
and fetal asphyxia especially cause these attempted respiratory movements.
take place beginning at the end of the first trimester of pregnancy. Tactile stimuli
to breathe in the amniotic cavity. However, attempted respiratory movements do
Respiratory System.
lymphocyte and plasma cell production in lymphoid tissue.
of the red blood cells as well as most of the white blood cells, except for continued
from the third month on, the bone marrow gradually becomes the principal source
the spleen and other lymphoid tissues of the body begin forming blood cells. Finally,
vessels. Then, at 6 weeks, the liver begins to form blood cells, and in the third month,
This is followed 1 week later (at 4 to 5 weeks) by formation of non-nucleated red
tilization, contracting at a rate of about 65 beats/min. This increases steadily to about
The human heart begins beating during the fourth week after fer-
Circulatory System.
liver, lack full development, as discussed in more detail later in the chapter.
at birth, certain structures, particularly in the nervous system, the kidneys, and the
requires the full remaining 5 months of pregnancy for complete development. Even
However, cellular development in each organ is usually far from complete and
month 4, the organs of the fetus are grossly the same as those of the neonate.
to 3 months, most of the details of the different organs are established. Beyond
different organs of the fetus have already begun to develop, and during the next 2
Within 1 month after fertilization of the ovum, the gross characteristics of all the
pounds in normal infants with normal gestational periods.
birth, the weight averages 3 pounds, 1 month before birth 4.5 pounds, and at birth
last trimester of pregnancy, the fetus gains tremendously, so that 2 months before
months) of gestation. Then, during the
and reaches 1 pound only at 23 weeks (5
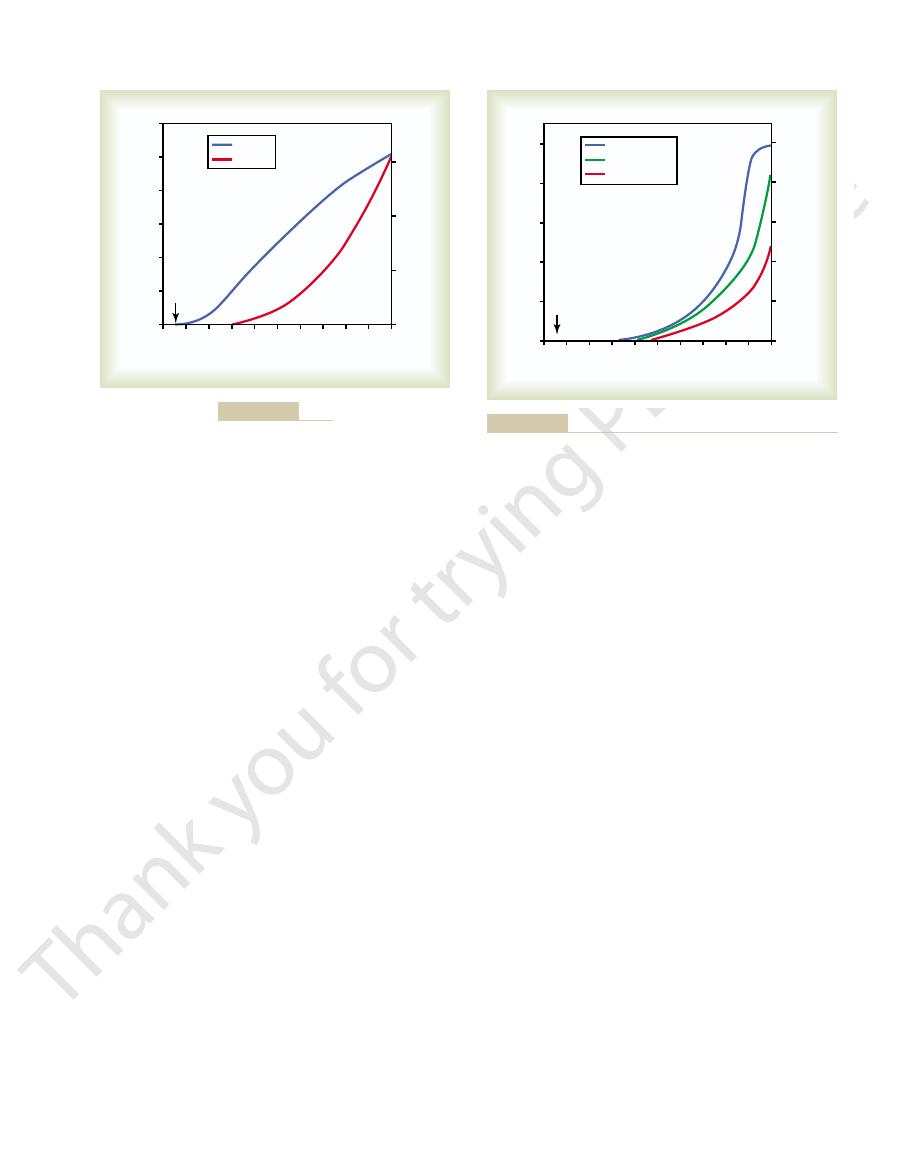
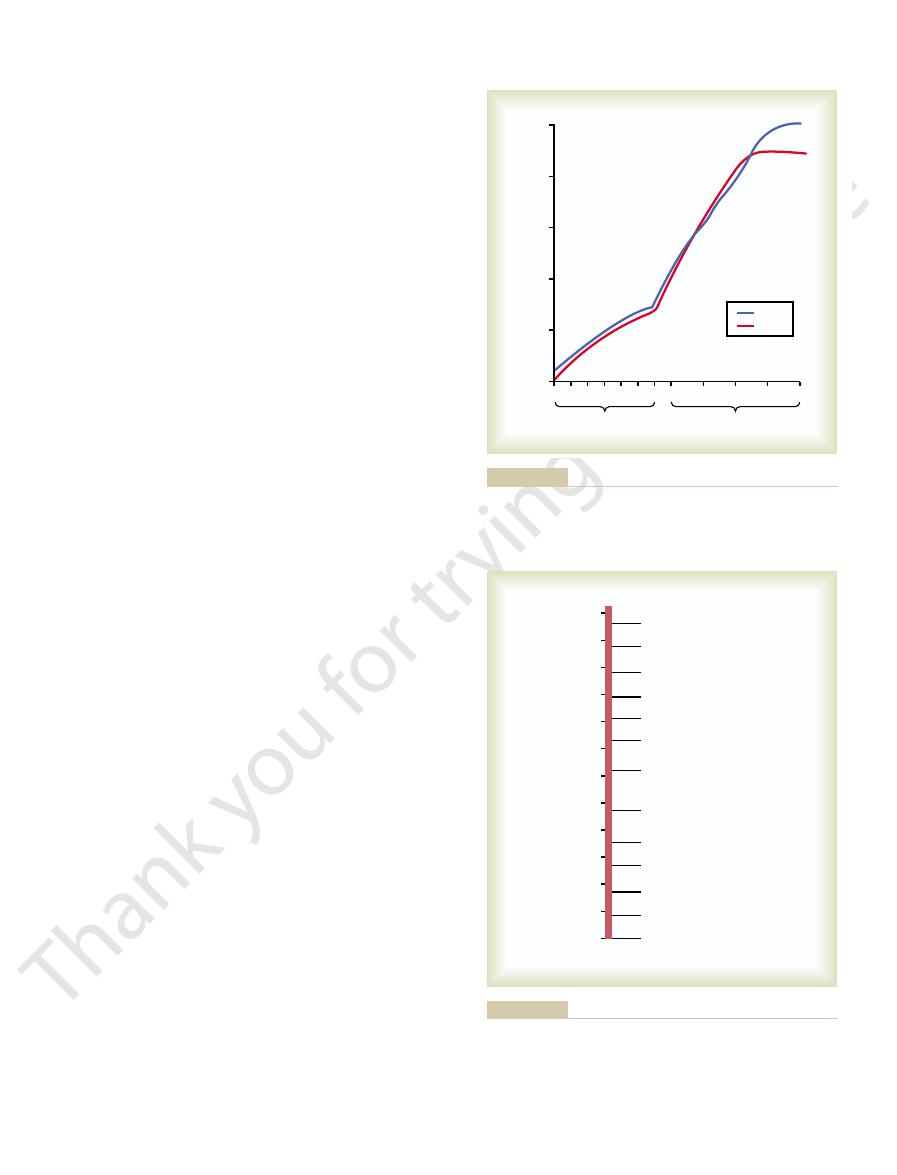
Note in Figure 83–1 that the weight remains minuscule during the first 12 weeks
