44
(see Fig. 2.16).
stomach contents into the thoracic part of the esophagus
and possibly assist in the prevention of regurgitation of the
a slinglike loop. These fibers appear to act as a sphincter
pass up to the left and surround the esophageal orifice in
pericardium. Some of the muscle fibers of the right crus
don is partially fused with the inferior surface of the fibrous
is shaped like three leaves. The superior surface of the ten
which
central tendon,
The diaphragm is inserted into a
crosses over the anterior surface of the aorta (see Fig. 2.16).
which
median arcuate ligament,
crura are connected by a
lower border of the 12th rib. The medial borders of the two
of the transverse process of the first lumbar vertebra to the
vertebra. The lateral arcuate ligament extends from the tip
vertebra to the tip of the transverse process of the first lumbar
ment extends from the side of the body of the second lumbar
(see Fig. 2.16). The medial arcuate liga
arcuate ligaments
lateral
medial
the crura the diaphragm arises from the
vertebrae and the intervertebral disc (see Fig. 2.16). Lateral to
arises from the sides of the bodies of the first two lumbar
crus
left
three lumbar vertebrae and the intervertebral discs; the
arises from the sides of the bodies of the first
right crus
The
from the arcuate ligaments
arising by vertical columns or crura and
vertebral part
ribs and their costal cartilages (see Fig. 2.16)
arising from the deep surfaces of the lower six
costal part
xiphoid process (see Fig. 2.2)
arising from the posterior surface of the
sternal part
origin of the diaphragm can be divided into three parts:
opening, and a centrally placed tendon (see Fig. 2.16). The
cular part, which arises from the margins of the thoracic
tion. It is dome shaped and consists of a peripheral mus
The diaphragm is the most important muscle of respira
pass between the chest and the abdomen.
cavity below (Fig. 2.16). It is pierced by the structures that
that separates the chest cavity above from the abdominal
The diaphragm is a thin muscular and tendinous septum
The Thorax: Part I—The Thoracic Wall
Diaphragm
-
-
A
A
A
and
-
-
Traumatic Injury to the Thorax
When the anatomy of the thorax is reviewed, it is important to
ula, which overlies the upper seven ribs. This bone is covered
of a vertebral fracture with associated injury to the spinal cord
tebral column. In severe posterior chest injuries, the possibility
is sucked in during inspiration and driven out during expiration,
case, the stability of the chest wall is lost, and the flail segment
either side of the sternum, the sternum may be flail. In either
nected to the rest of the thoracic wall. If the fractures occur on
and anteriorly near the costochondral junctions. This causes
ited to one side, the fractures may occur near the rib angles
patient to breathe adequately, it may be necessary to relieve the
Severe localized pain is usually the most important symptom
jagged ends of a fractured rib may penetrate the lungs and pres
and the delicate pleura internally, it is not surprising that the
Because the rib is sandwiched between the skin externally
posteriorly. The 11th and 12th ribs float and move with the force of
muscles anteriorly and by the scapula and its associated muscles
ribs. The first four ribs are protected by the clavicle and pectoral
tively fixed. Ribs 5 through 10 are the most commonly fractured
may be injured. With increasing age, the rib cage becomes more
can be easily compressed so that the underlying lungs and heart
Fractures of the ribs are common chest injuries. In children,
Traumatic injury to the thorax is common, especially as a result
of automobile accidents.
Fractured Sternum
The sternum is a resilient structure that is held in position by
relatively pliable costal cartilages and bendable ribs. For these
reasons, fracture of the sternum is not common; however, it does
occur in high-speed motor vehicle accidents. Remember that the
heart lies posterior to the sternum and may be severely contused
by the sternum on impact.
Rib Contusion
Bruising of a rib, secondary to trauma, is the most common
rib injury. In this painful condition, a small hemorrhage occurs
beneath the periosteum.
Rib Fractures
the ribs are highly elastic, and fractures in this age group are
therefore rare. Unfortunately, the pliable chest wall in the young
rigid, owing to the deposit of calcium in the costal cartilages, and
the ribs become brittle. The ribs then tend to break at their weak-
est part, their angles.
The ribs prone to fracture are those that are exposed or rela-
impact.
-
ent as a pneumothorax.
of a fractured rib. The periosteum of each rib is innervated by the
intercostal nerves above and below the rib. To encourage the
pain by performing an intercostal nerve block.
