, pathogenesis and immunity
Poliovirus is transmitted by feco-oral route. It replicates in
the oropharynx and intestine. The virus is regularly
present in the throat and in stools before onset of illness.
One week after infection there is little virus in the throat,
but virus continues to be excreted in the stools for several
weeks even though high antibody levels are present in the
blood. No permanent carrier state occurs following
infection by poliovirus.
It is believed that the virus first multiply in the tonsils,
lymph nodes of the neck, peyer´s patches, and the small
intestine.
The virus spread through the blood stream or retrograde
along nerve axons to CNS. In CNS, poliovirus
preferentially replicates in the motor neurons located in
the anterior horn of the spinal cord .Death of these cells
results in paralysis of the muscles innervated by those
neurons. The virus also affects the brain stem, leading to
bulbar poliomyelitis.
In infected individuals, the immune response consists of
both intestinal IgA and humoral IgG to specific serotype.
Infection provides lifelong type-specific immunity.
Clinical features
The infection ranges from inapparent infection, to mild
febrile illness, to severe and permanent paralysis.
a) Most infections are subclinical; only about 1% of
infections result in clinical illness. Incubation period is
usually 7-14 days, but it may range from 3 days to 35
days.
b) Mild disease. This is the most common form of the
disease. The patient has only a minor illness,
chartecterized by fever, malaise, drowsiness, headache,
Nausea, vomiting, constipation, and sore throat. Recovery
occurs in a few days.
c) Non paralytic poliomyelitis (Aseptic meningitis): in
addition to the symptoms of mild disease, the patient has
stiffness and pain in the back and neck. The disease lasts
2-10 days, and recovery is rapid and complete.
d) Paralytic poliomyelitis: the predominant complaint is
flaccid paralysis resulting from lower motor neuron
damage. Maximal recovery usually occurs within 6
months, with residual paralysis lasting much longer. The
meninges and brain may be involved in paralytic
poliomyelitis.
e) Progressive Post poliomyelitis Muscle Atrophy: A
recrudescence of paralysis and muscle wasting has been
observed in individuals decades after their experience
with paralytic poliomyelitis. It is not a consequence of
persistent infection but rather a result of physiologic and
Unit 4: Virology
211
aging changes in paralytic patients already burdened by
loss of neuromuscular function.
Laboratory diagnosis
