Basic Anatomy
35
it. This is especially so in an era in which automobile accidents,
blunt or penetrating wounds can injure the soft organs beneath
them considerable protection. Although the chest wall is strong,
nal organs, such as the liver, stomach, and spleen, and offers
life-sustaining organs—lungs, heart, and major blood vessels. In
Contained within the protective thoracic cage are the important
■
■
An understanding of the structure of the chest wall and the
diaphragm is essential if one is to understand the normal move-
ments of the chest wall in the process of aeration of the lungs.
■
■
addition, the lower part of the cage overlaps the upper abdomi-
stab wounds, and gunshot wounds are commonplace.
■
■
Because of the clinical importance of the chest wall, examiners
tend to focus on this area. Questions concerning the ribs and
their movements; the diaphragm, its attachments, and its func-
tion; and the contents of an intercostal space have been asked
many times.
natomy
asic
B
a
The thorax (or chest) is the region of the body between the
ninth thoracic vertebra (see Fig. 2.2).
lies opposite the body of the
xiphisternal joint
The
the 4th and 5th thoracic vertebrae.
sternal angle lies opposite the intervertebral disc between
from which all costal cartilages and ribs are counted. The
ridge lies at the level of the 2nd costal cartilage, the point
the anterior aspect of the sternum (Fig. 2.2). The transverse
can be recognized by the presence of a transverse ridge on
ulation of the manubrium with the body of the sternum,
(angle of Louis), formed by the artic
sternal angle
The
life. No ribs or costal cartilages are attached to it.
tilage that becomes ossified at its proximal end during adult
(see Fig. 2.1) is a thin plate of car
xiphoid process
The
Fig. 2.1).
it articulates with the 2nd to the 7th costal cartilages (see
On each side,
xiphisternal joint.
the xiphoid process at the
and below with
manubriosternal joint
manubrium at the
articulates above with the
body of the sternum
The
and 4th thoracic vertebrae.
tilages on each side (see Fig. 2.1). It lies opposite the 3rd
1st costal cartilage and the upper part of the 2nd costal car
joint, and it also articulates with the clavicles and with the
ulates with the body of the sternum at the manubriosternal
is the upper part of the sternum. It artic
manubrium
The
brium sterni, body of the sternum, and xiphoid process.
It is a flat bone that can be divided into three parts: manu
The sternum lies in the midline of the anterior chest wall.
cavity from the abdominal cavity.
inferiorly by the diaphragm, which separates the thoracic
tal spaces; superiorly by the suprapleural membrane; and
costal cartilages (Fig. 2.1); laterally by the ribs and intercos
part of the vertebral column; anteriorly by the sternum and
The thoracic wall is formed posteriorly by the thoracic
lined with parietal pleura.
by muscles attaching the shoulder girdle to the trunk. It is
The thoracic wall is covered on the outside by skin and
Structure of the Thoracic Wall
walls.
each side of the thorax, between the lungs and the thoracic
are formed, one on
pleural cavities
branous sacs called the
In this manner, two mem
parietal pleura.
it is called the
vessels enter) to the inner surface of the chest wall, where
lung at its root (i.e., where the main air passages and blood
which passes from each
visceral pleura,
brane called the
pleurae and lungs. The lungs are covered by a thin mem
and the laterally placed
mediastinum,
partition, called the
The cavity of the thorax can be divided into a median
upper extremity, abdomen, and back.
heart and affords attachment for the muscles of the thorax,
the diaphragm. The thoracic cage protects the lungs and
neck, and inferiorly it is separated from the abdomen by
in front. Superiorly, the thorax communicates with the
spaces on either side, and the sternum and costal cartilages
by the vertebral column behind, the ribs and intercostal
is formed
thoracic cage,
thorax, which is referred to as the
but rounded at the sides. The framework of the walls of the
neck and the abdomen. It is flattened in front and behind
-
-
-
Sternum
-
-
-
-
-
the surgeon to gain easy access to the heart, great vessels,
bone. The sternum may also be split at operation to allow
into the marrow cavity through the anterior surface of the
Under a local anesthetic, a wide-bore needle is introduced
Since the sternum possesses red hematopoietic marrow
Sternum and Marrow Biopsy
throughout life, it is a common site for marrow biopsy.
and thymus.
C L I N I C A L N O T E S
Ribs
the sternum by their costal cartilages.
The upper seven pairs are attached anteriorly to
True ribs:
2.5). The ribs are divided into three categories:
riorly to the thoracic vertebrae (Figs. 2.1 and 2.3, 2.4, and
There are 12 pairs of ribs, all of which are attached poste-
C H A P T E R O B J E C T I V E S
36
The Thorax: Part I—The Thoracic Wall
facet for
seventh costal
cartilage
xiphoid process
body of sternum
costal
cartilages
A
B
suprasternal notch
facet forclavicle
facet for
first costal
cartilage
facet for
second costal
cartilage
facet for
third costal
cartilage
facet for
fourth costal
cartilage
facet for
fifth costal
cartilage
facet for
sixth costal
cartilage
manubrium
body of first thoracic
vertebra
ribs
xiphoid process
rib 12
floating ribs
body
sternal angle
manubrium
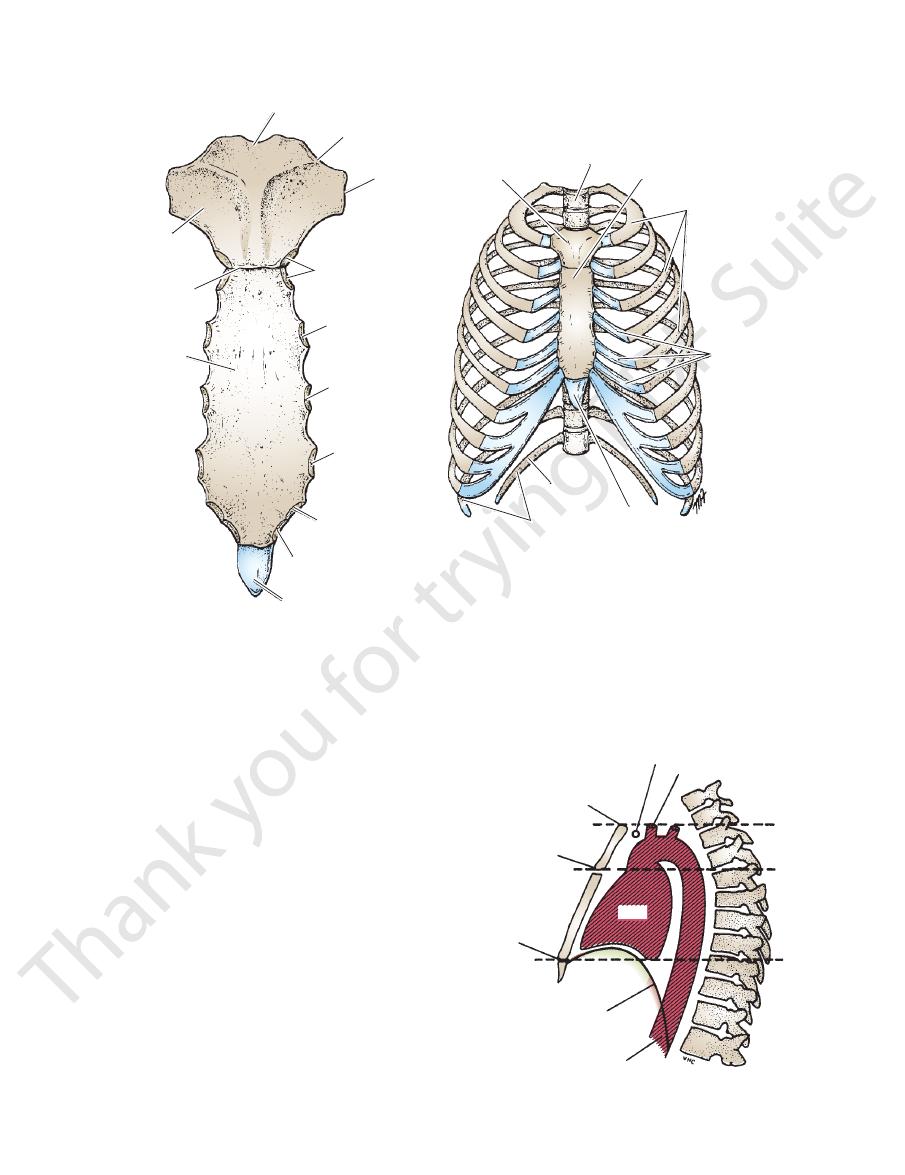
FIGURE 2.1
Sternum, ribs, and costal cartilages forming the thoracic skeleton.