Flail Chest
In severe crush injuries, a number of ribs may break. If lim-
flail chest, in which a section of the chest wall is discon-
producing paradoxical and ineffective respiratory movements.
Traumatic Injury to the Back of the Chest
The posterior wall of the chest in the midline is formed by the ver-
should be considered. Remember also the presence of the scap-
with muscles and is fractured only in cases of severe trauma.
Traumatic Injury to the Abdominal Viscera
and the Chest
remember that the upper abdominal organs—namely, the liver,
stomach, and spleen—may be injured by trauma to the rib cage.
In fact, any injury to the chest below the level of the nipple line
may involve abdominal organs as well as chest organs.
C L I N I C A L N O T E S
Basic Anatomy
the heart. Lymph within the abdominal lymph vessels is
vena cava and forces it upward into the right atrium of
pressure change compresses the blood in the inferior
same time increases the intra-abdominal pressure. This
phragm decreases the intrathoracic pressure and at the
The descent of the dia
Thoracoabdominal pump:
the bladder and anal canal under these circumstances.
it is important to have adequate sphincteric control of
muscles in the lifting of heavy weights. Needless to say,
prevent flexion. This greatly assists the postvertebral
extent that it helps support the vertebral column and
wall in raising the intra-abdominal pressure to such an
phragm assists the muscles of the anterior abdominal
breath and holding it (fixing the diaphragm), the dia
In a person taking a deep
Weight-lifting muscle:
escape, producing a grunting sound.
in the respiratory tract. Now and again, air is allowed to
diaphragm is unable to rise because of the air trapped
a deep breath and closing the glottis of the larynx. The
This mechanism is further aided by the person taking
pressure for micturition, defecation, and parturition.
anterior abdominal wall in raising the intra-abdominal
diaphragm assists the contraction of the muscles of the
The contraction of the
Muscle of abdominal straining:
important muscle used in inspiration.
cal diameter of the thorax. The diaphragm is the most
pulls its central tendon down and increases the verti
On contraction, the diaphragm
Muscle of inspiration:
Functions of the Diaphragm
don and increases the vertical diameter of the thorax.
On contraction, the diaphragm pulls down its central ten
Action of the Diaphragm
from the lower six intercostal nerves.
the phrenic nerve and the periphery of the diaphragm is
covering the central surfaces of the diaphragm are from
The parietal pleura and peritoneum
Sensory nerve supply:
(C3, 4, 5).
The right and left phrenic nerves
Motor nerve supply:
Nerve Supply of the Diaphragm
the xiphoid process (see Fig. 2.2).
vertebral column and the short limb extending forward to
ance of an inverted J, the long limb extending up from the
When seen from the side, the diaphragm has the appear
ing; it is higher in the supine position and after a large meal.
The diaphragm is lower when a person is sitting or stand
ture, and the degree of distention of the abdominal viscera.
the diaphragm vary with the phase of respiration, the pos
whereas the central tendon supports the heart. The levels of
sternal joint. The domes support the right and left lungs,
the liver.) The central tendon lies at the level of the xiphi
at a higher level, because of the large size of the right lobe of
reach the lower border of the 5th rib. (The right dome lies
as the upper border of the 5th rib, and the left dome may
or cupulae. The right dome reaches as high
and left domes,
right
As seen from in front, the diaphragm curves up into
Shape of the Diaphragm
45
-
-
-
-
-
■
■
-
■
■
■
■
-
■
■
-
Needle Thoracostomy
right). Avoid damaging the diaphragm and entering the perito
the lower intercostal spaces is possible provided that the pres
the bundle passes forward to the rib angle, it becomes closely
The preferred insertion site for a tube thoracostomy is the fourth
(d) external intercostal muscle, (e) internal intercostal muscle, (f)
toral muscles are then penetrated), (c) serratus anterior muscle,
ing structures as it passes through the chest wall (see Fig. 2.8):
The skin is prepared in the usual way, and a local anesthetic
the 2nd rib, and the second intercostal space are found in the
For the anterior approach, the patient is in the supine position.
drain fluid (blood or pus) away from the pleural cavity to allow
A needle thoracostomy is necessary in patients with tension
pneumothorax (air in the pleural cavity under pressure) or to
the lung to reexpand. It may also be necessary to withdraw a
sample of pleural fluid for microbiologic examination.
