
574
CHAPTER 11
The Head and Neck
Muscles of the Head (continued )
T A B L E 1 1 . 4
Laterally:
parotid gland
tory meatus (Fig. 11.33) and the glenoid process of the
The tympanic plate of the external audi
Posteriorly:
Tuberosity of maxilla and
Temporalis
Muscle
Origin
Insertion
Nerve
Supply
Action
Muscles of Mastication
Masseter
Zygomatic arch
Lateral surface
ramus of mandible
Mandibular
division of
trigeminal
nerve
Elevates mandible to occlude teeth
Floor of temporal fossa
Coronoid process of
mandible
Mandibular
division of
trigeminal
nerve
Anterior and superior fibers
elevate mandible; posterior
fibers retract mandible
Lateral pterygoid (two
heads)
Greater wing of sphenoid
and lateral pterygoid
plate
Neck of mandible and
articular disc
Mandibular
division of
trigeminal
nerve
Pulls neck of mandible forward
Medial pterygoid (two
heads)
lateral pterygoid plate
Medial surface of angle
of mandible
Mandibular
division of
trigeminal
nerve
Elevates mandible
■
■
-
■
■
The parotid gland, fascia, and skin (see Fig. 11.85)
lotemporal nerve
The maxillary artery and vein and the auricu
Medially:
■
■
-
Clinical Significance of the Temporomandibular
of the temporomandibular joint may
articular disc
Joint
The temporomandibular joint lies immediately in front of the
external auditory meatus. The great strength of the lateral
temporomandibular ligament prevents the head of the mandi-
ble from passing backward and fracturing the tympanic plate
when a severe blow falls on the chin.
The
become partially detached from the capsule, and this results
in its movement becoming noisy and producing an audible
click during movements at the joint.
Dislocation of the Temporomandibular Joint
Dislocation sometimes occurs when the mandible is
depressed. In this movement, the head of the mandible and
the articular disc both move forward until they reach the sum-
mit of the articular tubercle. In this position, the joint is unsta-
ble, and a minor blow on the chin or a sudden contraction of
the lateral pterygoid muscles, as in yawning, may be sufficient
C L I N I C A L N O T E S
(continued)
to pull the disc forward beyond the summit. In bilateral cases,
lateral margins of the aponeurosis are attached to
occipitofrontalis muscle (Figs. 11.37 and 11.38). The
sheet that unites the occipital and frontal bellies of the
poneurosis (epicranial), which is a thin, tendinous
arteries, and a free anastomosis takes place between them.
arteries are branches of the external and internal carotid
Numerous arteries and veins are found in this layer. The
aponeurosis of the occipitofrontalis muscle (Fig. 11.37).
the fibrous septa uniting the skin to the underlying
onnective tissue beneath the skin, which is fibrofatty,
numerous sebaceous glands
kin, which is thick and hair bearing and contains
layer of the scalp.
to denote the
the scalp, use each letter of the word
To assist one in memorizing the names of the five layers of
intimately bound together and move as a unit (Fig. 11.37).
The scalp consists of five layers, the first three of which are
dislocation is easily achieved by pressing the gloved thumbs
the mouth is fixed in an open position, and both heads of the
mandible lie in front of the articular tubercles. Reduction of the
downward on the lower molar teeth and pushing the jaw back-
ward. The downward pressure overcomes the tension of the
temporalis and masseter muscles, and the backward pressure
overcomes the spasm of the lateral pterygoid muscles.