Anterior view of the sternum.
A.
B.
left brachiocephalic vein
left common carotid artery
sternal angle
xiphisternal
joint
diaphragm
aorta
T1
2
4
5
9
12
heart
suprasternal notch
FIGURE 2.2
Lateral view of the thorax showing the relation
tionship to the lower nerves of the brachial plexus and the
The 1st rib is important clinically because of its close rela
sharply forward.
tal groove. The angle is where the shaft of the rib bends
twisted on its long axis. Its inferior border has the cos
tebra (see Fig. 2.4). The shaft is thin and flattened and
transverse process of the numerically corresponding ver
with the shaft. It has a facet for articulation with the
the outer surface of the rib at the junction of the neck
is a prominence on
tubercle
head and the tubercle. The
is a constricted portion situated between the
neck
The
and that of the vertebra immediately above (see Fig. 2.4).
tion with the numerically corresponding vertebral body
has two facets for articula
head
Figs. 2.4 and 2.5). The
(see
angle
head, neck, tubercle, shaft,
A rib has a
attached to the corresponding costal cartilage (Fig. 2.4).
costal vessels and nerve. The anterior end of each rib is
which accommodates the inter
costal groove,
forms the
(see Figs. 2.4 and 2.5). The inferior border overhangs and
smooth superior border and a sharp, thin inferior border
A typical rib is a long, twisted, flat bone having a rounded,
Typical Rib
attachment.
The 11th and 12th pairs have no anterior
Floating ribs:
their costal cartilages and small synovial joints.
anteriorly to each other and to the 7th rib by means of
The 8th, 9th, and 10th pairs of ribs are attached
False ribs:
ship of the surface markings to the vertebral levels.
-
-
and
-
-
-
Atypical Rib
-
Basic Anatomy
37
lamina
pedicle
facet for rib tubercle
transverse process
spinous process
inferior articular process
inferior vertebral notch
demifacet for rib head
body of vertebra
demifacet for rib head
superior articular process
heart-shaped body
demifacet for rib head
superior articular process
facet for rib
tubercle
transverse
process
spinous process
A
B
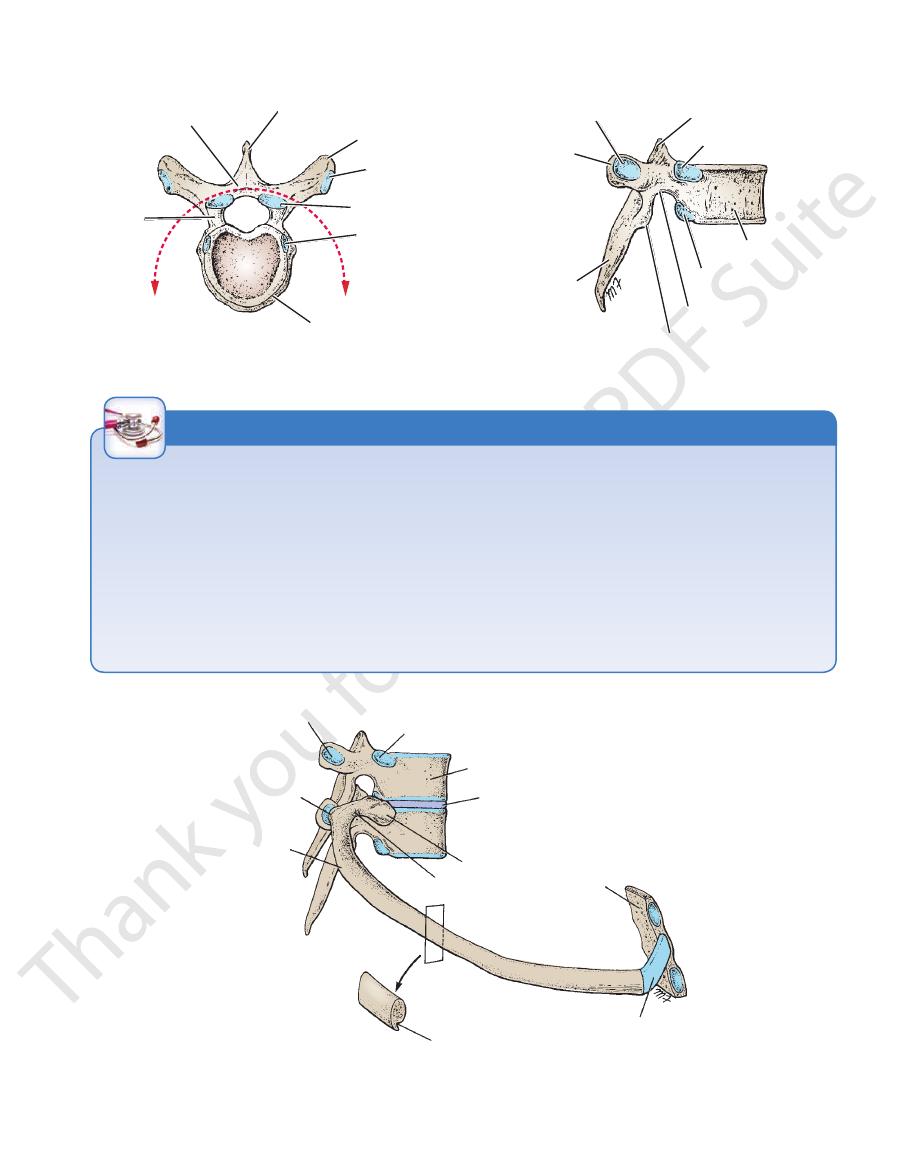
FIGURE 2.3
Thoracic vertebra.