almost in proportion to the cube of the age of the fetus.
fetus is approximately proportional to the cube of length, the weight increases
and at term (40 weeks), 53 centimeters (about 21 inches). Because the weight of the
age. At 12 weeks, the length is about 10 centimeters; at 20 weeks, 25 centimeters;
as shown in Figure 83–1, the length of the fetus increases almost in proportion to
implantation of the blastocyst, the fetus remains almost microscopic, but thereafter,
than development of the fetus itself. In fact, during the first 2 to 3 weeks after
Growth and Functional Development
important of these.
liar to the infant itself. This chapter discusses the more
atrics. However, many physiologic principles are pecu-
ing of the child immediately after birth, and growth and
A complete discussion of fetal development, function-
Fetal and Neonatal Physiology
C
H
A
P
T
E
R
8
3
1042
development through the early years of life lies within
the province of formal courses in obstetrics and pedi-
of the Fetus
Initial development of the placenta and fetal membranes occurs far more rapidly
1
/
2
7 pounds—the final birth weight varying from as low as 4.5 pounds to as high as 11
Development of the Organ Systems
140 beats/min immediately before birth.
Formation of Blood Cells.
Nucleated red blood cells begin to be formed in the yolk sac
and mesothelial layers of the placenta at about the third week of fetal development.
blood cells by the fetal mesenchyme and also by the endothelium of the fetal blood
Respiration cannot occur during fetal life because there is no air
before implantation of the ovum; this iron is ingested
mother’s uterine progestational endometrium even
hemoglobin, which begins to be formed as early as the
and phosphate. Most of the iron is in the form of
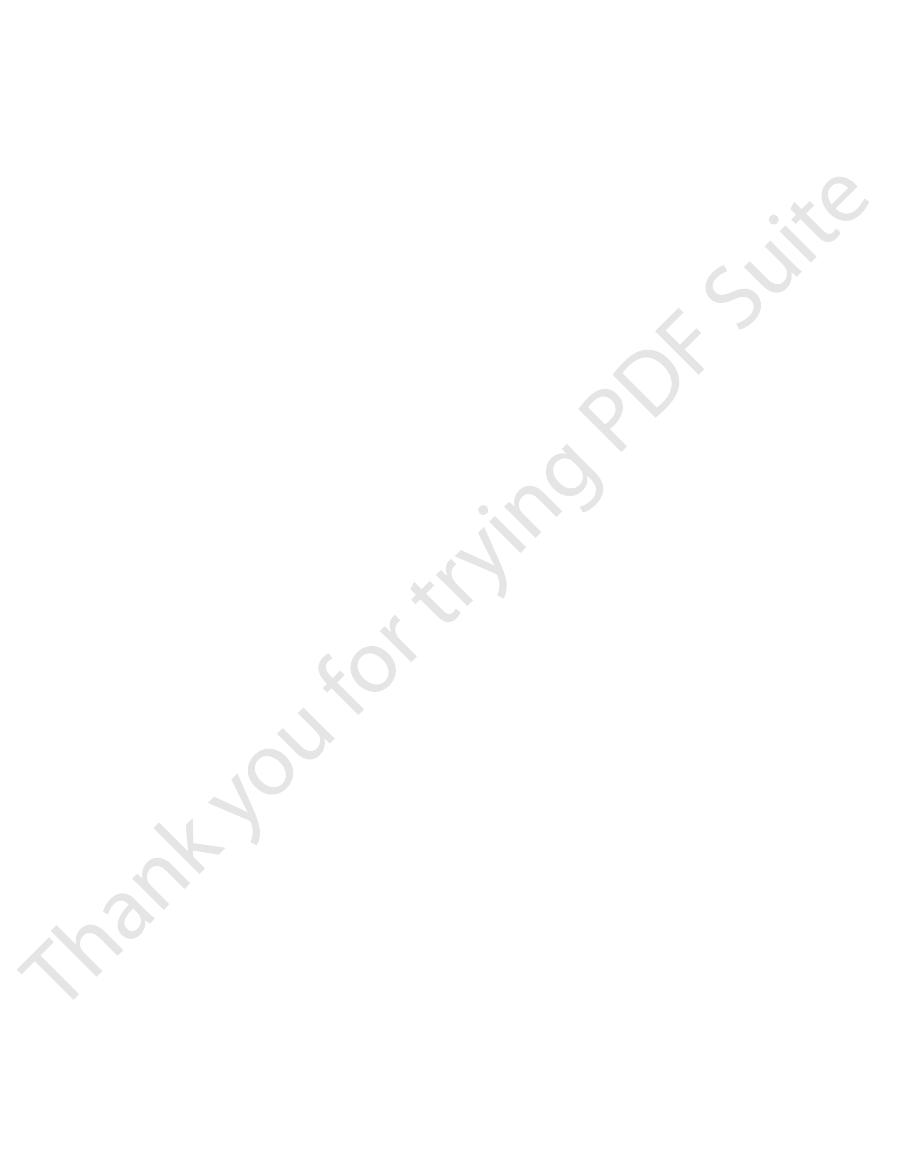
Figure 83–2 also shows that iron
minimal drain from the mother. Much greater drain
substances in the mother’s bones. Therefore, this is a
ossification until after the fourth month of pregnancy.