1) Isolation of the virus from the throat, stool, or spinal
fluid by inoculation of cell culture. The virus cause
cytopathic effect (CPE) and can be identified by
neutralization of the CPE with specific antisera.
2) Rise in antibody titer in paired sera.
Treatment
1) There is no antiviral therapy.
2) Treatment is limited to symptomatic relief and
respiratory support, if needed.
3) Physiotherapy for the affected muscles is important.
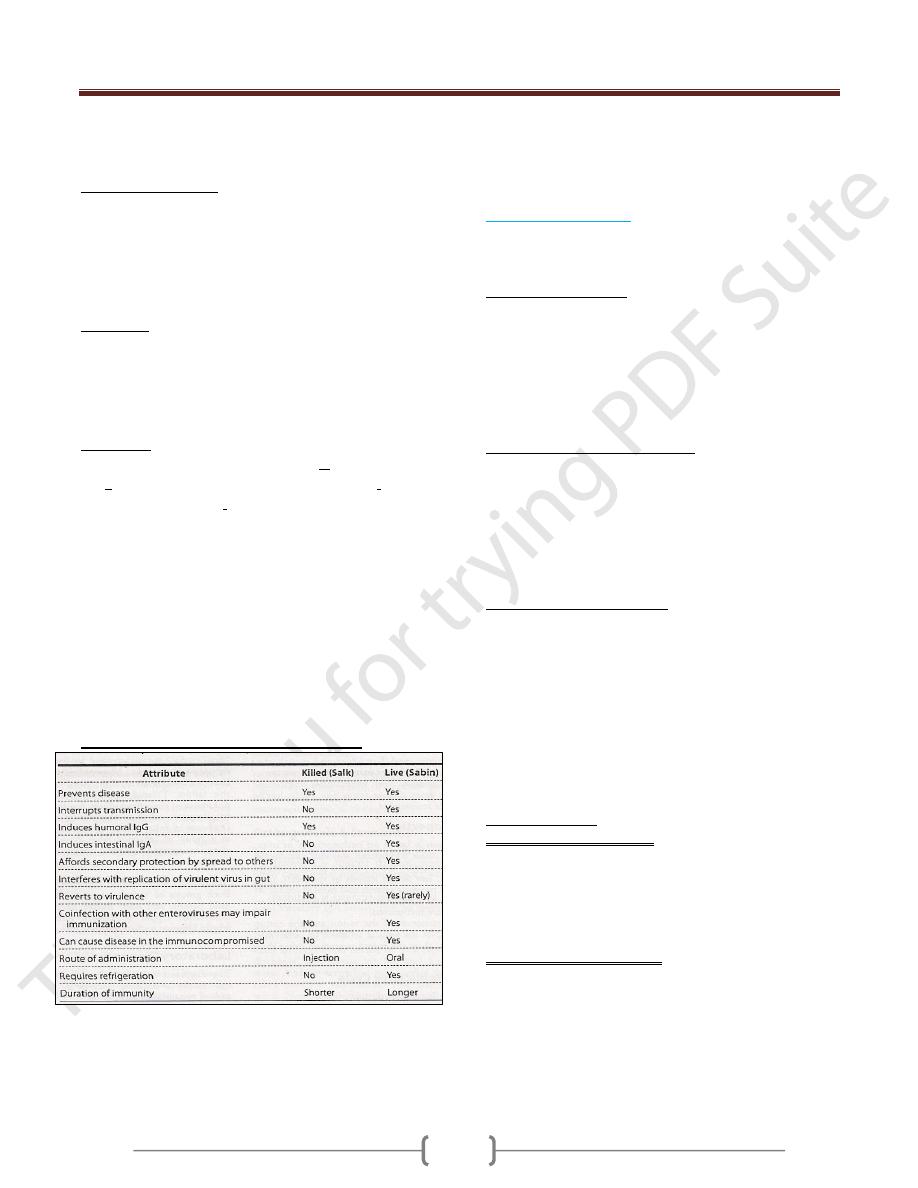
Prevention
Poliomyelitis can be prevented by both Killed vaccine
(Salk vaccine, inactivated vaccine, IPV) and the live,
attenuated vaccine (Sabin vaccine, oral vaccine, OPV).
Both vaccines induce humoral antibodies, which
neutralize virus entering the blood and hence prevent
central nervous system infection and disease. Both
vaccines contain all three serotypes.
The current version of the inactivated vaccine is called
enhanced polio vaccine, or eIPV .It has a high
seroconversion rate and induces a higher titer of antibody
than the previous IPV. eIPV also induces some mucosal
immunity IgA, making it capable of interrupting
transmission.
Important properties of poliovirus vaccines.
The currently approved vaccine schedule for OPV 2, 4, 6
month age, 18 months & upon entry to school at age 4-6
years.
Passive immunization with immune serum globulin is
available for protection of unimmunized individuals
known to have been exposed.
2- Coxackieviruses
Coxackieviruses are named for the town of Coxackie,
NY, where they were first isolated.
Important properties:
Group classification is based on pathogenicity in mice
Coxackieviruses group A includes 24 serotypes
Coxackieviruses group B includes 6serotypes.
The size and structure of virion and the nature of the
genome RNA are similar to poliovirus but unlike
poliovirus, they can infect mammals other than primates.
Transmission and epidemiology:
Coxackieviruses are transmitted primarily by the fecal-
oral route; but respiratory aerosols also play a role.
They replicate in the oropharynx and the intestinal tract.
Humans are the only natural hosts.
Coxackievirus infection occur worldwide, primarily in the
summer and fall.
Pathogenesis and immunity:
Group A virus has a predilection for skin and mucous
membranes, whereas group B viruses cause disease in
various organs such as the heart, pleura, pancreas, and
liver. Both groups can affect the meninges and the motor
neurons (anterior horn cells) to cause paralysis. From their
original site of replication in the oropharynx and GIT,
they disseminate via blood stream.