The Scalp
Structure
SCALP
■
■
S
■
■
C
■
■
A
Basic Anatomy
575
the temporal fascia. The subaponeurotic space is the
The origin, insertion, nerve supply, and action of this
Occipitofrontalis
the skull bones (Fig. 11.37).
continuous with the periosteum on the inner surface of
periosteum on the outer surface of the bones becomes
that at the sutures between individual skull bones, the
surface of the skull bones. It is important to remember
ericranium, which is the periosteum covering the outer
and with the intracranial venous sinuses (Fig. 11.37).
veins of the scalp with the diploic veins of the skull bones
emissary veins are valveless and connect the superficial
but it also contains some important emissary veins. The
nium). The areolar tissue contains a few small arteries,
aponeurosis to the periosteum of the skull (the pericra
space (Fig. 11.37) and loosely connects the epicranial
oose areolar tissue, which occupies the subaponeurotic
attachment of the aponeurosis to the temporal fascia.
itofrontalis muscle, and it extends laterally as far as the
limited in front and behind by the origins of the occip
potential space beneath the epicranial aponeurosis. It is
-
■
■
L
-
■
■
P
Muscles of the Scalp
muscle are described in Table 11.4.
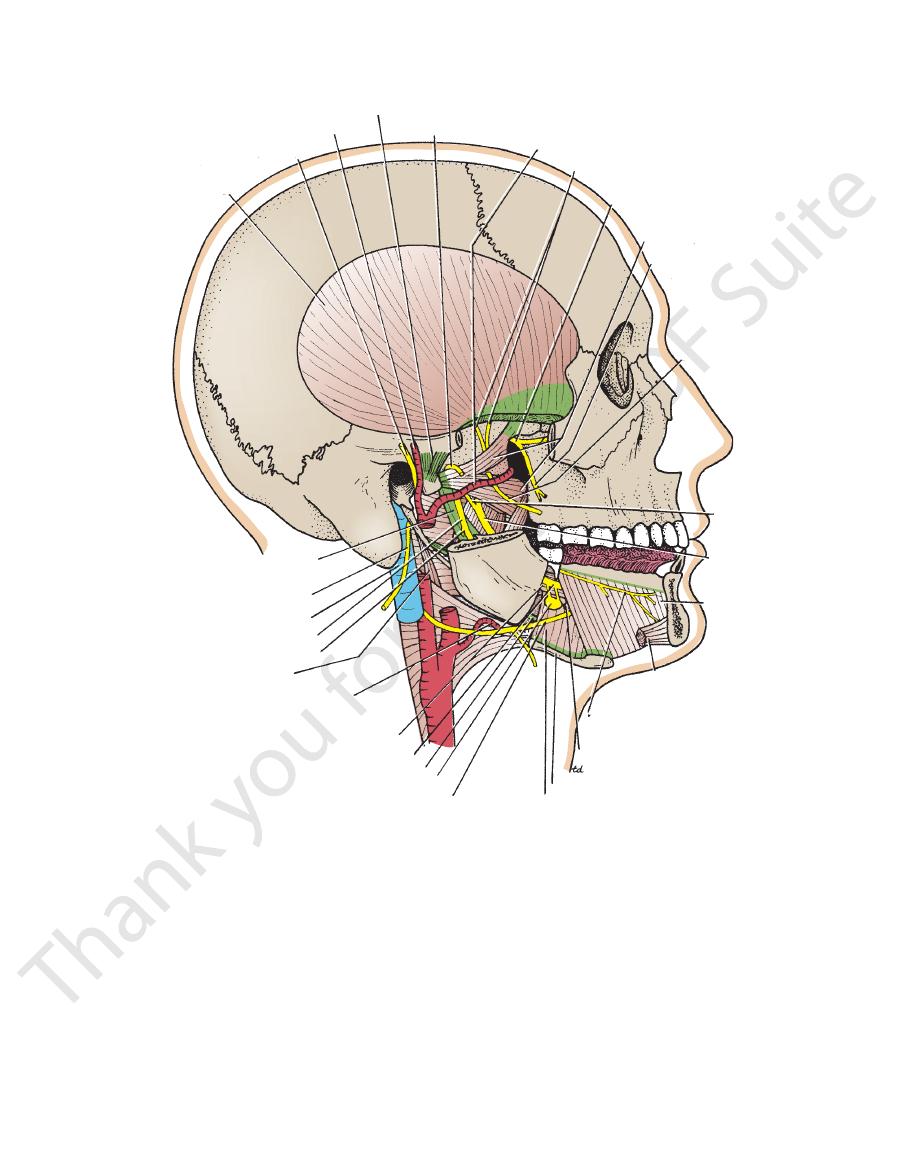
superficial temporal artery