Lateral surface.
Superior surface.
A.
B.
FIGURE 2.4
Fifth right rib as it articulates with the vertebral column posteriorly and the sternum anteriorly. Note that the rib
ence of the costal groove along the inferior border of the rib.
head articulates with the vertebral body of its own number and that of the vertebra immediately above. Note also the pres-
facet for tubercle of rib
tubercle of rib
angle of rib
cross section of rib
costal groove
costal cartilage
sternum
neck of rib
head of rib
intervertebral disc
body of vertebra
demifacet for head of rib
fifth rib
T4
T5
Cervical Rib
incision is then made through the bed of the rib, which is the
rib, and a segment of the rib is removed. A second longitudinal
sion is made through the periosteum on the outer surface of the
Rib excision is commonly performed by thoracic surgeons wish
It can also exert pressure on the overlying subclavian artery and
forearm and hand and wasting of the small muscles of the hand.
in some patients, producing pain down the medial side of the
can cause pressure on the lower trunk of the brachial plexus
late with the 1st rib. The importance of a cervical rib is that it
0.5% of humans (Fig. 2.7). It may have a free anterior end, may
transverse process of the 7th cervical vertebra) occurs in about
A cervical rib (i.e., a rib arising from the anterior tubercle of the
be connected to the 1st rib by a fibrous band, or may articu-
interfere with the circulation of the upper limb.
Rib Excision
-
ing to gain entrance to the thoracic cavity. A longitudinal inci-
inner covering of periosteum. After the operation, the rib regen-
erates from the osteogenetic layer of the periosteum.
C L I N I C A L N O T E S
38
9th, and 10th ribs to the cartilage immediately above. The
seven ribs to the lateral edge of the sternum and the 8th,
Costal cartilages are bars of cartilage connecting the upper
with the bone.
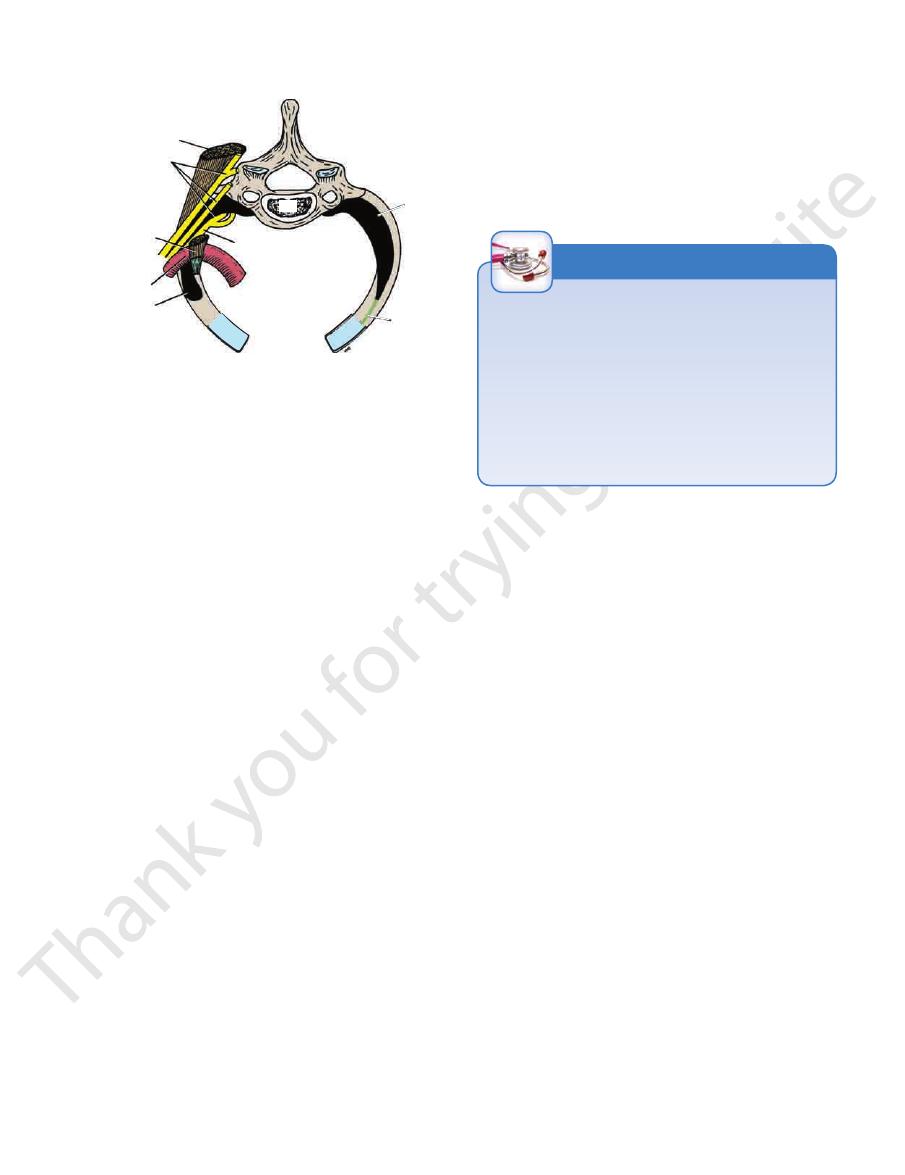
trunk of the brachial plexus cross the rib and lie in contact
the muscle attachment, the subclavian artery and the lower
anterior, the subclavian vein crosses the rib; posterior to
upper surface and inner border. Anterior to the scalenus
downward. The scalenus anterior muscle is attached to its
vein (Fig. 2.6). This rib is small and flattened from above
main vessels to the arm, namely, the subclavian artery and
The Thorax: Part I—The Thoracic Wall
Costal Cartilages
demifacet for
vertebral
body
demifacet for
vertebral body
articular part
of tubercle
sharp inferior
border
costal
groove
angle
rounded
superior
border
nonarticular part
of tubercle
neck
head
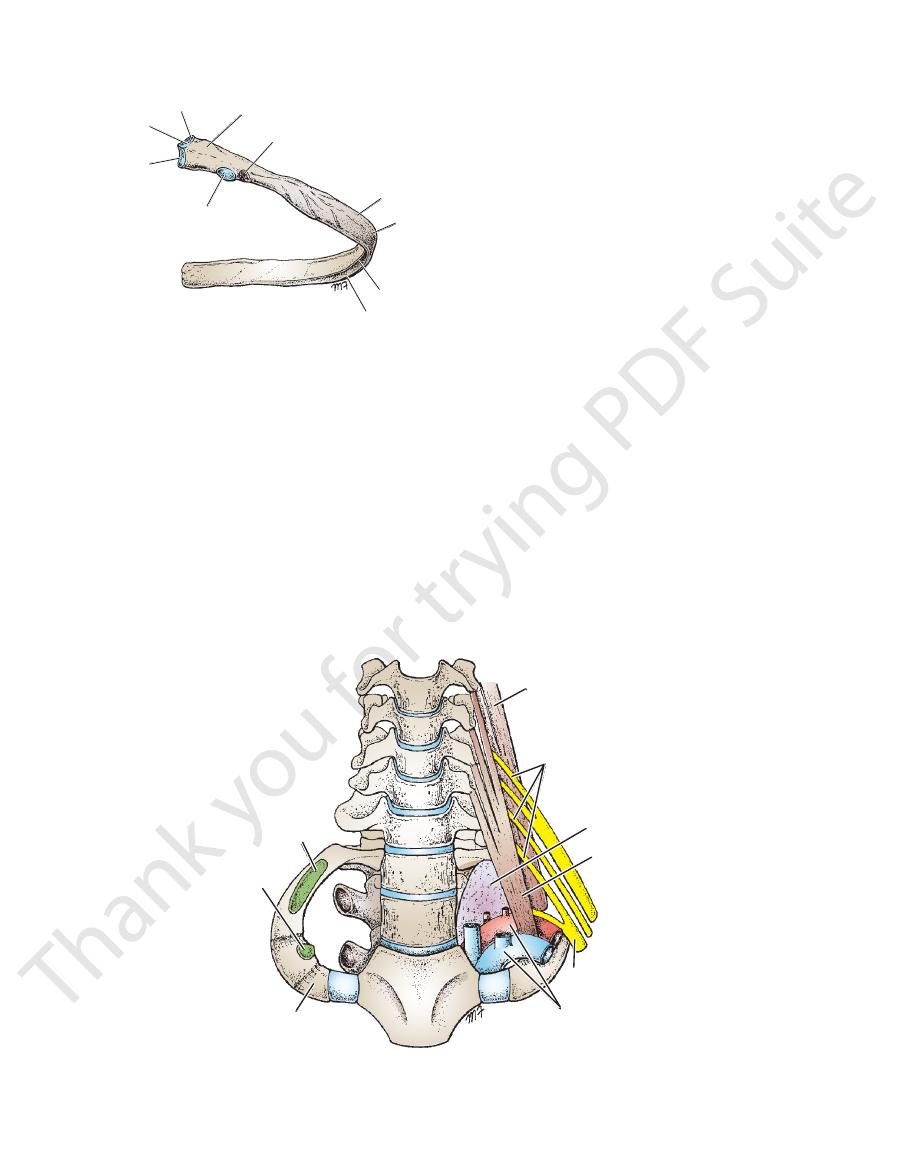
FIGURE 2.5
Fifth right rib, as seen from the posterior aspect.
insertion of scalenus medius
insertion of
scalenus anterior
first rib
scalenus medius
brachial plexus
cervical dome of pleura
scalenus anterior
lower trunk of plexus
subclavian artery and vein
C3
T1
C7
C6
C5
C4
T2
FIGURE 2.6
Thoracic outlet showing the cervical dome of pleura on the left side of the body and its relationship to the inner
12th ribs.)
tebra (see Fig. 2.4). (This joint is absent on the 11th and
joint with the transverse process of the corresponding ver