matrix. Indeed x-ray films ordinarily do not show any
During the earlier part of fetal life, the bones are
the fetus.
accumulate during the last 4 weeks of gestation, which
average fetus during gestation. About one half of these
fetus, demonstrating that about 22.5 grams of calcium
Figure 83–2 shows
tion to calcium, phosphate, iron, and some vitamins.
the mother’s blood. In addition to these generalities,
protein, much if not most of the fat being synthesized
energy, and it has a high capability to store fat and
The fetus uses mainly glucose for
base balance, are almost nonexistent until late fetal life
volume and electrolyte balances, and especially acid-
Although the fetal kidneys form urine, the renal
for about 70 to 80 per cent of the amniotic fluid. Abnor-
the second trimester pregnancy, and fetal urine accounts
The fetal kidneys begin to excrete urine during
ucts from the gastrointestinal mucosa and glands.
the anus into the amniotic fluid. Meconium is composed
that time, small quantities of
function approaches that of the normal neonate. By
and during the last 2 to 3 months, gastrointestinal
By midpregnancy, the fetus begins
Tract
only after about 1 year of postnatal life.
development even at birth. Indeed, myelinization of
However, those nervous system functions that involve
present by the third to fourth months of pregnancy.
Nervous System.
thus keeping only clean fluid in the lungs.
Also, small amounts of fluid are secreted into the lungs
the fetus’s gastrointestinal tract into the amniotic fluid.
pletely deflated. The inhibition of respiration during the
for reasons unknown, and the lungs remain almost com-
During the last 3 to 4 months of pregnancy, the res-
Fetal and Neonatal Physiology
Chapter 83
1043
piratory movements of the fetus are mainly inhibited,
later months of fetal life prevents filling of the lungs
with fluid and debris from the meconium excreted by
by the alveolar epithelium up until the moment of birth,
Most of the reflexes of the fetus that
involve the spinal cord and even the brain stem are
the cerebral cortex are still only in the early stages of
some major tracts of the brain itself becomes complete
Gastrointestinal.
to ingest and absorb large quantities of amniotic fluid,
meconium are continually
formed in the gastrointestinal tract and excreted from
partly of residue from swallowed amniotic fluid and
partly of mucus and other residues of excretory prod-
Kidneys.
mal kidney development or severe impairment of
kidney function in the fetus greatly reduce the forma-
tion of amniotic fluid (oligohydramnios) and can lead to
fetal death.
control systems for regulating fetal extracellular fluid
and do not reach full development until a few months
after birth.
Fetal Metabolism.
from glucose rather than being absorbed directly from
there are special problems of fetal metabolism in rela-
Metabolism of Calcium and Phosphate.
the rates of calcium and phosphate accumulation in the
and 13.5 grams of phosphorus are accumulated in the
is coincident with the period of rapid ossification of the
fetal bones and with the period of rapid weight gain of
relatively unossified and have mainly a cartilaginous
Note especially that the total amounts of calcium and
phosphate needed by the fetus during gestation repre-
sent only about 2 per cent of the quantities of these
occurs after birth during lactation.
Accumulation of Iron.
accumulates in the fetus even more rapidly than calcium
third week after fertilization of the ovum.
Small amounts of iron are concentrated in the
into the embryo by the trophoblastic cells and is used
Weight
0
36
32
28
24
20
16
12
8
4
Ovulation
Parturition
40
50
Length
40
30
20
10
0
2
1
3
0
Age of fetus (weeks after last menstruation)
Length (centimeters)
Weight (Kilograms)
Growth of the fetus.
Figure 83–1
0
4
8
12 16 20 24 28 32 36 40
Ovulation
Parturition
25
20
15
10
5
0
Iron
Calcium
Phosphorus
0
250
200
150
50
100
Age of fetus (weeks after last menstruation)
Grams of calcium or phosphorus stored
Milligrams of iron stored
Iron, calcium, and phosphorus storage in the fetus at different
Figure 83–2
stages of gestation.