auriculotemporal nerve
temporalis
temporomandibular joint
nerve to masseter
maxillary artery
deep temporal nerves
maxillary nerve
lateral pterygoid
posterior superior
alveolar nerve
buccal nerve
lingual
nerve
mylohyoid
anterior belly
of digastric
nerve to the mylohyoid and
anterior belly of digastric
submandibular duct
hyoid bone
hyoglossus
hypoglossal nerve
submandibular ganglion
lingual nerve
styloglossus
lingual artery
stylopharyngeus
nerve to mylohyoid
inferior alveolar nerve
internal jugular vein
spinal part of
accessory nerve
sphenomandibular ligament
stylohyoid ligament
chorda
tympani
nerve
FIGURE 11.36
Infratemporal and submandibular regions. Parts of the zygomatic arch, the ramus, and the body of the
mandible have been removed to display deeper structures.
576
CHAPTER 11
The Head and Neck
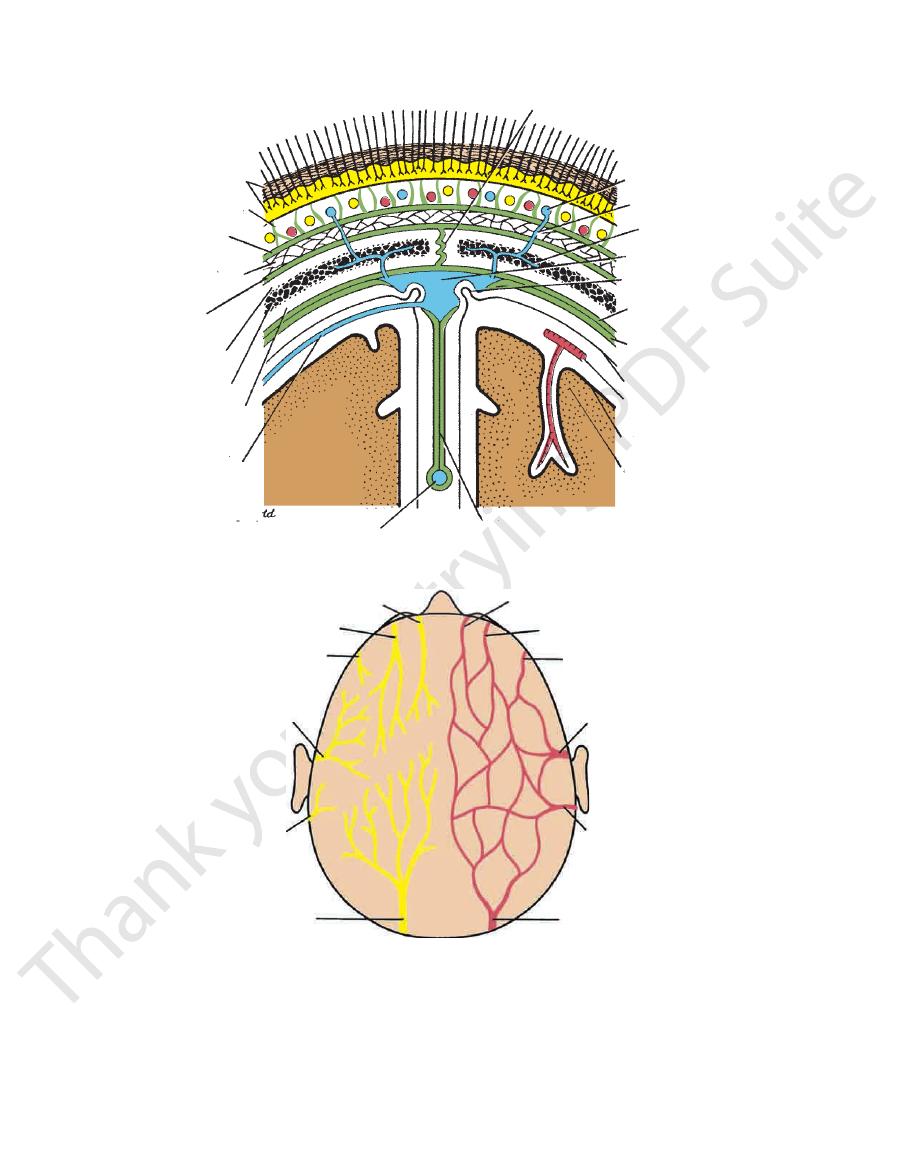
diploe¨
supratrochlear nerve
supraorbital nerve
zygomaticotemporal nerve
auriculotemporal nerve
lesser occipital nerve
greater occipital nerve
occipital artery
posterior auricular artery
superficial temporal artery
zygomaticotemporal artery
supraorbital artery
supratrochlear artery
A
B
skin
connective tissue
aponeurosis
loose connective
tissue
pericranium
(periosteum)
outer table of
parietal bone
inner table of
parietal bone
cerebral vein in
subarachnoid space