Anterior Approach
The sternal angle is identified, and then the 2nd costal cartilage,
midclavicular line.
Lateral Approach
For the lateral approach, the patient is lying on the lateral side.
The 2nd intercostal space is identified as above, but the anterior
axillary line is used.
is introduced along the course of the needle above the upper bor-
der of the 3rd rib. The thoracostomy needle will pierce the follow-
(a) skin, (b) superficial fascia (in the anterior approach the pec-
innermost intercostal muscle, (g) endothoracic fascia, and (h) pari-
etal pleura.
The needle should be kept close to the upper border of the
3rd rib to avoid injuring the intercostal vessels and nerve in the
subcostal groove.
Tube Thoracostomy
or fifth intercostal space at the anterior axillary line (Fig. 2.14).
The tube is introduced through a small incision. The neurovas-
cular bundle changes its relationship to the ribs as it passes for-
ward in the intercostal space. In the most posterior part of the
space, the bundle lies in the middle of the intercostal space. As
related to the lower border of the rib above and maintains that
position as it courses forward.
The introduction of a thoracostomy tube or needle through
-
ence of the domes of the diaphragm is remembered as they
curve upward into the rib cage as far as the 5th rib (higher on the
-
neal cavity and injuring the liver, spleen, or stomach.
C L I N I C A L N O T E S
(continued)
46
first part of the subclavian artery in the neck. It descends
body from the clavicle to the umbilicus. It is a branch of the
The internal thoracic artery supplies the anterior wall of the
tal origins of the diaphragm on each side (see Fig. 2.16).
superior epigastric vessels pass between the sternal and cos
terior to the medial arcuate ligament on each side; and the
nerves pierce the crura; the sympathetic trunks pass pos
In addition to these openings, the sympathetic splanchnic
right phrenic nerve.
mits the inferior vena cava and terminal branches of the
vertebra in the central tendon (see Fig. 2.16). It trans
lies at the level of the 8th thoracic
caval opening
The
third of the esophagus.
the left gastric vessels, and the lymphatics from the lower
right and left vagus nerves, the esophageal branches of
right crus (see Fig. 2.16). It transmits the esophagus, the
racic vertebra in a sling of muscle fibers derived from the
lies at the level of the 10th tho
esophageal opening
The
transmits the aorta, the thoracic duct, and the azygos vein.
thoracic vertebra between the crura (see Fig. 2.16). It
lies anterior to the body of the 12th
aortic opening
The
The diaphragm has three main openings:
backflow.
The presence of valves within the thoracic duct prevents
racic duct is aided by the negative intrathoracic pressure.
also compressed, and its passage upward within the tho
The Thorax: Part I—The Thoracic Wall
-
Openings in the Diaphragm
■
■
■
■
-
■
■
-
-
-
Internal Thoracic Artery
vertically on the pleura behind the costal cartilages, a
fingerbreadth lateral to the sternum, and ends in the sixth
verse process and is inserted into the rib below.
lar in shape and arises by its apex from the tip of the trans
There are 12 pairs of muscles. Each levator costa is triangu
each side.
racic artery and drains into the brachiocephalic vein on
The internal thoracic vein accompanies the internal tho
Internal Thoracic Vein
intercostal spaces and the diaphragm
costal margin of the diaphragm and supplies the lower
which runs around the
musculophrenic artery,
The
rectus muscle as far as the umbilicus
sheath of the anterior abdominal wall and supplies the
which enters the rectus
superior epigastric artery,
The
mediastinum (e.g., the thymus)
to the contents of the anterior
Mediastinal arteries
the phrenic nerve and supplies the pericardium
which accompanies
pericardiacophrenic artery,
The
branches of the corresponding intercostal nerves
which accompany the terminal
Perforating arteries,
costal spaces
for the upper six inter
anterior intercostal arteries
Two
Branches
and musculophrenic arteries (see Figs. 2.9 and 2.10).
intercostal space by dividing into the superior epigastric
■
■
-
■
■
■
■
■
■
■
■
■
■
-
Levatores Costarum
-
-
Thoracotomy
to the diaphragm until proved otherwise. The arching domes of
circumstances, the nerve to the subclavius muscle must also
To obtain complete paralysis under these
sory phrenic nerve.