The tubercle of a rib articulates by means of a synovial
Joints of the Tubercles of the Ribs
tebral disc.
that connects the head to the interver
articular ligament
intra-
the vertebra above it (see Fig. 2.4). There is a strong
joint with the corresponding vertebral body and that of
2nd to 9th ribs, the head articulates by means of a synovial
vial joint with their corresponding vertebral body. For the
The 1st rib and the three lowest ribs have a single syno
Joints of the Heads of the Ribs
Joints of the Ribs
of the sternum during middle age.
sternum. The xiphoid process usually fuses with the body
between the xiphoid process (cartilage) and the body of the
is a cartilaginous joint
xiphisternal joint
respiration. The
A small amount of angular movement is possible during
between the manubrium and the body of the sternum.
is a cartilaginous joint
manubriosternal joint
The
Joints of the Sternum
Joints of the Chest Wall
result of superficial calcification.
costal cartilages tend to lose some of their flexibility as the
ticity and mobility of the thoracic walls. In old age, the
The costal cartilages contribute significantly to the elas
musculature (see Fig. 2.1).
cartilages of the 11th and 12th ribs end in the abdominal
border of the 1st rib. Note also the presence of brachial plexus and subclavian vessels. (Anatomists often refer to the tho-
racic outlet as the thoracic inlet.)
-
-
-
-
Basic Anatomy
The 1st costal cartilages articulate with the manubrium, by
Joints of the Costal Cartilages with the Sternum
possible.
These joints are cartilaginous joints. No movement is
Joints of the Ribs and Costal Cartilages
39
cartilaginous joints that permit no movement (see Fig. 2.1).
nerves, all of which pierce the diaphragm.
phragm, pass the esophagus and many large vessels and
Through this large opening, which is closed by the dia
ing costal margin, and anteriorly by the xiphisternal joint.
riorly by the 12th thoracic vertebra, laterally by the curv
through a large opening. The opening is bounded poste
The thoracic cavity communicates with the abdomen
into the neck.
ing, the apices of the lung and pleurae project upward
vessels and nerves. Because of the obliquity of the open
opening pass the esophagus and trachea and many
placed facing upward and forward. Through this small
border of the manubrium sterni. The opening is obliquely
and their costal cartilages, and anteriorly by the superior
vertebra, laterally by the medial borders of the 1st ribs
The opening is bounded posteriorly by the 1st thoracic
from the thorax here to enter the neck and upper limbs.
because important vessels and nerves emerge
outlet
It is called
thoracic outlet.
through an opening called the
The chest cavity communicates with the root of the neck
Openings of the Thorax
neck of each rib to rotate around its own axis.
both the joints of the head and the tubercle, permitting the
ribs during respiration are accompanied by movements in
ubrium and are immobile. The raising and lowering of the
The 1st ribs and their costal cartilages are fixed to the man
Movements of the Ribs and Costal Cartilages
the abdominal musculature.