inferior sagittal sinus
falx cerebri
cerebral cortex
pia mater
cerebral artery in
subarachnoid space
arachnoid
meningeal layer
of dura mater
endosteal layer
of dura mater
arachnoid granulation
superior sagittal sinus
diploic vein
emissary vein
superficial vein of scalp
sagittal suture
FIGURE 11.37
A.
Sensory nerve supply and arterial supply to the scalp.
relation of cerebral blood vessels to the subarachnoid space.
the falx cerebri, the superior and inferior sagittal venous sinuses, the arachnoid granulations, the emissary veins, and the
Coronal section of the upper part of the head showing the layers of the scalp, the sagittal suture of the skull,
B.
Basic Anatomy
577
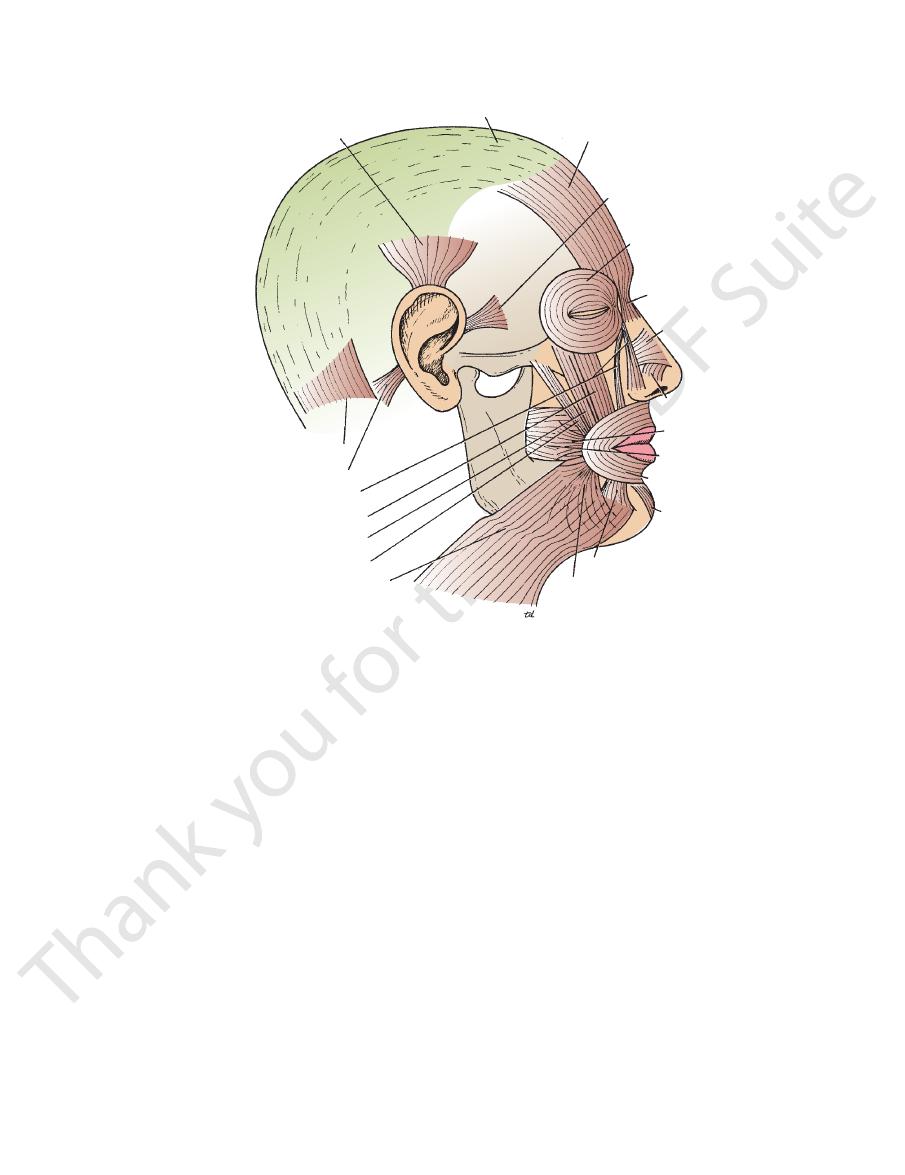
auricularis superior
epicranial aponeurosis
frontal belly of occipitofrontalis
auricularis anterior
orbicularis oculi
procerus
compressor naris
dilatator naris
buccinator
orbicularis oris
mentalis
depressor labii inferioris
depressor anguli oris
platysma
zygomaticus major
zygomaticus minor
levator labii superioris
levator labii superioris alaeque nasi
auricularis posterior
occipital belly of occipitofrontalis
risorius
FIGURE 11.38
Muscles of facial expression.
nerves (Fig. 11.37).
company with the supratrochlear and supraorbital
of the ophthalmic artery, ascend over the forehead in
branches