cal spinal nerve joins the phrenic nerve late as a branch from
when the physician wishes to rest the lower lobe of the lung
essary in the treatment of certain forms of lung tuberculosis,
A single dome of the diaphragm may be paralyzed by crushing
however, be a symptom of disease such as pleurisy, peritonitis,
Hiccup is the involuntary spasmodic contraction of the dia
intercostal muscle, (g) endothoracic fascia, and (h) parietal
costal membrane, (e) internal intercostal muscle, (f) innermost
side. The following tissues will be incised (see Fig. 2.14): (a)
heart and the aorta, the chest should be entered from the left
left incision depends on the site of the injury. For access to the
the anterior axillary line (Fig. 2.15). Whether to make a right or
tal space, extending from the lateral margin of the sternum to
ing procedure. After preparing the skin in the usual way, the
In patients with penetrating chest wounds with uncontrolled
intrathoracic hemorrhage, thoracotomy may be a life-sav-
physician makes an incision over the fourth or fifth intercos-
skin, (b) subcutaneous tissue, (c) serratus anterior and pecto-
ral muscles, (d) external intercostal muscle and anterior inter-
pleura.
Avoid the internal thoracic artery, which runs vertically
downward behind the costal cartilages about a fingerbreadth
lateral to the margin of the sternum, and the intercostal vessels
