626
CHAPTER 11
The Head and Neck
The anterior two thirds of the tongue is separated from the
soft palate.
foramen. The glossopharyngeal nerve also supplies the
enters the front of the hard palate through the incisive
nasopalatine nerve, also a branch of the maxillary nerve,
the greater and lesser palatine foramina (Fig. 11.74). The
division of the trigeminal nerve enter the palate through
The greater and lesser palatine nerves from the maxillary
Nerve Supply of the Palate
nerve supply, and actions are summarized in Table 11.9.
The muscles of the soft palate, their origins, insertions,
a tense sheet.
that the soft palate may be moved upward or downward as
cles of the two sides contract, the soft palate is tightened so
expands to form the palatine aponeurosis. When the mus
The tendon, together with the tendon of the opposite side,
don, which turns medially around the pterygoid hamulus.
as they descend from their origin to form a narrow ten
The muscle fibers of the tensor veli palatini converge
nerve as it passes downward and forward in the carotid tri
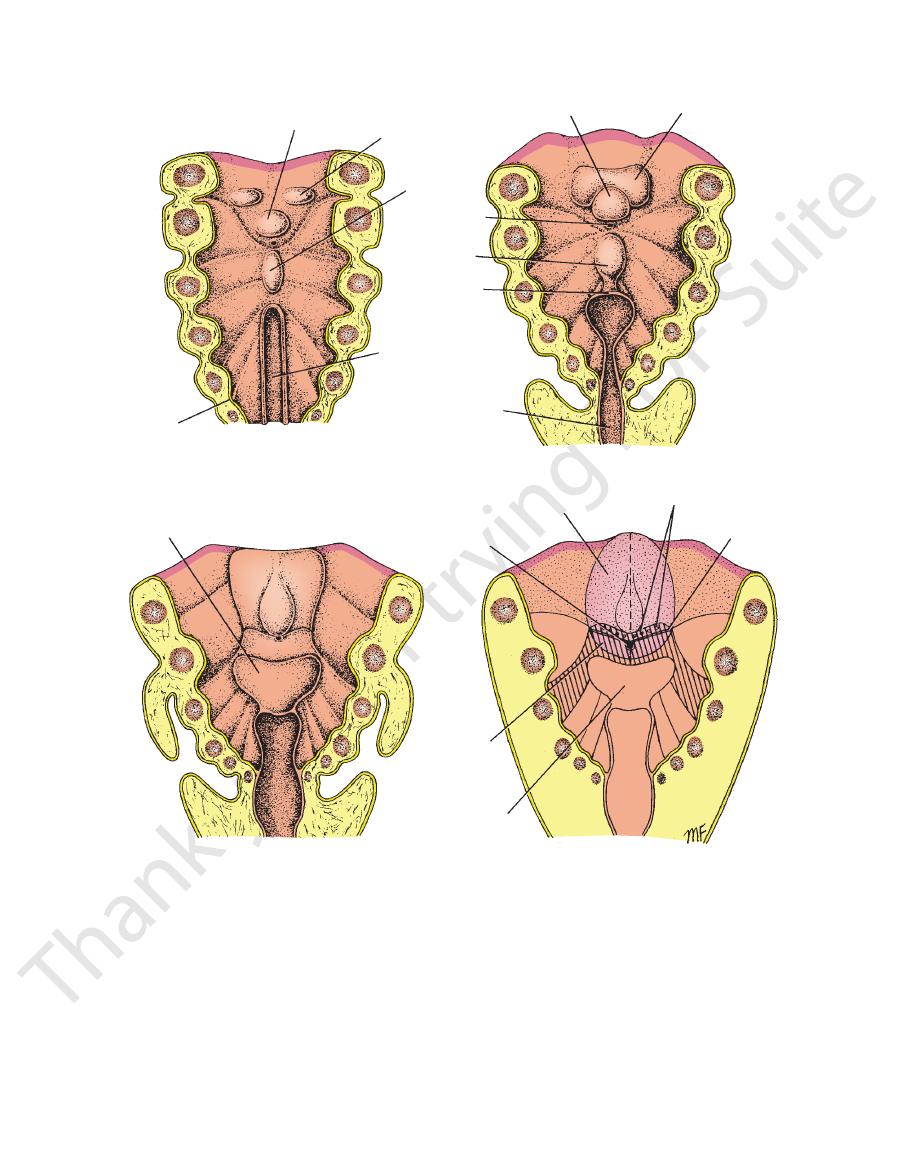
ing hindbrain and later migrate inferiorly and anteriorly around
the mucous membrane just anterior to the sulcus terminalis,
of the tongue becomes free. Some of the entodermal cells remain
lying mesenchyme. Later, these cells degenerate so that this part
arches. Around the edge of the anterior two thirds of the tongue,
ryngeal arches and the anterior ends of the third pharyngeal
posterior third by a groove, the sulcus terminalis, which repre-
sents the interval between the lingual swellings of the first pha-
the entodermal cells proliferate and grow inferiorly into the under-
in the midline and help form the frenulum of the tongue.
Remember that the circumvallate papillae are situated on