The cartilages of the 11th and 12th ribs are embedded in
one another along their borders by small synovial joints.
6th, 7th, 8th, 9th, and 10th costal cartilages articulate with
border of the sternum by synovial joints. In addition, the
The 2nd to 7th costal cartilages articulate with the lateral
-
an
-
-
-
-
ing of the small muscles of the hand. Pressure on the blood
caused by pressure on the lower trunk of the plexus producing
be compressed between the bones. Most of the symptoms are
(see Fig. 2.6). It is here that the nerves or blood vessels may
face of the 1st rib and the clavicle as they enter the upper limb
The brachial plexus of nerves (C5, 6, 7, and 8 and T1) and the
The Thoracic Outlet Syndrome
subclavian artery and vein are closely related to the upper sur-
pain down the medial side of the forearm and hand and wast-
vessels may compromise the circulation of the upper limb.
C L I N I C A L N O T E S
Intercostal Spaces
nerves and vessels. The innermost intercostal muscle can be
cia) and parietal pleura and externally to the intercostal
the ribs. It is related internally to fascia (endothoracic fas
layer and crosses more than one intercostal space within
in the anterior abdominal wall. It is an incomplete muscle
layer and corresponds to the transversus abdominis muscle
forms the deepest
innermost intercostal muscle
The
Fig. 2.9).
(see
posterior (internal) intercostal membrane
rosis, the
ribs behind, where the muscle is replaced by an aponeu
backward from the sternum in front to the angles of the
border of the rib below (see Fig. 2.8). The muscle extends
from the subcostal groove of the rib above to the upper
ate layer. Its fibers are directed downward and backward
forms the intermedi
internal intercostal muscle
The
(Fig. 2.9).
brane
anterior (external) intercostal mem
aponeurosis, the
forward to the costal cartilage where it is replaced by an
border of the rib below (see Fig. 2.8). The muscle extends
from the inferior border of the rib above to the superior
ficial layer. Its fibers are directed downward and forward
forms the most super
external intercostal muscle
The
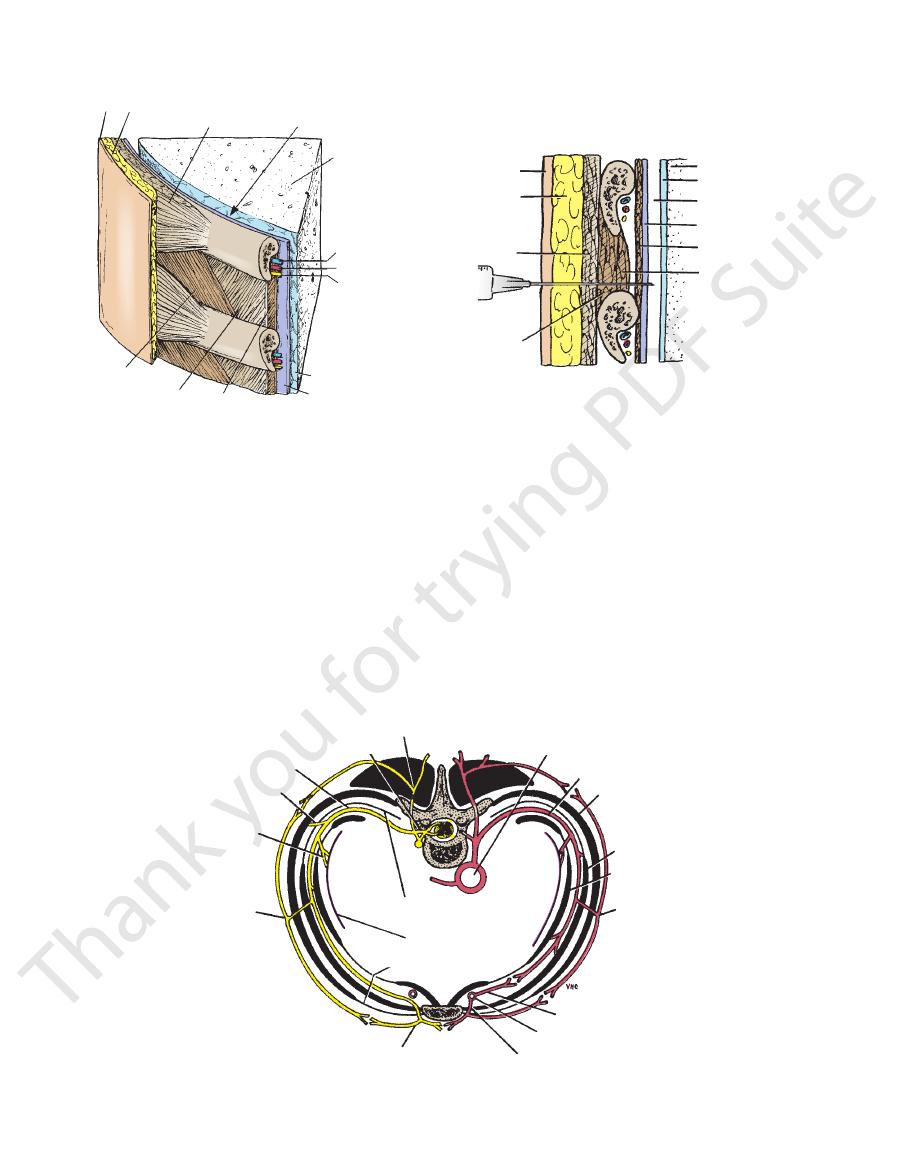
intercostal artery, and intercostal nerve (i.e., VAN).
the following order from above downward: intercostal vein,
deepest layers of muscles (Fig. 2.8). They are arranged in
nerves and blood vessels run between the intermediate and
is lined internally by the parietal pleura. The intercostal
which
endothoracic fascia,
muscle is lined internally by the
the innermost intercostal muscle. The innermost intercostal
ration: the external intercostal, the internal intercostal, and
The spaces between the ribs contain three muscles of respi-
Intercostal Muscles
-
-
-
-
-
scalenus
medius
C7
brachial
plexus
scalenus
anterior
subclavian
artery
cervical rib
lower trunk of plexus
fibrous
band
cervical
rib
FIGURE 2.7
Thoracic outlet as seen from above. Note the
the brachial plexus and may kink the subclavian artery.
that the cervical rib may exert pressure on the lower trunk of
fibrous band that is attached to the first costal cartilage. Note
thorax, the rib is rudimentary but is continued forward as a
articulates anteriorly with the 1st rib. On the left side of the
right side of the thorax, the rib is almost complete and
) on both sides. On the
black
presence of the cervical ribs (
40
intercostal nerves.