supraorbital arteries,
supratrochlear
The
the midline anteriorly, the following arteries are present:
The arteries lie in the superficial fascia. Moving laterally from
licles, and, for this reason, the smallest cut bleeds profusely.
The scalp has a rich supply of blood to nourish the hair fol
vertex of the skull (Fig. 11.37).
of the scalp and supplies the skin as far forward as the
ramus of the 2nd cervical nerve, ascends over the back
a branch of the posterior
greater occipital nerve,
The
face of the auricle.
ital region (Fig. 11.37) and the skin over the medial sur
(C2), supplies the scalp over the lateral part of the occip
a branch of the cervical plexus
lesser occipital nerve,
The
region.
terminal branches supply the skin over the temporal
of the head from in front of the auricle (Fig. 11.37). Its
division of the trigeminal nerve, ascends over the side
a branch of the mandibular
auriculotemporal nerve,
The
the temple (Fig. 11.37).
division of the trigeminal nerve, supplies the scalp over
a branch of the maxillary
zygomaticotemporal nerve,
The
11.37). It supplies the scalp as far backward as the vertex.
rior orbital margin and ascends over the forehead (Fig.
sion of the trigeminal nerve, winds around the supe
a branch of the ophthalmic divi
supraorbital nerve,
The
nearly as far as the vertex of the skull.