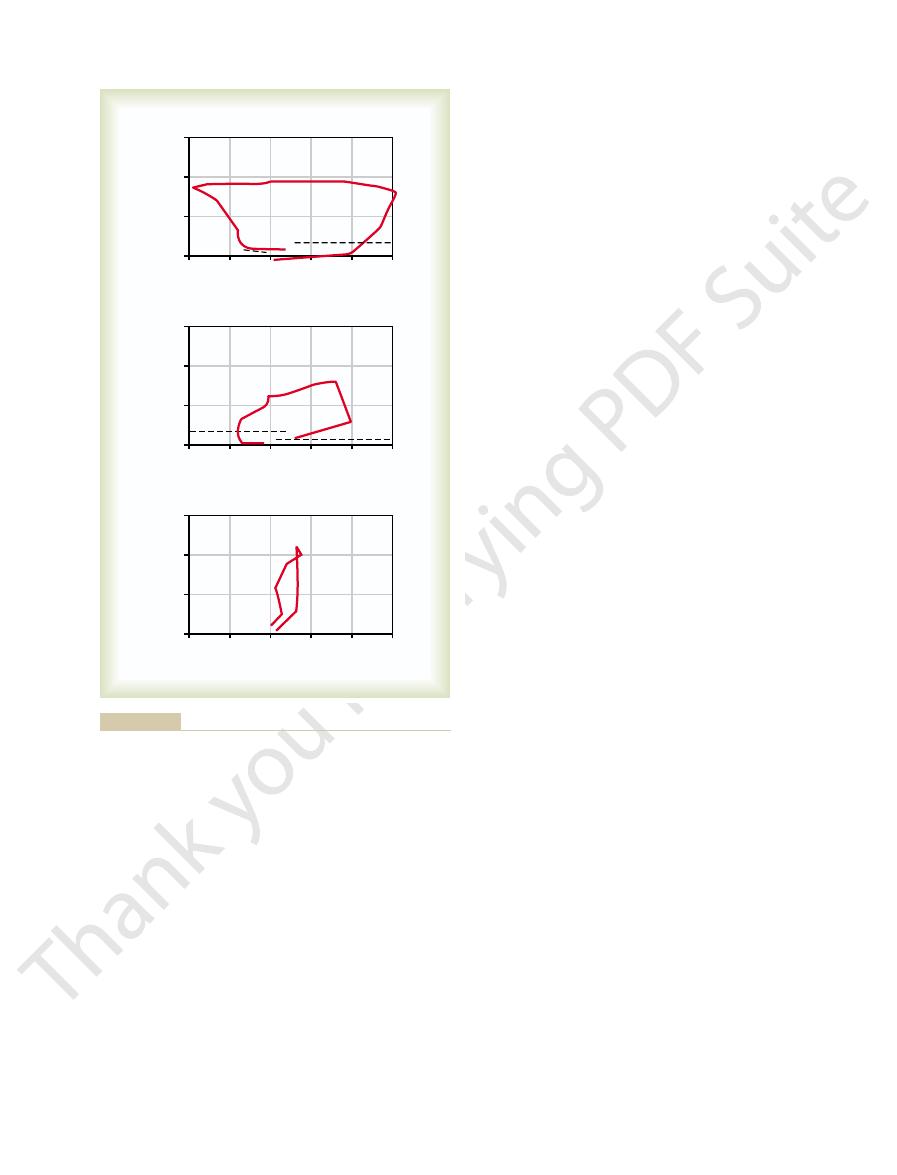
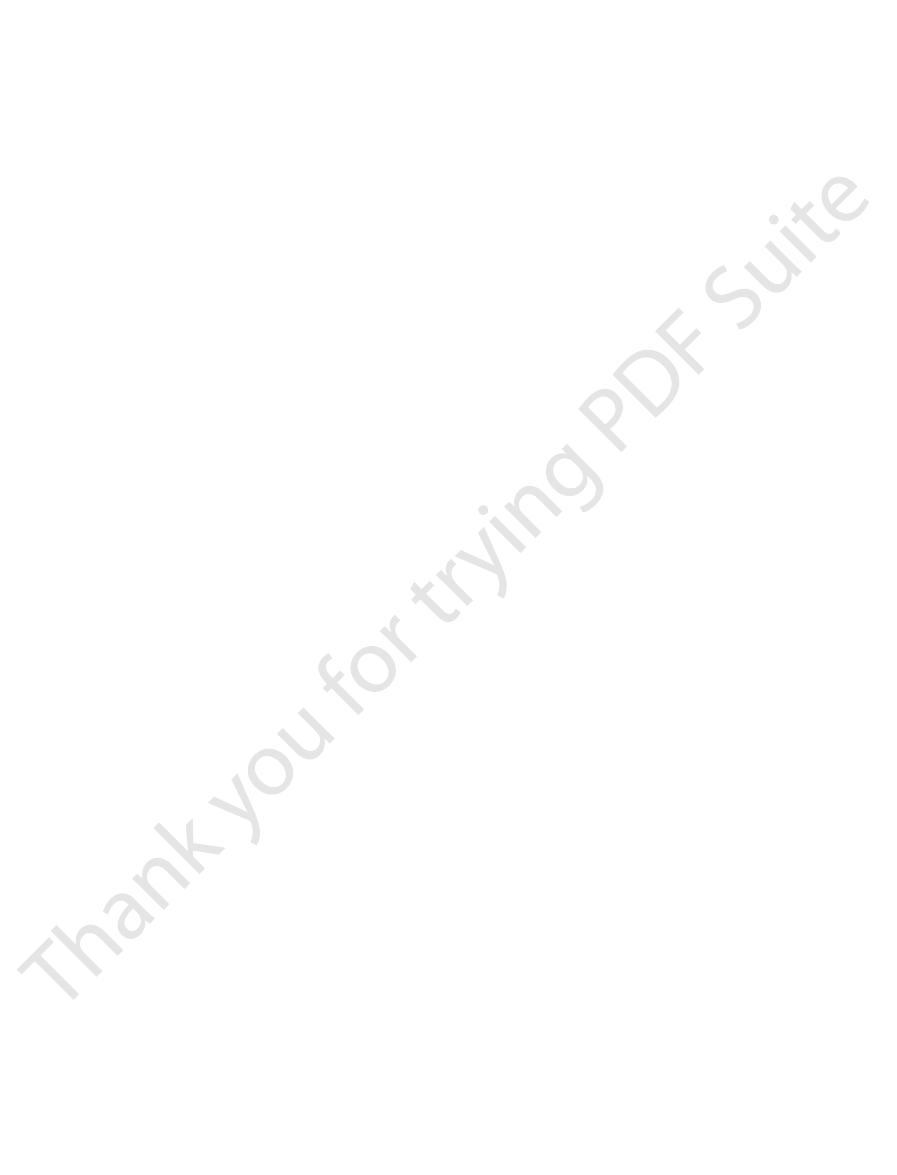
minutes after birth, as shown by the third compliance
less negative and positive pressures required. Breathing
Note that the second breath is much easier, with far
fluid in the bronchioles.