The intercostal muscles are supplied by the corresponding
Nerve Supply
page 74.
on
Mechanics of Respiration
action of these muscles, see
intrathoracic pressure. For further details concerning the
ing in or the blowing out of the tissues with changes in
sues of the intercostal spaces, thus preventing the suck
different phases of respiration serves to strengthen the tis
addition, the tone of the intercostal muscles during the
contraction of the intercostal muscles, as in expiration. In
abdomen, the 1st to the 11th ribs will be lowered by the
ratus lumborum muscle and the oblique muscles of the
ration. If, conversely, the 12th rib is fixed by the quad
the 2nd to the 12th ribs toward the 1st rib, as in inspi
namely, the scaleni muscles, the intercostal muscles raise
by the contraction of the muscles in the root of the neck,
pull the ribs nearer to one another. If the 1st rib is fixed
When the intercostal muscles contract, they all tend to
Action
less separate from one another.
divided into three portions (see Fig. 2.9), which are more or
The Thorax: Part I—The Thoracic Wall
-
-
-
-
skin superficial
fascia
serratus
anterior
pleural
cavity (space)
lung
intercostal vein
intercostal artery
intercostal nerve
visceral pleura
parietal pleura
innermost
intercostal
internal
intercostal
external
intercostal
A
skin
superficial
fascia
serratus
anterior
syringe
external
intercostal
lung
visceral pleura
pleural cavity (space)
parietal pleura and
endothoracic fascia
innermost intercostal
internal intercostal
B
FIGURE 2.8
to pleural cavity. Depending on the site of penetration, the pectoral muscles will be pierced in addition to the serratus ante
Structures penetrated by a needle when it passes from skin surface
Section through an intercostal space.
A.
B.
-
rior muscle.
lateral
cutaneous branch
posterior ramus
spinal nerve
intercostal nerve
muscular branch
branches to
parietal pleura
anterior cutaneous branch
perforating branch
internal thoracic artery
anterior intercostal artery
lateral cutaneous
branch
innermost intercostal
internal intercostal
external intercostal
posterior intercostal
artery
thoracic aorta
posterior intercostal membrane
parietal pleura
anterior intercostal
membrane
FIGURE 2.9
ve and a posterior and an anterior
Cross section of the thorax showing distribution of a typical intercostal ner
intercostal artery.
Basic Anatomy
neous branch.
first intercostal nerve is small, and there is no anterior cuta
branch of typical intercostal nerves. The remainder of the
by a large branch that is equivalent to the lateral cutaneous
is joined to the brachial plexus
first intercostal nerve
The
nerves only) run to the parietal peritoneum.
(7th to 11th intercostal
Peritoneal sensory branches
go to the parietal pleura.
Pleural sensory branches
run to the intercostal muscles.
Muscular branches
midline. It divides into a medial and a lateral branch.
portion of the main trunk, reaches the skin near the
which is the terminal
anterior cutaneous branch,
The
rior branch.
side of the chest. It divides into an anterior and a poste
reaches the skin on the
lateral cutaneous branch
The
main nerve on the upper border of the rib below.
runs forward inferiorly to the
collateral branch
The
the white ramus leaves it.
gray ramus joins the nerve medial at the point at which
a ganglion of the sympathetic trunk (see Fig. 1.26). The
connect the intercostal nerve to
Rami communicantes
See Figures 2.9 and 2.12.
Branches
abdominal wall.
the corresponding ribs are floating, pass directly into the
anterior abdominal wall. The 10th and 11th nerves, since
spaces by passing deep to the costal cartilages, to enter the
intercostal nerves leave the anterior ends of their intercostal
distributed within their intercostal spaces. The 7th to 9th
tal and internal intercostal muscle. The first six nerves are
of the corresponding rib, between the innermost intercos
inferiorly to the intercostal vessels in the subcostal groove
membrane (see Figs. 2.8 and 2.9). It then runs forward
between the parietal pleura and the posterior intercostal
Each intercostal nerve enters an intercostal space
subcostal nerve.
ward in the abdominal wall as the
the 12th thoracic nerve lies in the abdomen and runs for
11 thoracic spinal nerves (Fig. 2.12). The anterior ramus of
The intercostal nerves are the anterior rami of the first
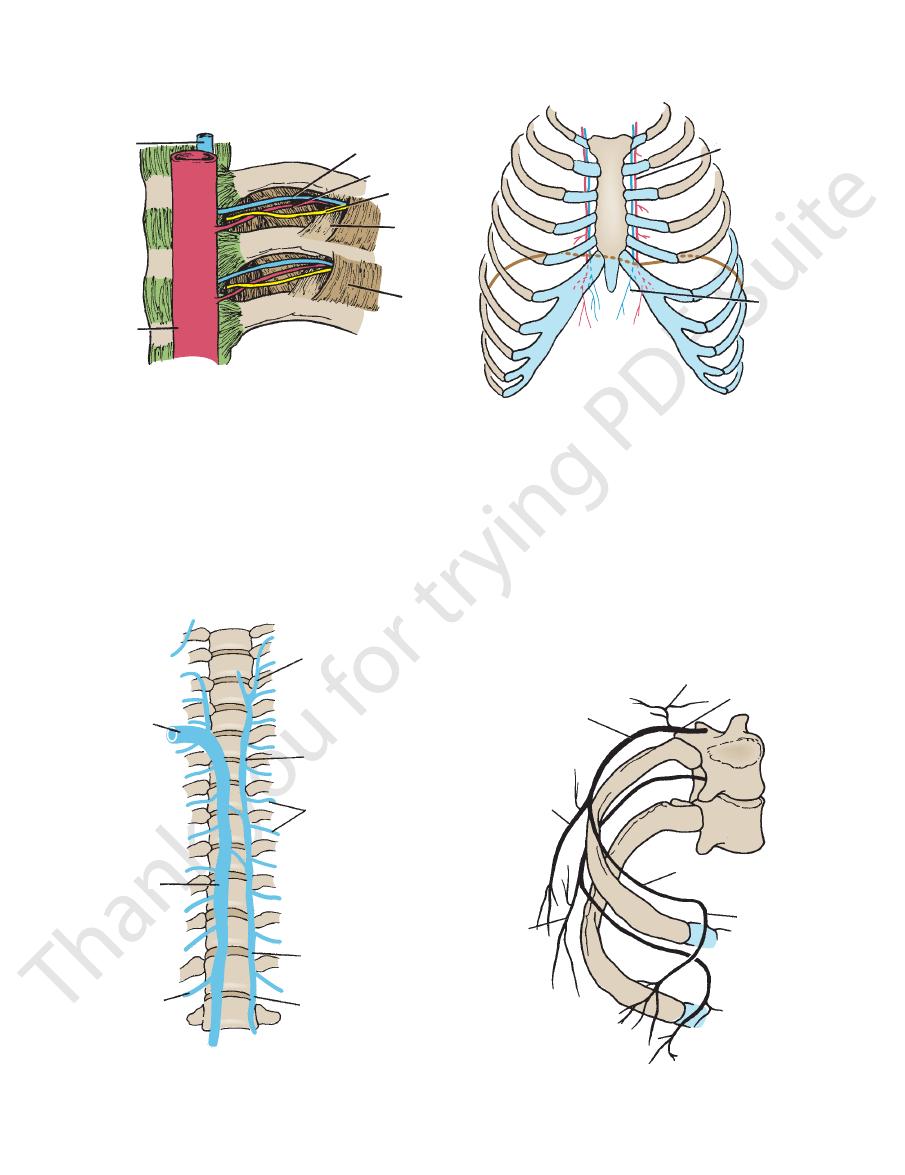
into the internal thoracic and the musculophrenic veins.