passes backward close to the median plane and reaches
rior orbital margin and supplies the scalp (Fig. 11.37). It
division of the trigeminal nerve, winds around the supe
a branch of the ophthalmic
supratrochlear nerve,
The
lowing nerves are present:
fascia. Moving laterally from the midline anteriorly, the fol
The main trunks of the sensory nerves lie in the superficial
surprise or horror.
occipitofrontalis can raise the eyebrows in expressions of
rosis to move on the pericranium. The frontal bellies of the
tissue of the fourth layer of the scalp allowing the aponeu
ers of the scalp move forward or backward, the loose areolar
Note that when this muscle contracts, the first three lay-
-
Sensory Nerve Supply of the Scalp
-
-
-
-
-
-
Arterial Supply of the Scalp
-
and the
578
CHAPTER 11
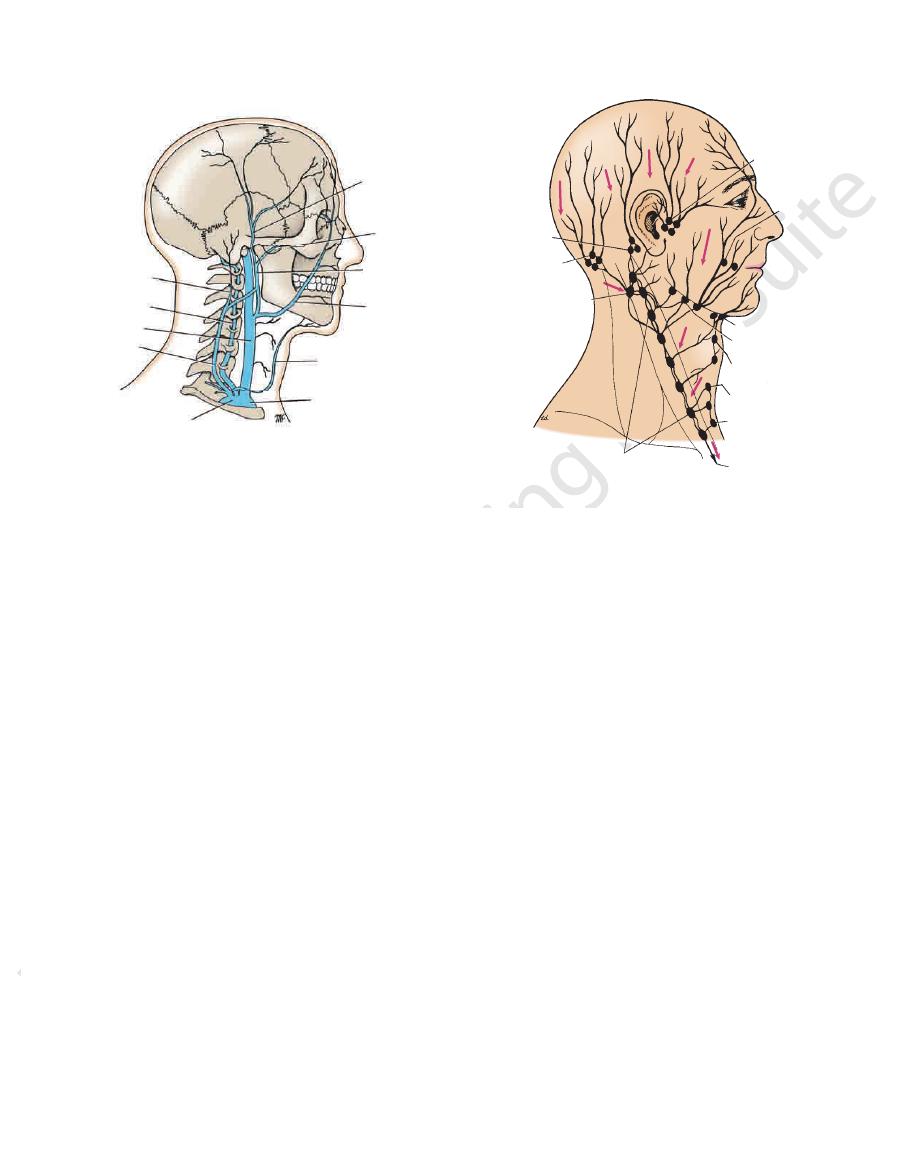
back of the scalp drain into the occipital nodes.