40 centimeters of water, is
itive pressure, about
enters the lungs. To deflate the lungs, considerable pos-
60 centimeters of water, about 40 milliliters of air
30 mm Hg). Then, as the negative pressure increases
moving to the right. The curve shows that the volume of
beginning at the zero pressure point
breath after birth. Observe, first, the lower part of
sure-volume curve (“compliance” curve) for the first
the onset of breathing. At the top is shown the pres-
Figure 83–3 shows the tremendous negative
space.
much as 60 mm Hg negative pressure in the intrapleural
are extremely powerful, usually capable of creating as
Fortunately, the first inspirations of the normal neonate
effected with relatively weak respiratory movements.
once the alveoli do open, further respiration can be
tension and to open the alveoli for the first time. But
25 mm Hg of negative inspiratory pressure in the lungs
tension of the viscid fluid that fills them. More than
At birth, the walls of the
affecting many of the motor functions of the body.
colliculi, and in other brain stem areas, thus permanently
lesions develop mainly in the thalamus, in the inferior
delayed more than 8 to 10 minutes. Indeed, actual
failure to breathe after birth. Permanent and very
Degree of Hypoxia That an Infant Can Tolerate.
the placenta; or (4) excessive anesthesia of the mother,
the uterus, which can cut off the mother’s blood flow to
separation of the placenta; (3) excessive contraction of
(1) compression of the umbilical cord; (2) premature
serious depression of the respiratory center.
tant, prolonged fetal hypoxia during delivery can cause
tory center. Second, and probably much more impor-
result from two possible effects: First, in a few infants,
breathe or sometimes do not breathe at all. This can
importance of using as little anesthesia as feasible. Also,
delayed for several minutes, thus demonstrating the
the fetus as well, the onset of respiration is likely to be
during delivery, which at least partially anesthetizes
progressively more hypoxic and hypercapnic, which
does not breathe immediately, the body becomes
originate in the suddenly cooled skin. In an infant who
birth process, but also from (2) sensory impulses that
sudden exposure to the exterior world, probably result-
minute after birth. The promptness with which the fetus
mother who has not been depressed by anesthetics, the
infant is to begin breathing.
fore, loss of this means of metabolic support. One of the
the placental connection with the mother and, there-
The most obvious effect of birth on the baby is loss of
Onset of Breathing
the mother is helpful in preventing fetal hemorrhage,
newborn infant. Therefore, prenatal storage in the fetal
colon, the neonate has no adequate source of vitamin K
vitamin K is formed by bacterial action in the mother’s
in the fetus as well as in the mother. Because most
mother, Factor VII and prothrombin become deficient
ulation factors. When vitamin K is insufficient in the
Factor VII, prothrombin, and several other blood coag-
Vitamin K is used by the fetal liver for formation of
pregnancy.
the early embryo. In its absence in laboratory animals,
are not clear, is necessary for normal development of
Vitamin E, although the mechanisms of its functions
body fluids, large quantities of the vitamin will be stored
nal tract. If the mother has plenty of this vitamin in her
fetus, but even more important, the mother needs it for
Vitamin D is needed for normal bone growth in the
fibers of connective tissue.
intercellular substances, especially the bone matrix and
Vitamin C is necessary for appropriate formation of
nervous tissue, as well as for overall growth of the fetus.
The B vitamins, especially vitamin B
mentioned, however.
71. Special functions of several vitamins should be
same in the fetus as in the adult, as discussed in Chapter
far greater extent. In general, the vitamins function the
The fetus needs vitamins
in the liver. This iron can then be used for several
to form the very early red blood cells. About one third
1044
Unit XIV
Endocrinology and Reproduction
of the iron in a fully developed fetus is normally stored
months after birth by the neonate for formation of addi-
tional hemoglobin.
Utilization and Storage of Vitamins.
equally as much as the adult and in some instances to a
12
and folic acid,
are necessary for formation of red blood cells and
adequate absorption of calcium from her gastrointesti-
by the fetal liver to be used by the neonate for several
months after birth.
spontaneous abortion usually occurs at an early stage of
for the first week or so of life after birth until normal
colonic bacterial flora become established in the
liver of at least small amounts of vitamin K derived from
particularly hemorrhage in the brain when the head is
traumatized by squeezing through the birth canal.
Adjustments of the Infant
to Extrauterine Life
most important immediate adjustments required of the
Cause of Breathing at Birth.
After normal delivery from a
child ordinarily begins to breathe within seconds and
has a normal respiratory rhythm within less than 1
begins to breathe indicates that breathing is initiated by
ing from (1) a slightly asphyxiated state incident to the
provides additional stimulus to the respiratory center
and usually causes breathing within an additional
minute after birth.
Delayed or Abnormal Breathing at Birth—Danger of Hypoxia.
If
the mother has been depressed by a general anesthetic
many infants who have had head trauma during deliv-
ery or who undergo prolonged delivery are slow to
intracranial hemorrhage or brain contusion causes a
concussion syndrome with a greatly depressed respira-
Hypoxia frequently occurs during delivery because of
which depresses oxygenation even of her blood.
In an adult,
failure to breathe for only 4 minutes often causes death,
but a neonate often survives as long as 10 minutes of
serious brain impairment often ensues if breathing is
Expansion of the Lungs at Birth.
alveoli are at first collapsed because of the surface
is usually required to oppose the effects of this surface
intrapleural pressures required to open the lungs at
the curve
and
air in the lungs remains almost exactly zero until the
negative pressure has reached
-40 centimeters water
(
-
to
-
+
required because of viscous resistance offered by the
does not become completely normal until about 40
The basic changes
the lungs.