and nerve, which extend forward in the subcostal groove in the
upper part of the intercostal space (see Fig. 2.14).
Hiccup
-
phragm accompanied by the approximation of the vocal folds
and closure of the glottis of the larynx. It is a common condition
in normal individuals and occurs after eating or drinking as a
result of gastric irritation of the vagus nerve endings. It may,
pericarditis, or uremia.
Paralysis of the Diaphragm
or sectioning of the phrenic nerve in the neck. This may be nec-
on one side. Occasionally, the contribution from the fifth cervi-
the nerve to the subclavius muscle. This is known as the acces-
be sectioned.
Penetrating Injuries of the Diaphragm
Penetrating injuries can result from stab or bullet wounds to the
chest or abdomen. Any penetrating wound to the chest below
the level of the nipples should be suspected of causing damage
the diaphragm can reach the level of the 5th rib (the right dome
can reach a higher level).
Basic Anatomy
47
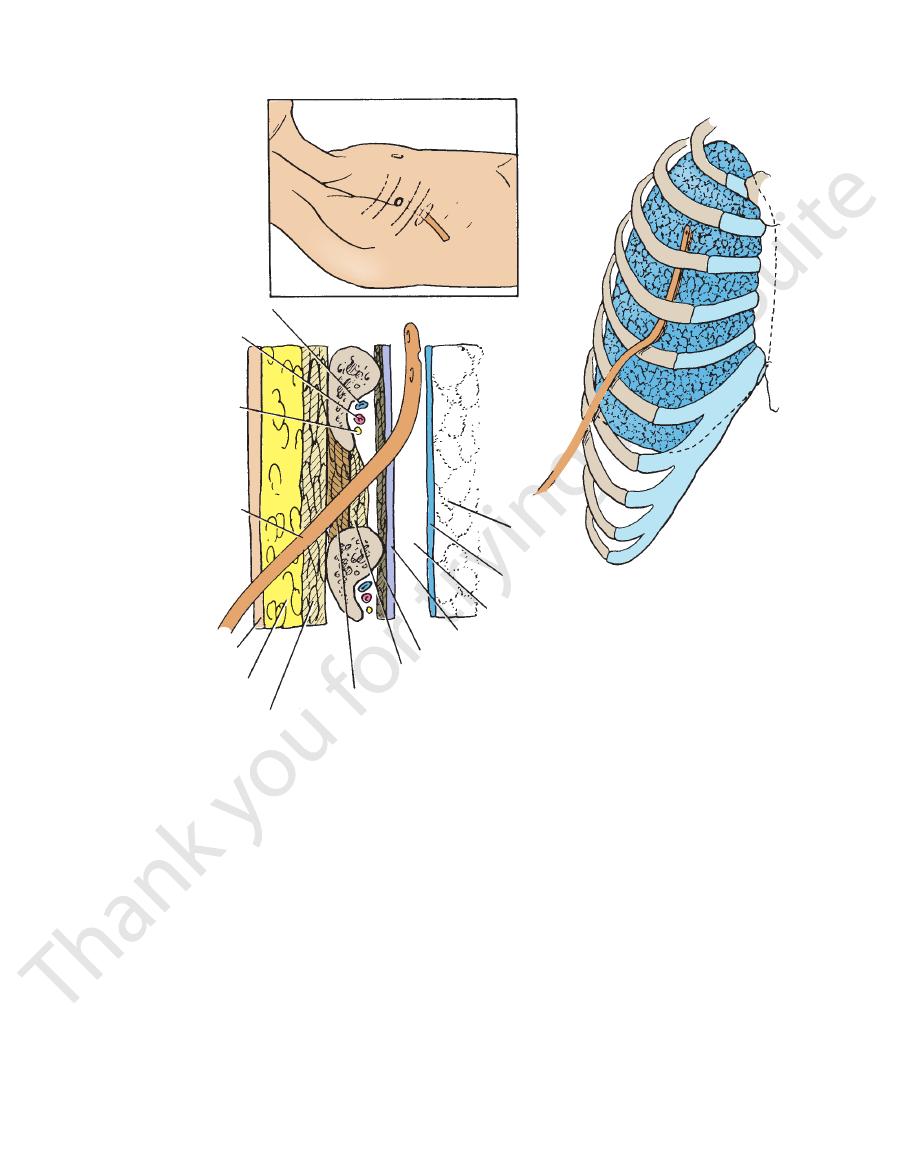
intercostal vein
4
intercostal artery
intercostal nerve
tube
superficial fascia
serratus anterior
external
intercostal
internal intercostal
innermost intercostal
parietal pleura
pleural cavity (space)
visceral pleura
lung
B
A
C
5
4
5
skin
4
5
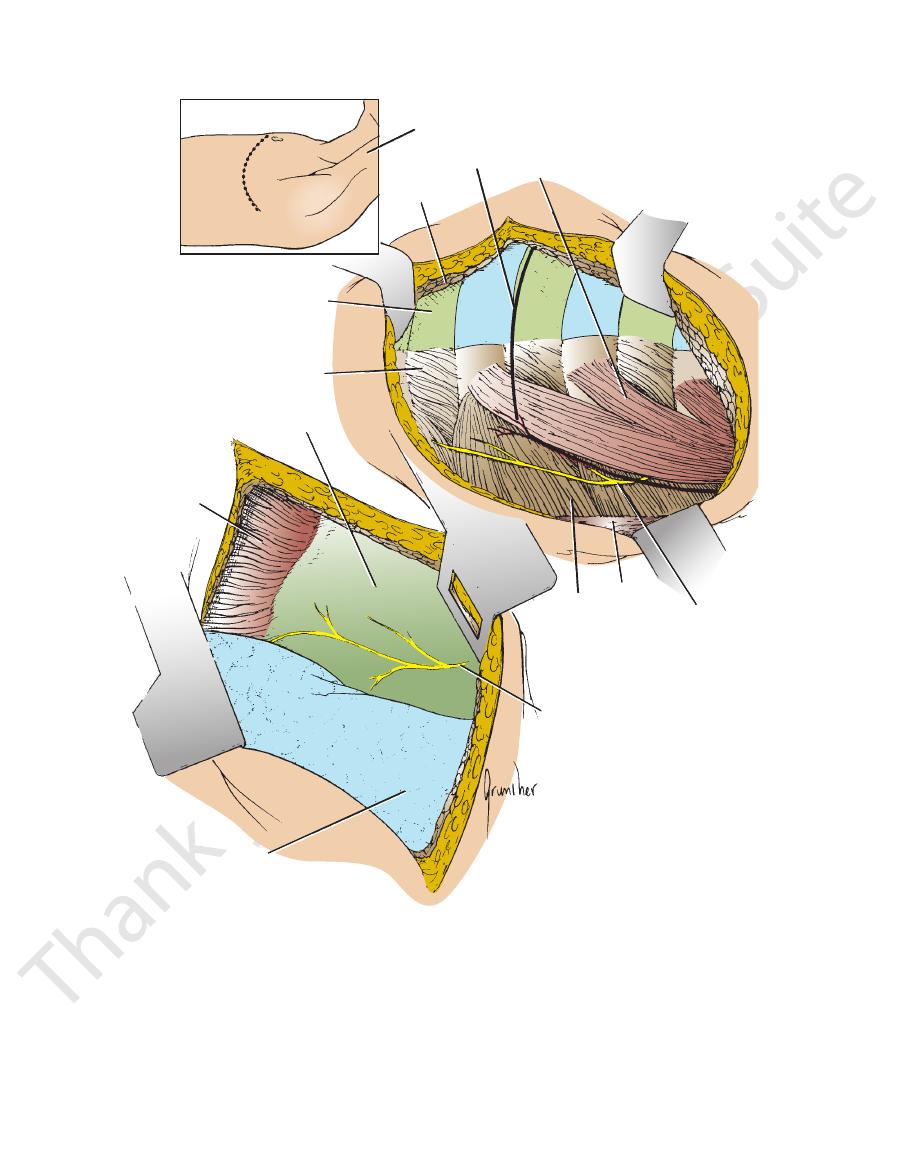
FIGURE 2.14
Tube thoracostomy.