drain forward
anterior intercostal veins
and 2.11), and the
backward into the azygos or hemiazygos veins (Figs. 2.10
drain
posterior intercostal veins
The corresponding
ticularly large.
female, the branches to the superficial structures are par
skin, and parietal pleura. In the region of the breast in the
Each intercostal artery gives off branches to the muscles,
thoracic artery.
artery, one of the terminal branches of the internal
the lower spaces are branches of the musculophrenic
subclavian artery. The anterior intercostal arteries of
2.9 and 2.10), which arises from the first part of the
are branches of the internal thoracic artery (see Figs.
of the first six spaces
anterior intercostal arteries
The
aorta (Figs. 2.9 and 2.10).
nine spaces are branches of the descending thoracic
artery. The posterior intercostal arteries of the lower
branch of the costocervical trunk of the subclavian
are branches from the superior intercostal artery, a
of the first two spaces
posterior intercostal arteries
The
intercostal artery and two small anterior intercostal arteries.
Each intercostal space contains a large single posterior
Intercostal Arteries and Veins
costal vein, intercostal artery, and intercostal nerve (i.e., VAN).
arranged in the following order from above downward: inter
innermost layers of muscles (see Figs. 2.8 and 2.9). They are
bundle), as in the abdominal wall, run between the middle and
The intercostal nerves and blood vessels (the neurovascular
41
-
■
■
■
■
-
Intercostal Nerves
-
-
■
■
■
■
■
■
-
■
■
■
■
■
■
■
■
-
Skin Innervation of the Chest Wall and
with inflammation of the skin. In the thorax, the first symptom
in a patient who has previously had chickenpox. The lesion is
the abdominal musculature. The abdominal pain in these
give rise to abdominal pain and tenderness and rigidity of
nia with pleurisy involving the costal parietal pleura could
across the costal margin into the anterior abdominal wall.
wall may be revealed as pain in a dermatome that extends
importance because it means that disease in the thoracic
and parietal peritoneum. This latter fact is of great clinical
abdominal wall, muscles of the anterior abdominal wall,
that they, in addition, supply dermatomes on the anterior
thoracic wall and enter the anterior abdominal wall so
Furthermore, the 7th to 11th intercostal nerves leave the
muscles, and parietal pleura lining the intercostal space.
but also supplies the ribs, costal cartilages, intercostal
An intercostal nerve not only supplies areas of skin,
Referred Pain
Above the level of the sternal angle, the cutaneous innerva-
tion of the anterior chest wall is derived from the supracla-
vicular nerves (C3 and 4). Below this level, the anterior and
lateral cutaneous branches of the intercostal nerves supply
oblique bands of skin in regular sequence. The skin on the
posterior surface of the chest wall is supplied by the posterior
rami of the spinal nerves. The arrangement of the dermatomes
is shown in Figures 1.23 and 1.24.
For example, a pulmonary thromboembolism or a pneumo-
instances is called referred pain.
Herpes Zoster
Herpes zoster, or shingles, is a relatively common condition
caused by the reactivation of the latent varicella-zoster virus
seen as an inflammation and degeneration of the sensory neu-
ron in a cranial or spinal nerve with the formation of vesicles
is a band of dermatomal pain in the distribution of the sensory
neuron in a thoracic spinal nerve, followed in a few days by a
skin eruption. The condition occurs most frequently in patients
older than 50 years.
C L I N I C A L N O T E S
42
The Thorax: Part I—The Thoracic Wall
azygos vein
about to enter
superior vena
cava
azygos vein
right subcostal
vein
left superior
intercostal vein
superior hemiazygos
vein
posterior
intercostal veins
inferior hemiazygos
vein
left ascending lumbar
vein
FIGURE 2.11
The common arrangement of the azygos vein,
the inferior hemiazygos (hemiazygos) vein.
the superior hemiazygos (accessory hemiazygos) vein, and
superior
hemiazygos
vein
descending
thoracic
aorta
innermost
intercostal
muscle
internal
intercostal
muscle
intercostal
nerve
posterior
intercostal artery
posterior
intercostal vein
A
superior
epigastric
vessels
internal
thoracic
vessels
B
FIGURE 2.10
Anterior view of the chest showing the courses of the internal thoracic vessels. These vessels
been removed for clarity.
Internal view of the posterior end of two typical intercostal spaces; the posterior intercostal membrane has
A.
B.
descend about one fingerbreadth from the lateral margin of the sternum.
anterior ramus
posterior
ramus
second thoracic
spinal nerve
anterior
cutaneous
branch
lateral
cutaneous
branch
intercostobrachial
nerve
T3
T4
intercostal nerve
FIGURE 2.12
The distribution of two intercostal nerves
skin and the parietal peritoneum covering the outer and
In addition, the 7th to 11th intercostal nerves supply the
and the levatores costarum and serratus posterior muscles.
tively, and the intercostal muscles of each intercostal space
outer and inner surfaces of each intercostal space, respec
therefore supply the skin and the parietal pleura covering the
With the exceptions noted, the 1st six intercostal nerves
is referred along this nerve to the medial side of the arm.
coronary artery disease,
medial side of the arm. In
therefore supplies the skin of the armpit and the upper
neous branch of other nerves. The 2nd intercostal nerve
which is equivalent to the lateral cuta
costobrachial nerve,
inter
cutaneous nerve of the arm by a branch called the
is joined to the medial
second intercostal nerve
The
relative to the rib cage.
-
-
pain
-
Basic Anatomy
43
Intercostal Nerve Block
The skin and the parietal pleura cover the outer and inner sur
Area of Anesthesia
-
faces of each intercostal space, respectively; the 7th to 11th
intercostal nerves supply the skin and the parietal peritoneum
covering the outer and inner surfaces of the abdominal wall,
respectively. Therefore, an intercostal nerve block will also
anesthetize these areas. In addition, the periosteum of the adja-
cent ribs is anesthetized.