diately after birth, virtually all the blood flows through
12 per cent of the blood flows through the lungs; imme-
tissues of the fetus. Furthermore, during fetal life, only
centa, leaving only 45 per cent to pass through all the
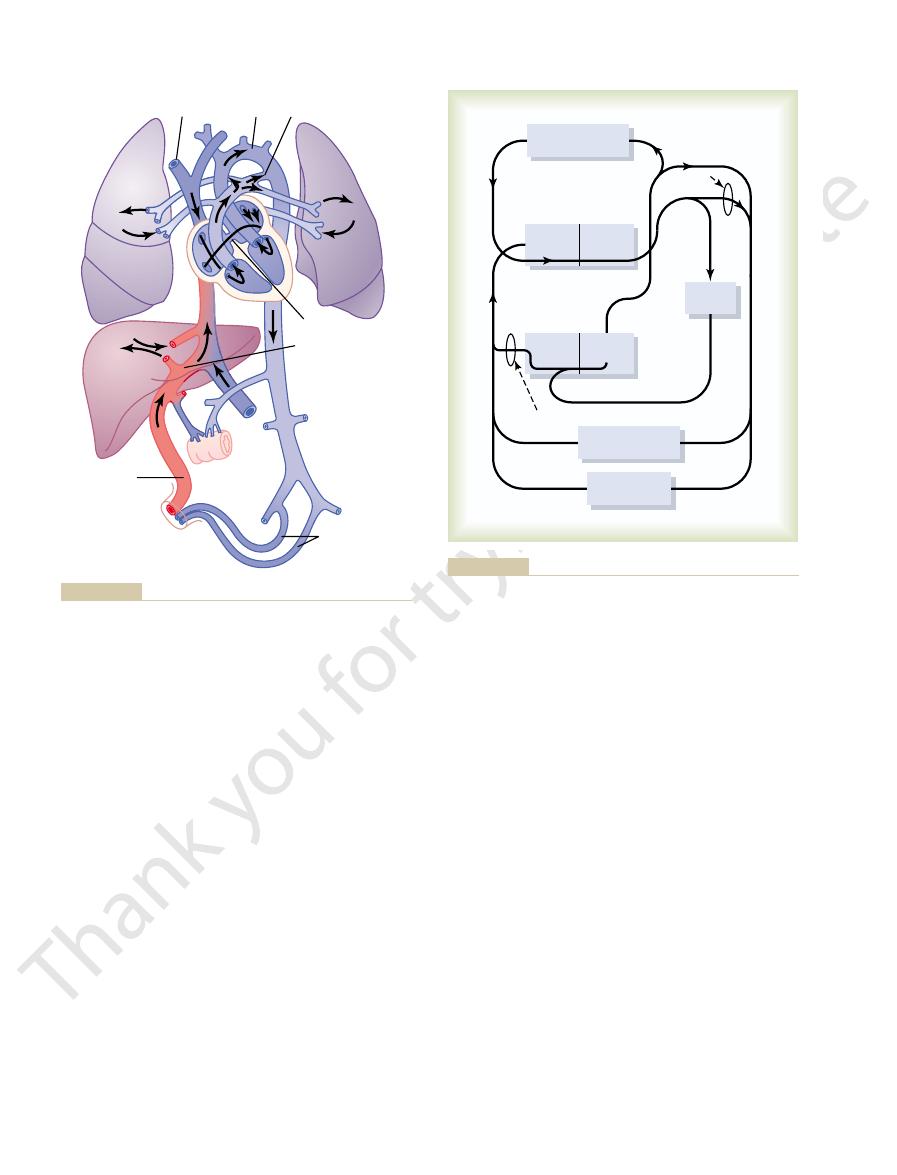
ferent vascular circuits of the fetus. This figure shows
Figure 83–5 gives the relative percentages of the total
umbilical arteries into the placenta, where the deoxy-
into the descending aorta, then through the two
deoxygenated blood from the head region of the fetus,
cuspid valve into the right ventricle. This blood is mainly
The blood entering the right atrium from the supe-
into the arteries of the head and forelimbs.
right side, and is pumped by the left ventricle mainly
enters mainly the left side of the heart, rather than the
Thus, the well-oxygenated blood from the placenta
foramen ovale
, mainly bypassing the liver. Then
First, as shown in Figure 83–4, blood returning from
differently from that of the newborn baby.
placenta. Therefore, special anatomical arrangements
through either the lungs or the liver. However, the fetal
because the liver is only partially functional, it is not
Specific Anatomical Structure of the Fetal Circulation.
these readjustments, we must first consider the anatom-
to this point has had very little blood flow. To describe
and more blood flow through the baby’s liver, which up
quate blood flow through the lungs. Also, circulatory
pulmonary edema. The role of surfactant in preventing
a collapse tendency of the alveoli and development of
bility to secrete sufficient surfactant, which causes both
months of gestation. Therefore, many premature babies
ing the alveoli to open easily during inspiration. The sur-
the surface tension of the alveolar fluid, therefore allow-
, a sub-
hyaline membrane.
lar epithelial cells. This condition is called
the alveoli. The fluid also contains desquamated alveo-
contain large quantities of proteinaceous fluid, almost
next day or so. The alveoli of these infants at death
the first several days after birth, and some die within the
mature infants and infants born of diabetic mothers,
A small number of infants, especially pre-
Respiratory Distress Syndrome Caused When Surfactant Secretion
for the normal adult, as shown in Chapter 38.
curve, the shape of which compares favorably with that
Fetal and Neonatal Physiology
Chapter 83
1045
Is Deficient.
develop severe respiratory distress in the early hours to
as if pure plasma had leaked out of the capillaries into
hyaline mem-
brane disease because microscopic slides of the lung
show the material filling the alveoli to look like a
One of the most characteristic findings in respiratory
distress syndrome is failure of the respiratory epithe-
lium to secrete adequate quantities of surfactant
stance normally secreted into the alveoli that decreases
factant-secreting cells (type II alveolar epithelial cells)
do not begin to secrete surfactant until the last 1 to 3
and a few full-term babies are born without the capa-
these effects is discussed in Chapter 37.
Circulatory Readjustments at Birth
Equally as essential as the onset of breathing at birth
are immediate circulatory adjustments that allow ade-
adjustments during the first few hours of life cause more
ical structure of the fetal circulation.
Because
the lungs are mainly nonfunctional during fetal life and
necessary for the fetal heart to pump much blood
heart must pump large quantities of blood through the
cause the fetal circulatory system to operate much
the placenta through the umbilical vein passes through
the ductus venosus
most of the blood entering the right atrium from the
inferior vena cava is directed in a straight pathway
across the posterior aspect of the right atrium and
through the
directly into the left atrium.
rior vena cava is directed downward through the tri-
and it is pumped by the right ventricle into the pul-
monary artery and then mainly through the ductus arte-
riosus
genated blood becomes oxygenated.
blood pumped by the heart that pass through the dif-
that 55 per cent of all the blood goes through the pla-
Changes in the Fetal Circulation at Birth.
in the fetal circulation at birth are discussed in
20
0
20
0
20
0
+
40
+
-
60
-
20
-
40
Pressure
Second Breath
60
40
20
0
Volume (ml)
+
40
+
-
60
-
20
-
40
Pressure
First Breath
60
40
20
0
Volume (ml)
+
40
+
-
60
-
20
-
40
Pressure
40 Minutes
60
40
20
0
Volume (ml)
reserved.)