and that their taste buds are innervated by the ninth cranial
nerve. It is presumed that during development the mucous
membrane of the posterior third of the tongue becomes pulled
anteriorly slightly, so that fibers of the ninth cranial nerve cross
the succus terminalis to supply these taste buds (Fig. 11.79).
The muscles of the tongue are derived from the occipital
myotomes, which at first are closely related to the develop-
the pharynx and enter the tongue. The migrating myotomes
carry with them their innervation, the 12th cranial nerve, and
this explains the long curving course taken by the 12th cranial
-
angle of the neck (see page 616).
-
-
right hypoglossal nerve
cut right hypoglossal
nerve
intact
hypoglossal
nerve
right half
of tongue
atrophied
genioglossus muscle
A
B
C
D
E
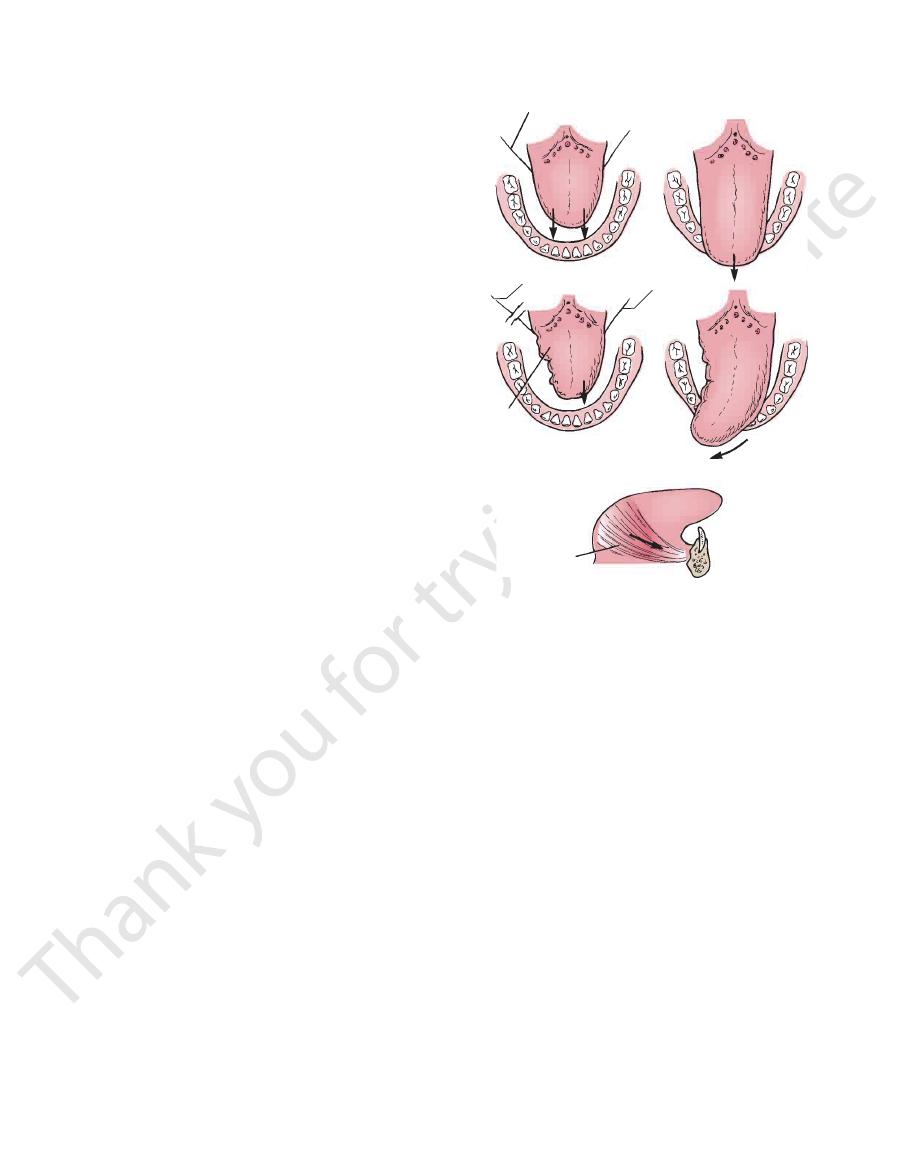
FIGURE 11.78
Diagrammatic representation of the action of
geus, and the musculus uvulae (Fig. 11.81).
levator veli palatini, the palatoglossus, the palatopharyn
The muscles of the soft palate are the tensor veli palatini, the
Muscles of the Soft Palate
don of the tensor veli palatini muscle.
posterior border of the hard palate. It is the expanded ten
The palatine aponeurosis is a fibrous sheet attached to the
Palatine Aponeurosis
faces of the soft palate.
The mucous membrane covers the upper and lower sur
Mucous Membrane
tine aponeurosis, and muscles.
The soft palate is composed of mucous membrane, pala
lateral wall of the pharynx.
The soft palate is continuous at the sides with the
uvula.
der presents in the midline a conical projection called the
border of the hard palate (Fig. 11.81). Its free posterior bor
The soft palate is a mobile fold attached to the posterior
(Fig. 11.80). It is continuous behind with the soft palate.
maxillae and the horizontal plates of the palatine bones