Indications
Intercostal nerve block is indicated for repair of lacerations of
the thoracic and abdominal walls, for relief of pain in rib frac-
tures, and to allow pain-free respiratory movements.
Procedure
To produce analgesia of the anterior and lateral thoracic and
abdominal walls, the intercostal nerve should be blocked before
the lateral cutaneous branch arises at the midaxillary line. The
ribs may be identified by counting down from the 2nd (opposite
sternal angle) or up from the 12th. The needle is directed toward
the rib near the lower border (see Fig. 2.8), and the tip comes
to rest near the subcostal groove, where the local anesthetic is
infiltrated around the nerve. Remember that the order of struc-
tures lying in the neurovascular bundle from above downward
is intercostal vein, artery, and nerve and that these structures
are situated between the posterior intercostal membrane of the
internal intercostal muscle and the parietal pleura. Furthermore,
laterally, the nerve lies between the internal intercostal muscle
and the innermost intercostal muscle.
Anatomy of Complications
Complications include pneumothorax and hemorrhage.
Pneumothorax can occur if the needle point misses the subcos-
tal groove and penetrates too deeply through the parietal pleura.
Hemorrhage is caused by the puncture of the intercostal
blood vessels. This is a common complication, so aspiration
should always be performed before injecting the anesthetic.
A small hematoma may result.
C L I N I C A L N O T E S
inner surfaces of the abdominal wall, respectively, and the
movements.
in intrathoracic pressure occurring during respiratory
tects the underlying cervical pleura and resists the changes
structures passing from the thorax into the neck. It pro
cervical vertebra and medially to the fascia investing the
its apex to the tip of the transverse process of the seventh
border of the 1st rib and costal cartilage. It is attached at
tent-shaped fibrous sheet is attached laterally to the medial
(Fig. 2.13). This
suprapleural membrane
layer called the
of these structures, the outlet is closed by a dense fascial
for the most part lie close to the midline. On either side
and the neck (esophagus, trachea, blood vessels, etc.) and
outlet transmits structures that pass between the thorax
(see page 39). The
thoracic outlet
a narrow aperture, the
Superiorly, the thorax opens into the root of the neck by
tus abdominis muscles.
oblique, internal oblique, transversus abdominis, and rec
anterior abdominal muscles, which include the external
-
Suprapleural Membrane
-
The shape of the thorax can be distorted by congenital anom
Thoracic Cage Distortion
-
alies of the vertebral column or by the ribs. Destructive dis-
ease of the vertebral column that produces lateral flexion or
scoliosis results in marked distortion of the thoracic cage.
C L I N I C A L N O T E S
Endothoracic Fascia
The suprapleural membrane is a thickening of this fascia.
sue that separates the parietal pleura from the thoracic wall.
The endothoracic fascia is a thin layer of loose connective tis-
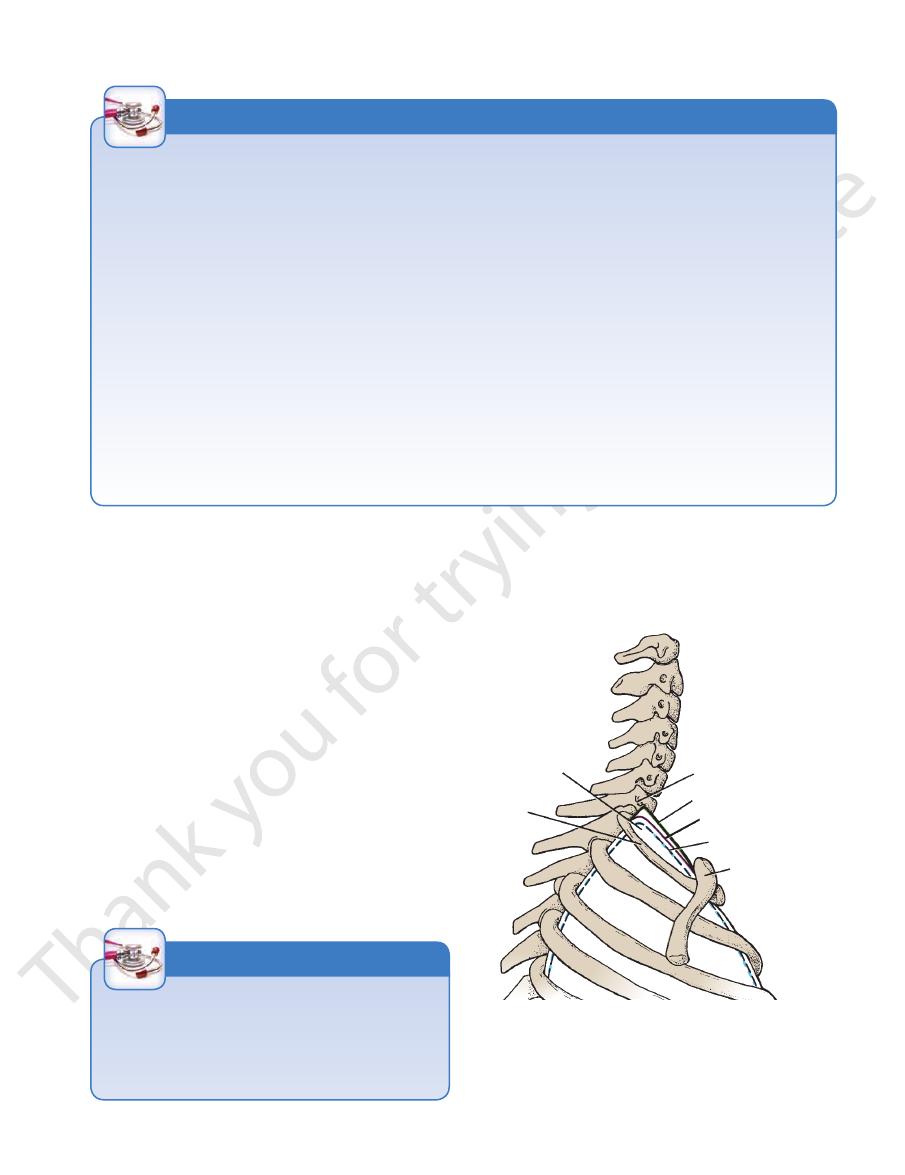
location of
apex of lung
first rib
transverse process of
seventh cervical vertebra
suprapleural membrane
parietal pleura
visceral pleura
clavicle
FIGURE 2.13
Lateral view of the upper opening of the
of the endothoracic fascia.
tected by the suprapleural membrane, which is a thickening
covered with visceral and parietal layers of pleura and is pro
superiorly into the root of the neck. The apex of the lung is
thoracic cage showing how the apex of the lung projects
-