Immunity following infection is provided by type –
specific IgG antibodies.
Clinical findings:
1) Group A- specific diseases
Herepangina is characterized by fever, sore throat, and
tender vesicles in the oropharynx.
Foot-and-mouth disease is characterized by a vesicular
rash on the hands and feet and ulcerations in the mouth,
mainly in children.
2) Group-B- Specific diseases:
Pleurodynia (Bronholm disease, epidemic myalgia, devil's
grip) is characterized by fever and severe pleuritic chest
pain.
Myocarditis and pericarditis are characterized by fever,
chest pain, and signs of congestive heart failure.
Diabetes in mice can be caused by pancreatic damage as a
result of infection with coxackievirus B4. This virus is
Unit 4: Virology
211
suspected to have a similar role in juvenile diabetes in
humans.
3) Disease caused by both groups:
Aseptic meningitis, mild paresis, and acute flaccid
paralysis similar to poliomyelitis. Upper respiratory
infections and minor febrile illnesses with or without rash
can occur also.
Laboratory diagnosis:
Virus isolation or serology.
Treatment :
Neither antiviral nor vaccines are available.
3- Echovirus
E= enteric C= cytopathic H= human O= orphan
More than 30 serotypes have been isolated
They are transmitted by the feco-oral route
It causes aseptic meningitis, URTI, febrile illnesses with
or without rash, infantile diarrhea, and hemorrhagic
conjunctivitis.
Neither antiviral nor vaccines are available.
4- Other enteroviruses
Enterovirus 70 cause acute haemorrhagic conjunctivitis
Enterovirus 71 meningitis, encephalitis, and paralysis,
diarrhea, pulmonary hemorrhages, hand –foot-and- mouth
disease, and herpangina.
Enterovirus 72 is hepatitis A virus.
II-Rhinoviruses
They are the main cause of common cold.
Important properties:
1) More than 100 serotypes.
2) They replicate better at 33 C
º
, so they replicate in nose
and conjunctiva.
3) They are acid labile, they are killed by gastric acid
when swallowed.
Transmission and epidemiology:
2 modes of transmission.
1- Direct via respiratory aerosol
2- Indirect, in which respiratory droplets are deposited on
hands or on a surface such as table and then transported
by fingers to the nose or eyes.
A few serotypes of rhinoviruses are prevalent during one
season, only to be replaced by other serotypes during the
following seasons.
Clinical findings
Incubation period of 2-4 days, sneezing, nasal discharge,
and headache are common with chilly sensation. The
illness lasts about 1 week.
Laboratory diagnosis
Viral isolation rarely done.
Treatment
No antiviral drugs are available.
B- Calciviruses
They are small nonenveloped virus with single strand
RNA of positive polarity.
1- Norwalk virus (Norovirus)
It is one of the most common causes of gastroenteritis in
adult in USA and worldwide.
It is transmitted by fecooral route by ingestion of seafood
and contaminated water and diseaee is characterized by
sudden onset of vomiting and diarrhea with low grade
fever and abdominal cramping. The disease last for
several days.
No role for antiviral drugs. Supportive treatment id required.
C- Reovirus (Respiratory Enteric Orphan).
1- Rotavirus:
It is the most common cause of viral gastroenteritis in
young children.
Properties:
It has segmented (11 segments) double strand RNA
genome surrounded by double –layered icosahedral
capsid without an envelope.
The virion has RNA-dependent RNA polymerase.
There are at least six serotype of human rotavirus.
Rota virus attaches to cell surface at the site of ß-
adrenergic receptor.
Laboratory diagnosis:
Detection of rotavirus in the stool by ELISA.
Four fold increase in antibody titer
No role for viral culture in the diagnosis.
Prevention
There are two type of rotavaccine
1) Live attenuated vaccine (Rotarix) which contain single
most common serotype.
2) Live reassortant vaccine ( Rotateq) which contains
five rotavirus strain.