behind the ear drain into the mastoid nodes. Vessels in the
nodes; lymph vessels in the part of the scalp above and
above the ear is into the superficial parotid (preauricular)
(Fig. 11.40). Drainage from the lateral part of the scalp
forehead drain into the submandibular lymph nodes
Lymph vessels in the anterior part of the scalp and
Lymph Drainage of the Scalp
(Fig. 11.37).
emissary veins
bones and the intracranial venous sinuses by the valveless
another and are connected to the diploic veins of the skull
The veins of the scalp freely anastomose with one
bral veins or the internal jugular vein.
posterior triangle; the plexus in turn drains into the verte
plexus, which lies beneath the floor of the upper part of the
drains into the suboccipital venous
occipital vein
The
gland, to form the external jugular vein (Fig. 11.39).
division of the retromandibular vein, just below the parotid
unites with the posterior
posterior auricular vein
The
romandibular vein (Fig. 11.39).
vein in the substance of the parotid gland to form the ret
unites with the maxillary
superficial temporal vein
The
medial margin of the orbit to form the facial vein.
unite at the
supraorbital veins
supratrochlear
The
Venous Drainage of the Scalp
high as the vertex of the skull.
plies the skin over the back of the scalp and reaches as
pany with the greater occipital nerve (Fig. 11.37). It sup
ascends from the apex of the posterior triangle, in com
a branch of the external carotid artery,
occipital artery,
The
scalp above and behind the auricle (Fig. 11.37).
carotid artery, ascends behind the auricle to supply the
a branch of the external
posterior auricular artery,
The
temporal regions.
branches, which supply the skin over the frontal and
nerve (Fig. 11.37). It divides into anterior and posterior
of the auricle in company with the auriculotemporal
branch of the external carotid artery, ascends in front
the smaller terminal
superficial temporal artery,
The
The Head and Neck
-
-
and
-
-
Clinical Significance of the Scalp Structure
because of the attachment of the periosteum to the sutural
other hand, subperiosteal blood or pus is limited to one bone
the nuchal lines, and laterally by the temporal lines. On the
skull, being limited in front by the orbital margin, behind by
the epicranial aponeurosis. It tends to spread over the
Blood or pus may collect in the potential space beneath
Occasionally, an infection of the scalp spreads by the emis
and the neck. Thus, in an emergency situation, encircle the head
the superficial arteries supplying the scalp ascend from the face
Anatomically, it is useful to remember in an emergency that all
through the windshield. Because of the profuse blood supply,
Even a small laceration of the scalp can cause severe blood loss.
the ducts of which are prone to infection and damage by combs.
It is important to realize that the skin, the subcutaneous tissue,
and the epicranial aponeurosis are closely united to one another
and are separated from the periosteum by loose areolar tissue.
The skin of the scalp possesses numerous sebaceous glands,
For this reason, sebaceous cysts of the scalp are common.
Lacerations of the Scalp
The scalp has a profuse blood supply to nourish the hair follicles.
It is often difficult to stop the bleeding of a scalp wound because
the arterial walls are attached to fibrous septa in the subcutane-
ous tissue and are unable to contract or retract to allow blood
clotting to take place. Local pressure applied to the scalp is the
only satisfactory method of stopping the bleeding (see below).
In automobile accidents, it is common for large areas of the
scalp to be cut off the head as a person is projected forward
it is often possible to replace large areas of scalp that are only
hanging to the skull by a narrow pedicle. Suture them in place,
and necrosis will not occur.