and their actions is given in Table 2.1.
A summary of the muscles of the thorax, their nerve supply,
Intercostal nerves.
Nerve supply:
tory muscle.
It depresses the ribs and is therefore an expira
Action:
the lower ribs.
Its fibers pass upward and laterally and are inserted into
arises from the upper lumbar and lower thoracic spines.
The serratus posterior inferior is a thin, flat muscle that
Intercostal nerves.
Nerve supply:
muscle.
It elevates the ribs and is therefore an inspiratory
Action:
the upper ribs.
Its fibers pass downward and laterally and are inserted into
arises from the lower cervical and upper thoracic spines.
The serratus posterior superior is a thin, flat muscle that
Posterior rami of thoracic spinal nerves.
Nerve supply:
inspiratory muscle.
Each raises the rib below and is therefore an
Action:
The tube advancing
space is kept close to the upper border of the rib to avoid injuring the intercostal vessels and nerve.
and later the tube as they pass through the chest wall to enter the pleural cavity (space). The incision through the intercostal
The various layers of tissue penetrated by the scalpel
made over the intercostal space one below the space to be pierced.
The site for insertion of the tube at the anterior axillary line. The skin incision is usually
A.
B.
C.
superiorly and posteriorly in the pleural space.
■
■
■
■
Serratus Posterior Superior Muscle
■
■
■
■
Serratus Posterior Inferior Muscle
■
■
-
■
■
48
The Thorax: Part I—The Thoracic Wall
A
neck
line of
incision
4
5
pectoralis
minor
pectoralis
major
left lung
diaphragm
pericardium
anterior intercostal
membrane
external intercostal
muscle
3
left phrenic nerve
serratus
anterior
latissimus
dorsi
long thoracic
nerve
B
C
FIGURE 2.15
Left thoracotomy.
the way to visualize the mediastinum.
phrenic nerve descends over the pericardium beneath the mediastinal pleura. The collapsed left lung must be pushed out of
The pleural space opened and the left side of the mediastinum exposed. The left
injuring the intercostal vessels and nerve.
ated muscles. The line of incision through the intercostal space should be placed close to the upper border of the rib to avoid