after birth. (Redrawn from Smith CA: The first breath. Sci Am
opment of a nearly normal compliance curve within 40 minutes
required for breathing during the first two breaths of life and devel-
neonate immediately after birth, showing the extreme forces
Pressure-volume curves of the lungs (“compliance” curves) of a
Figure 83–3
209:32, 1963, © 1963 by Scientific American, Inc. All rights
of the ductus arteriosus. Then, during the next 1 to
to stop all blood flow. This is called
within 1 to 8 days, the constriction is usually sufficient
wall of the ductus arteriosus constricts markedly, and
in fetal life. However, after only a few hours, the muscle
ductus arteriosus, rather than in the other direction as
consequence, after birth, blood begins to flow backward
reduces the pulmonary arterial pressure.
reasons. First, the increased systemic resistance
The ductus arteriosus also closes, but for different
than the right atrial pressure, and the backpressure
throughout life normally remains 2 to 4 mm Hg greater
manent closure does not occur, the left atrial pressure
years and forms a permanent closure. But even if per-
In two thirds of all people, the valve becomes adher-
the foramen ovale.
this opening, thereby preventing further flow through
Consequently, the small valve that lies over the foramen
than in the other direction, as occurred during fetal life.
that is, from the left atrium into the right atrium, rather
low right atrial pressure
The
right atrial pressure.
through the lungs as much as fivefold, which
tion of the lungs eliminates the hypoxia. All these
blood vessels, but vasodilation takes place when aera-
severalfold. Also, in fetal life, the hypoxia of the lungs
diately on expansion, these vessels are no longer
pressed because of the small volume of the lungs. Imme-
unexpanded fetal lungs, the blood vessels are com-
as a result of expansion of the lungs. In the
Second, the
resistance at birth. This increases the aortic pressure as
The primary changes in the circulation at birth are, first,
Primary Changes in Pulmonary and Systemic Vascular
are the following.
throughout life in a few persons. Briefly, these changes
1046
Unit XIV
Endocrinology and Reproduction
Chapter 23 in relation to congenital anomalies of the
ductus arteriosus and foramen ovale that persist
Resistances at Birth
loss of the tremendous blood flow through the placenta,
which approximately doubles the systemic vascular
well as the pressures in the left ventricle and left atrium.
pulmonary vascular resistance greatly
decreases
compressed and the resistance to blood flow decreases
causes considerable tonic vasoconstriction of the lung
changes together reduce the resistance to blood flow
reduces the
pulmonary arterial pressure, right ventricular pressure,
and
Closure of the Foramen Ovale
and the high left atrial pres-
sure that occur secondarily to the changes in pulmonary
and systemic resistances at birth cause blood now to
attempt to flow backward through the foramen ovale;
ovale on the left side of the atrial septum closes over
ent over the foramen ovale within a few months to a few
keeps the valve closed.
Closure of the Ductus Arteriosus
elevates
the aortic pressure while the decreased pulmonary
resistance
As a
from the aorta into the pulmonary artery through the
functional closure
Aorta
Ductus arteriosus
Ductus arteriosus
Umbilical
arteries
Umbilical
vein
Foramen ovale
Lung
Lung
Gut
Liver
Superior
vena cava
Embryology. 7th ed. Philadelphia: WB Saunders Co, 1974.)
Developmental Anatomy: A Textbook and Laboratory Manual of
Organization of the fetal circulation. (Modified from Arey LB:
Figure 83–4
Forequarters
Forequarters
Hindquarters
Hindquarters
Placenta
Placenta
Right
atrium
Right
atrium
Right
ventricle
Right
ventricle
Ductus
arteriosus
Ductus
arteriosus
Foramen
ovale
Foramen
ovale
Left
atrium
Left
atrium
Left
ventricle
Left
ventricle
Lungs
Lungs
58
58
46
46
27
27
15
15
15
15
43
43
42
42
30
30
73
73
73
73
12
12
18
18
55
55
heart flowing through each particular area.
represent the percentage of the total output from both sides of the
tion of blood flow to the different vascular areas. The numerals
Diagram of the fetal circulatory system, showing relative distribu-
Figure 83–5
that time on, increasing activity by the baby provides
per cubic millimeter by about 6 to 8 weeks of age. From
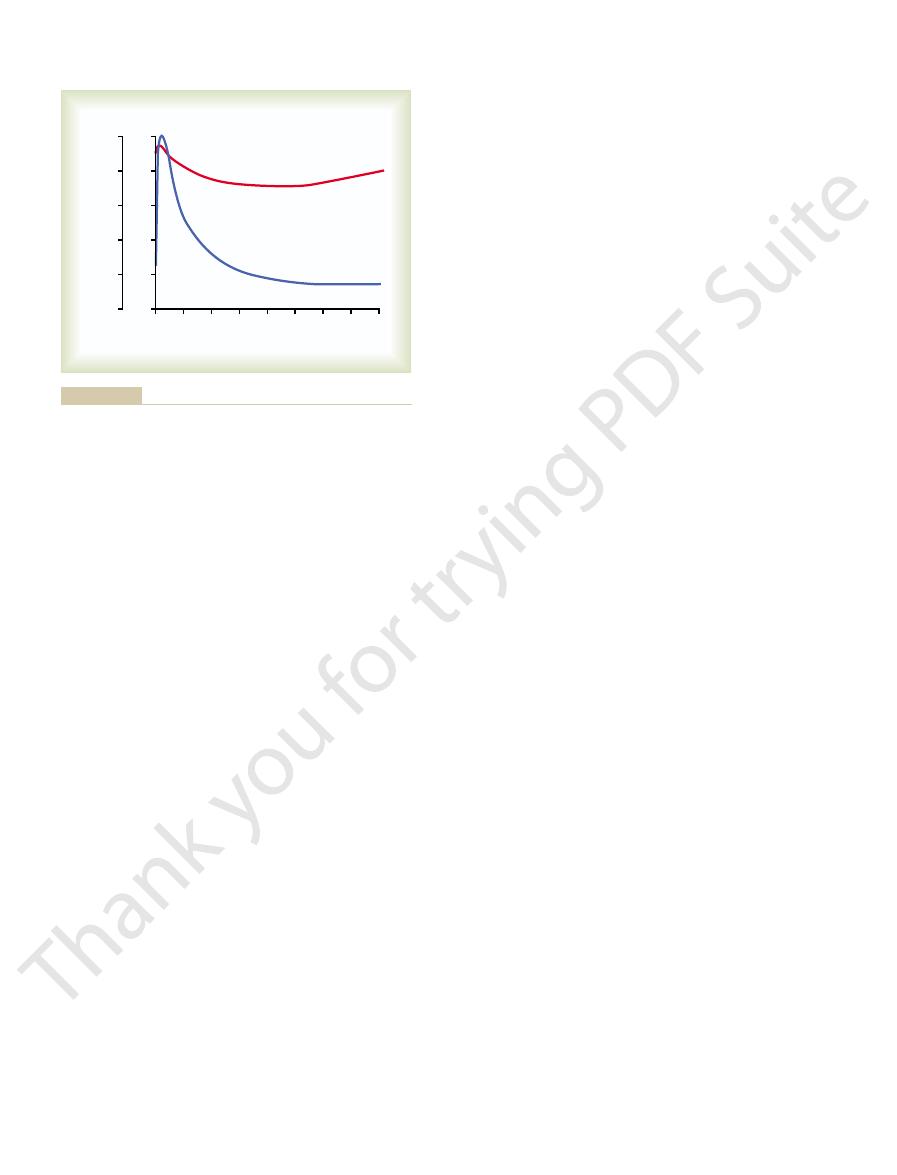
red cell production. Thus, as shown in Figure 83–6, the
first few weeks of life, presumably because the hypoxic
shown in Figure 83–6. Subsequent to this, however, few
count of about 4.75 million per cubic millimeter, as
during the first few hours of life, giving a red blood cell
If blood is stripped from the cord into the infant, the red
neonate averages about 4 million per cubic millimeter.