The hard palate is formed by the palatine processes of the
front and the soft palate behind.
nasal cavity. It is divided into two parts: the hard palate in
The palate forms the roof of the mouth and the floor of the
The origin and insertion and direction of
the nerve lesion.
asked to protrude the tongue, the tip points to the side of
When the patient is
The right hypoglossal nerve (which innervates
the tip of the tongue is protruded in the
The right and left muscles contract equally together
the right and left genioglossus muscles of the tongue.
A.
and as a result (B)
midline. C.
the genioglossus muscle and the intrinsic tongue muscles
on the same side) is cut and as a result the right side of the
tongue is atrophied and wrinkled. D.
E.
pull of the genioglossus muscle.
The Palate
Hard Palate
Soft Palate
-
-
-
-
-
Basic Anatomy
627
1
2
3
4
5
tuberculum impar
lingual swelling
of first pharyngeal
arch
copula
laryngotracheal
groove
endodermal
lining of pharynx
tuberculum impar
lingual swelling
of first pharyngeal
arch
copula
laryngotracheal
groove
developing
epiglottis
developing
epiglottis
epiglottis
foramen cecum
foramen cecum
posterior
third of
tongue
anterior two thirds
of tongue
circumvallate papillae
sulcus terminalis
A
B
C
D
6
1
2
3
4
5
6
FIGURE 11.79
The floor of the pharynx showing the stages in the development of the tongue.
the palatoglossal and palatopharyngeal arches (Fig. 11.81).
which are masses of lymphoid tissue, are located between
palatine tonsils,
The
palatopharyngeus muscle.
fold is the
join the pharyngeal wall. The muscle contained within the
(Figs. 11.72 and 11.81) that runs downward and laterally to
fold of mucous membrane behind the palatoglossal arch
The palatopharyngeal arch is a
Palatopharyngeal Arch
where the mouth becomes the pharynx.