The exposed ribs and associ
Site of skin incision over fourth or fifth intercostal space.
A.
B.
-
C.
Basic Anatomy
49
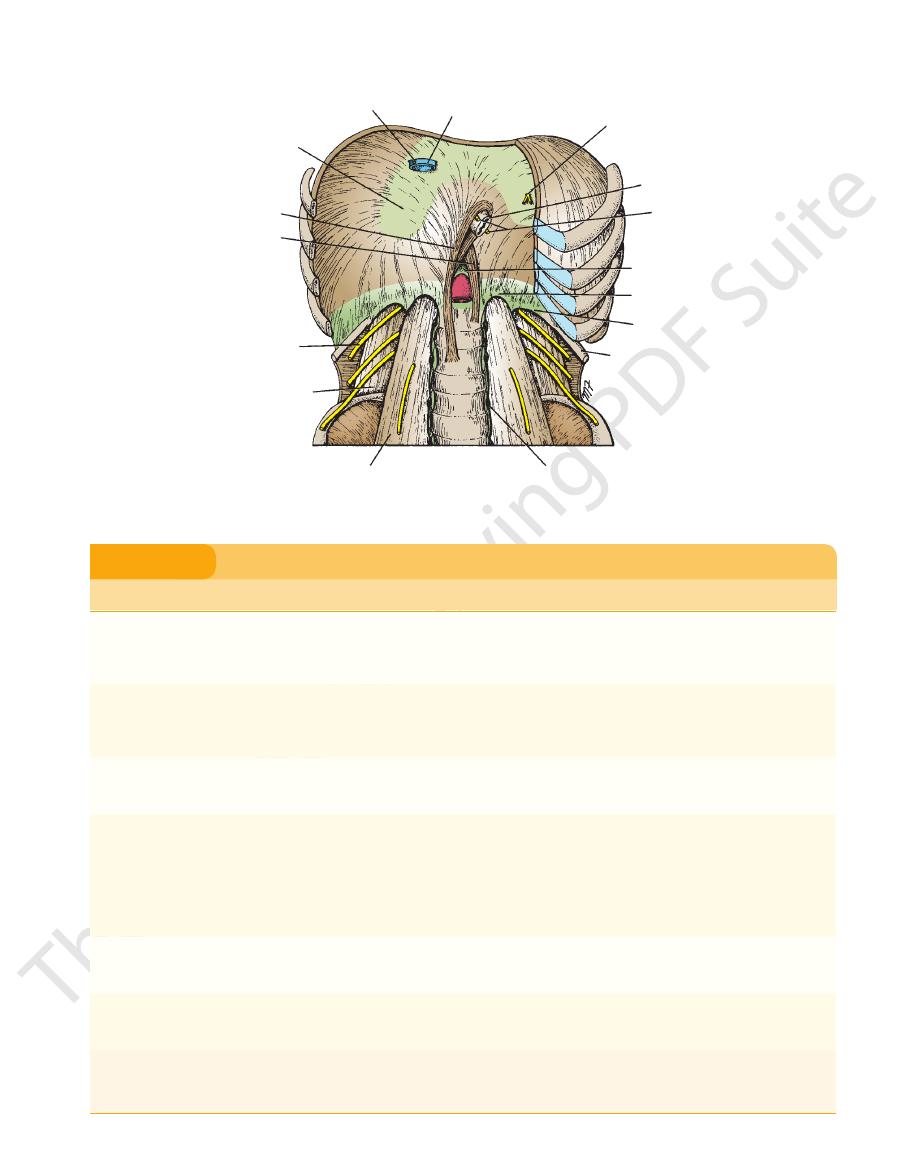
right phrenic nerve
inferior vena cava
left phrenic nerve
esophagus
vagi
median arcuate ligament
medial arcuate ligament
12th rib
sympathetic trunk
psoas muscle
quadratus lumborum muscle
subcostal nerve
left crus
right crus
central tendon
lateral arcuate ligament
FIGURE 2.16
he anterior portion of the right side has been removed. Note the sternal, cos
Diaphragm as seen from below. T
tal, and vertebral origins of the muscle and the important structures that pass through it.
-
Tip of transverse
Very important muscle of
Name of Muscle
Origin
Insertion
Nerve Supply
Action
External intercostal
muscle (11) (fibers pass
downward and forward)
Inferior border of rib
Superior border of
rib below
Intercostal nerves
With 1st rib fixed, they raise ribs
during inspiration and thus
increase anteroposterior and
transverse diameters of thorax
Internal intercostal
muscle (11) (fibers
pass downward and
backward)
Inferior border of rib
Superior border of
rib below
Intercostal nerves
With last rib fixed by abdominal
muscles, they lower ribs during
expiration
Innermost intercostal
muscle (incomplete
layer)
Adjacent ribs
Adjacent ribs
Intercostal nerves
Assists external and internal
intercostal muscles
Diaphragm (most important
muscle of respiration)
Xiphoid process;
lower six costal
cartilages, first
three lumbar
vertebrae
Central tendon
Phrenic nerve
inspiration; increases vertical
diameter of thorax by pulling
central tendon downward;
assists in raising lower ribs
Also used in abdominal straining
and weight lifting
Levatores costarum (12)
process of C7 and
T1–11 vertebrae
Rib below
Posterior rami of
thoracic spinal
nerves
Raises ribs and therefore
inspiratory muscles
Serratus posterior superior
Lower cervical and
upper thoracic
spines
Upper ribs
Intercostal nerves
Raises ribs and therefore
inspiratory muscles
Serratus posterior inferior
Upper lumbar and
lower thoracic
spines
Lower ribs
Intercostal nerves
Depresses ribs and therefore
expiratory muscles
Muscles of the Thorax
T A B L E 2 . 1