The tension of the epicranial aponeurosis, produced by the
tone of the occipitofrontalis muscles, is important in all deep
wounds of the scalp. If the aponeurosis has been divided, the
wound will gape open. For satisfactory healing to take place, the
opening in the aponeurosis must be closed with sutures.
Often, a wound caused by a blunt object such as a base-
ball bat closely resembles an incised wound. This is because
the scalp is split against the unyielding skull, and the pull of the
occipitofrontalis muscles causes a gaping wound. This anatomic
fact may be of considerable forensic importance.
Life-Threatening Scalp Hemorrhage
just above the ears and eyebrows with a tie, shoelaces, or even
a piece of string and tie it tight. Then, insert a pen, pencil, or stick
into the loop and rotate it so that the tourniquet exerts pressure
on the arteries.
Scalp Infections
Infections of the scalp tend to remain localized and are usually
painful because of the abundant fibrous tissue in the subcutane-
ous layer.
-
sary veins, which are valveless, to the skull bones, causing
osteomyelitis. Infected blood in the diploic veins may travel by
the emissary veins farther into the venous sinuses and produce
venous sinus thrombosis.
ligaments.
C L I N I C A L N O T E S
Basic Anatomy
579
posterior
auricular vein
vertebral vein
internal jugular
vein
external
jugular
vein
right
brachiocephalic
vein
anterior jugular vein
facial vein
maxillary
vein
superficial
temporal
vein
subclavian
vein
retromandibular
vein
FIGURE 11.39
Main veins of the head and neck.
retroauricular
(mastoid nodes)
occipital
nodes
superficial
cervical
nodes
deep cervical nodes
jugular trunk
tracheal nodes
laryngeal nodes
anterior cervical
nodes
submandibular
nodes
submental nodes
buccal
nodes
parotid nodes
FIGURE 11.40
Lymph drainage of the head and neck.
area over the angle of the mandible and the parotid gland
divisions of the trigeminal nerve, except for the small
The skin of the face is supplied by branches of the three
they follow the wrinkle lines.
elasticity. Surgical scars of the face are less conspicuous if
contracting muscles, coupled with the loss of youthful skin
of the skin perpendicular to the long axis of the underlying
Wrinkle lines of the face result from the repeated folding
No deep fascia is present in the face.
of facial expression.
loose connective tissue, in which are embedded the muscles
ceous glands. It is connected to the underlying bones by
The skin of the face possesses numerous sweat and seba
The Face
Skin of the Face
-
Sensory Nerves of the Face
(Fig. 11.41), which is supplied by the great auricular nerve
process; the maxillary nerve serves the region developed
nerve supplies the region developed from the frontonasal
of dermatomes of the trunk and limbs. The ophthalmic
inal nerve is slight compared with the considerable overlap
(C2 and 3). The overlap of the three divisions of the trigem-
supratrochlear nerve
infratrochlear nerve
supraorbital
nerve
lacrimal nerve
zygomaticotemporal
nerve
auriculotemporal
nerve
infraorbital nerve
external nasal nerve
buccal nerve
great auricular nerve
mental nerve
cervical branch
mandibular
branch
buccal
branch
zygomatic
branch
temporal
branch
supratrochlear artery
supraorbital artery
zygomaticotemporal
artery
superficial temporal artery
lacrimal artery
zygomaticofacial artery
infraorbital artery
transverse facial artery
external nasal artery
facial artery
mental artery
external carotid artery
internal jugular vein
mental vein
facial vein
transverse facial
vein
infraorbital vein
zygomaticofacial
vein
supraorbital vein
supratrochlear vein
A
C
zygomaticofacial
nerve
lacrimal vein
superficial temporal
vein
zygomaticotemporal
vein
B
D
FIGURE 11.41
A.
Venous drainage of the face.
Arterial supply of the face.
expression.
Branches of the 7th cranial nerve to muscles of facial
Sensory nerve supply to the skin of the face. B.
C.
D.