The palatoglossal arch marks
(Figs. 11.72 and 11.81).
which extends from the soft palate to the side of the tongue
palatoglossus muscle,
mucous membrane containing the
The palatoglossal arch is a fold of
Palatoglossal Arch
Deep Cervical Lymph Nodes
Lymph Drainage of the Palate
ascending pharyngeal artery
ascending palatine branch of the facial artery, and the
The greater palatine branch of the maxillary artery, the
Blood Supply of the Palate
628
CHAPTER 11
The Head and Neck
maxillary artery
mandibular nerve
middle meningeal
artery
tensor veli palatini
levator veli palatini
auditory tube
superior constrictor
stylopharyngeus
stylohyoid ligament
superior laryngeal nerve
internal laryngeal nerve
external laryngeal nerve
inferior constrictor
recurrent laryngeal nerve
esophagus
trachea
cricothyroid muscle
thyrohyoid membrane
middle constrictor
mylohyoid
buccinator
incisive fossa
palatine
process
of maxilla
A
B
horizontal
plate of
palatine
bone
hard
palate
pterygomandibular ligament
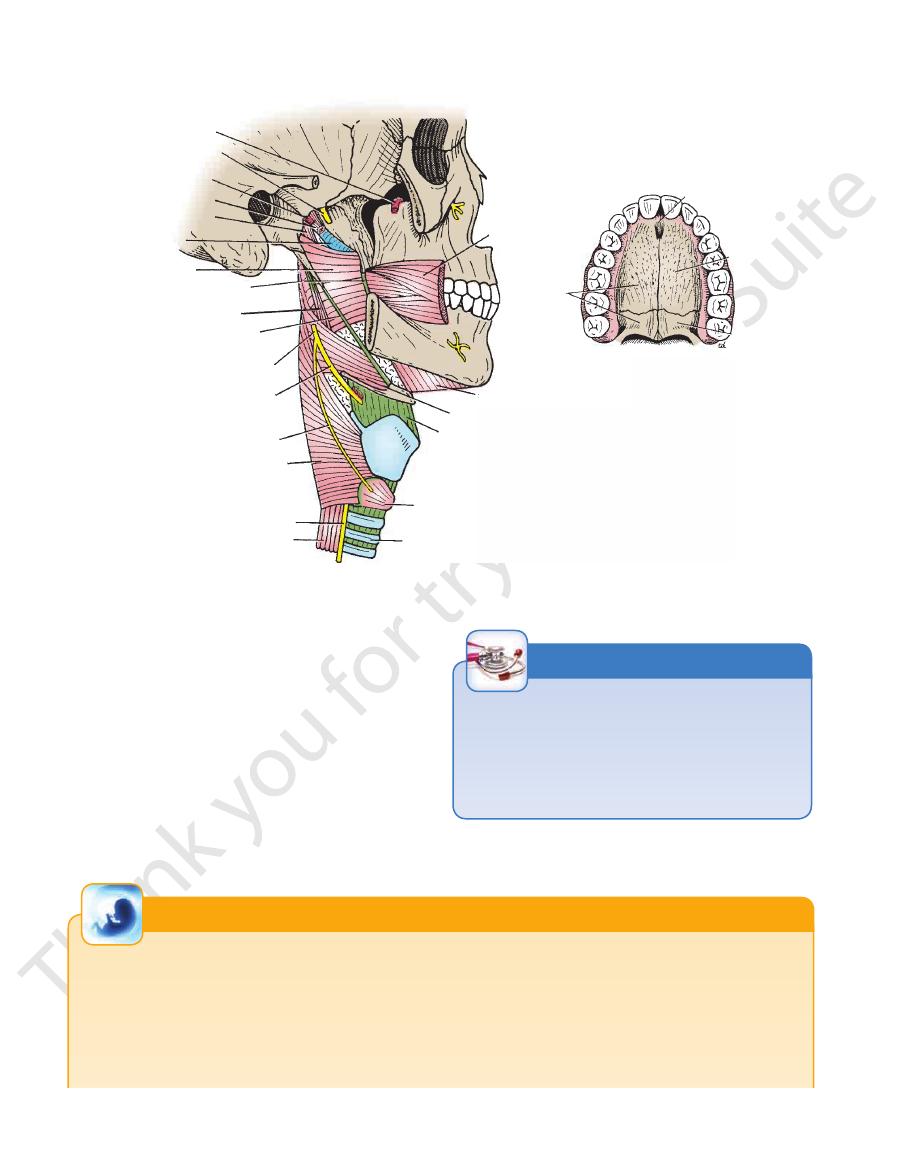
FIGURE 11.80
A.
off from the oral part.
tains. By this means, the nasal part of the pharynx is closed
palatopharyngeal arches are pulled medially, like side cur
geus muscles on both sides also contract so that the
the posterior pharyngeal wall forward. The palatopharyn
fibers of the superior constrictor muscle contract and pull
tor veli palatini on each side. At the same time, the upper
The soft palate is raised by the contraction of the leva
duction of explosive consonants in speech.
by raising the soft palate. Closure occurs during the pro
between the nasal and oral parts of the pharynx) is closed
The pharyngeal isthmus (the communicating channel
Movements of the Soft Palate
Three constrictor muscles of the pharynx. The superior and recurrent laryngeal nerves are also shown.
B. Hard palate.
-
-
-
-
Angioedema of the Uvula (Quincke’s Uvula)
lae, that is attached to the posterior border of the hard palate.
The uvula has a core of voluntary muscle, the musculus uvu-
Surrounding the muscle is the loose connective tissue of the
submucosa that is responsible for the great swelling of this
structure secondary to angioedema.
C L I N I C A L N O T E S
Development of the Palate
fusion takes place from the anterior to the posterior region. The
In early fetal life, the nasal and mouth cavities are in commu-
nication, but later they become separated by the development
of the palate (Fig. 11.82). The primary palate, which carries
the four incisor teeth, is formed by the medial nasal process.
Posterior to the primary palate, the maxillary process on each
side sends medially a horizontal plate called the palatal process;
these plates fuse to form the secondary palate and also unite
with the primary palate and the developing nasal septum. The
primary and secondary palates later will form the hard palate.
Two folds grow posteriorly from the posterior edge of the palatal
processes to create the soft palate, so that the uvula is the last
structure to be formed (Fig. 11.82). The union of the two folds of
E M B R Y O L O G I C N O T E S
(continued)
Basic Anatomy
629
middle concha
palate
tongue
palatoglossal fold
vallecula
entrance to larynx
palatopharyngeal
fold
tonsil
uvula
superior
constrictor
sphenoid sinus
pharyngeal recess
salpingopharyngeal fold
tubal elevation
tensor veli palatini
auditory tube
levator veli palatini
salpingopharyngeus
superior
constrictor
soft palate
palatopharyngeus
middle constrictor
mucous membrane
epiglottis
palatoglossus
vallecula
nasal septum
middle concha
levator veli palatini
tensor veli
palatini
hamulus
musculus uvulae
uvula
palatopharyngeus
carotid sheath
internal carotid artery
facial artery
tonsillar
artery
external palatine
vein
ramus of mandible
vestibule of mouth
buccinator
lip
pterygomandibular
ligament
palatoglossus
tonsillar crypts
capsule of tonsil
palatopharyngeus
pharyngeal raphe
superior constrictor
A
B
C
D
auditory
tube
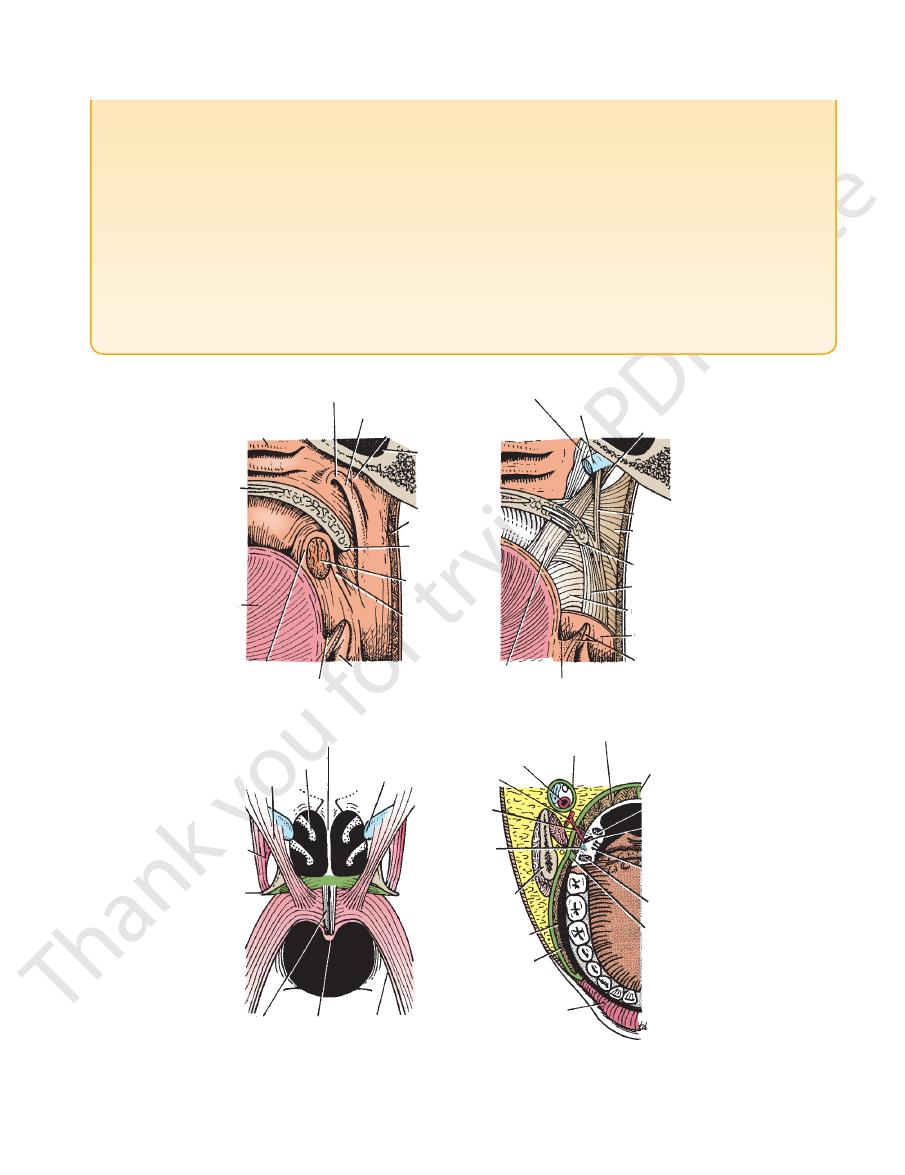
FIGURE 11.81
A.
pharynx showing the relations of the tonsil.
Horizontal section through the mouth and the oral part of the
Muscles of the soft palate seen from behind.
pharynx.
Muscles of the soft palate and the upper part of the
Note the position of the tonsil and the opening of the auditory tube.
Junction of the nose with the nasal part of the pharynx and the mouth with the oral part of the pharynx.
B.
C.
D.
the soft palate occurs during the eighth week. The two parts of
Plastic surgery is recommended usually between 1 and 2 years
regurgitated through the nose or aspirated into the lungs, leading
feeding problem, since he or she is unable to suck efficiently.
A baby born with a severe cleft palate presents a difficult
a bilateral cleft lip and failure of the primary palate to fuse with
associated with bilateral cleft lip. A rare form may occur in which
and a cleft on both sides of the primary palate. This type is usually
of severity, which is rare, consists of ununited palatal processes
is usually associated with unilateral cleft lip. The fourth degree
processes and a cleft on one side of the primary palate. This type
ununited palatal processes. The third degree is ununited palatal
first degree of severity is cleft uvula, and the second degree is
the primary palate (premaxilla) (Figs. 11.83 and 11.84). The
midline; in severe cases, these processes also fail to fuse with
palatal processes of the maxilla to fuse with each other in the
degrees of cleft palate occur and are caused by failure of the
Cleft palate is commonly associated with cleft upper lip. All
the uvula fuse in the midline during the 11th week. The interval
between the primary palate and secondary palate is represented
in the midline by the incisive foramen.
Cleft Palate
the palatal processes of the maxilla on each side are present.
Such a baby often receives in the mouth some milk, which then is
to respiratory infection. For this reason, careful artificial feeding
is required until the baby is strong enough to undergo surgery.
of age, before improper speech habits have been acquired.
630
CHAPTER 11
The Head and Neck
Muscles of the Soft Palate
T A B L E 1 1 . 9
Tenses soft palate
Tensor veli palatini
Muscle
Origin
Insertion
Nerve Supply
Action
Spine of sphenoid,
auditory tube
With muscle of other
side, forms palatine
aponeurosis
Nerve to medial pterygoid
from mandibular nerve
Levator veli palatini
Petrous part of temporal
bone, auditory tube
Palatine aponeurosis
Pharyngeal plexus
Raises soft palate
Palatoglossus
Palatine aponeurosis
Side of tongue
Pharyngeal plexus
Pulls root of tongue
upward and backward,
narrows oropharyngeal
isthmus
Palatopharyngeus
Palatine aponeurosis
Posterior border of
thyroid cartilage
Pharyngeal plexus
Elevates wall of pharynx,
pulls palatopharyngeal
folds medially
Musculus uvulae
Posterior border of hard
palate
Mucous membrane of
uvula
Pharyngeal plexus
Elevates uvula
communication
between nasal
and mouth
cavities
palatal process
of maxilla
superior concha
middle
concha
inferior
concha
tongue
nasal
cavity
palatal process
of maxilla
mouth
cavity
nasal
cavity
mouth
cavity
primary
palate
palatal
processes
of the
maxilla
nasal septum
primary
palate
primary palate
formation of
secondary palate
incisive
foramen
future
hard
palate
soft
palate
uvula
1
A
B
2
1
2
3
3
4
nasal septum
FIGURE 11.82
A.
molar tooth (Fig. 11.72).
the mouth upon a small papilla opposite the upper second
the lateral surface of the masseter. It enters the vestibule of
the anterior border of the gland and passes forward over
The parotid duct emerges from
deep lobes.
superficial
mastoid muscle. The facial nerve divides the gland into
mandible (Fig. 11.85), and in front of the sternocleido
the external auditory meatus, behind the ramus of the
posed mostly of serous acini. It lies in a deep hollow below
The parotid gland is the largest salivary gland and is com
The different stages in the formation
The formation of the palate and the nasal septum (coronal section). B.
of the palate.
The Salivary Glands
Parotid Gland
-
-
and