The red blood cell count in the
adult pressure of 115/70 is attained at adolescence.
next several months to about 90/60. Then there is a
50 mm Hg diastolic; this increases slowly during the
day after birth averages about 70 mm Hg systolic and
The arterial pressure during the first
weight as in the adult. Occasionally a child is born with
metabolism, is about twice as much in relation to body
averages 500 ml/min, which, like respiration and body
The cardiac output of the neonate
tory distress, but the extra red blood cells are often very
liliters. Some pediatricians believe that this extra blood
is lost into the neonate’s tissue spaces from this blood,
375 milliliters. Then, during the ensuing few hours, fluid
milliliters of blood enters the infant, to make a total of
blood out of its vessels into the baby, an additional 75
ately after birth averages about 300 milliliters, but if the
The blood volume of a neonate immedi-
Blood Volume.
blood gas variations.
decreases in the newborn baby’s blood gas concentra-
difference causes excessive cyclical increases and
This
tional residual capacity of the infant’s lungs is only one
volume of 640 ml/min, which is about twice as great in
ages 16 milliliters. This gives a total minute respiratory
breaths per minute, and tidal air with each breath aver-
The normal rate of respiration in a neonate is about 40
adjusted to the new way of life.
systems. This results partly from immature development
Special Functional Problems
body solids.
much as 20 per cent within the first 2 to 3 days of life.
requires several days to develop. Ordinarily, the infant’s
times that of an adult, and the mother’s milk supply
the infant’s rate of body fluid turnover averages seven
mother’s milk can be provided 2 to 3 days later.
than one half the normal value. Fortunately, however,
the first day to as low as 30 to 40 mg/dl of plasma, less
the infant’s blood glucose concentration frequently falls
which prevents significant gluconeogenesis. Therefore,
the infant’s needs for only a few hours. The liver of the
the amount of glucose stored in the infant’s body in the
glucose obtained from the mother’s blood. After birth,
Before birth, the fetus derives almost all its energy from
know almost nothing about what causes the closure.
Although the ductus venosus rarely fails to close, we
force portal venous blood flow through the liver sinuses.
rises from near 0 to 6 to 10 mm Hg, which is enough to
of flow. As a consequence, the portal venous pressure
However, within 1 to 3 hours the muscle wall of the
amount passing through the channels of the liver.
still flows through the ductus venosus, with only a small
umbilical vein ceases, but most of the portal blood
Immediately after birth, blood flow through the
liver.
below the heart but above the liver, thus bypassing the
umbilical vein, and these together pass by way of the
from the fetus’s abdomen joins the blood from the
In fetal life, the portal blood
Closure of the Ductus Venosus
prostaglandins, often leads to closure.
, which blocks synthesis of
prostaglandins in the ductus wall. In fact, administration
quences of which are discussed in Chapter 23. The
, the conse-
close, resulting in a
In one of several thousand infants, the ductus fails to
within a few hours after birth. Furthermore, many
15 to 20 mm Hg, but it increases to about 100 mm Hg
ductus. In fetal life the P
The cause of ductus arteriosus closure relates to the
4 months, the ductus arteriosus ordinarily becomes
Fetal and Neonatal Physiology
Chapter 83
1047
anatomically occluded by growth of fibrous tissue into
its lumen.
increased oxygenation of the blood flowing through the
O
2
of the ductus blood is only
experiments have shown that the degree of contraction
of the smooth muscle in the ductus wall is highly related
to this availability of oxygen.
patent ductus arteriosus
failure of closure has been postulated to result from
excessive ductus dilation caused by vasodilating
of the drug indomethacin
ductus venosus directly into the vena cava immediately
ductus venosus contracts strongly and closes this avenue
Nutrition of the Neonate
form of liver and muscle glycogen is sufficient to supply
neonate is still far from functionally adequate at birth,
appropriate mechanisms are available for the infant to
use its stored fats and proteins for metabolism until
Special problems are also frequently associated with
getting an adequate fluid supply to the neonate because
weight decreases 5 to 10 per cent and sometimes as
Most of this weight loss is loss of fluid rather than of
in the Neonate
An important characteristic of the neonate is instability
of the various hormonal and neurogenic control
of the different organs of the body and partly from the
fact that the control systems simply have not become
Respiratory System
relation to the body weight as that of an adult. The func-
half that of an adult in relation to body weight.
tions if the respiratory rate becomes slowed because it
is the residual air in the lungs that smooths out the
Circulation
infant is left attached to the placenta for a few minutes
after birth or if the umbilical cord is stripped to force
which increases the hematocrit but returns the blood
volume once again to the normal value of about 300 mil-
volume caused by stripping the umbilical cord can lead
to mild pulmonary edema with some degree of respira-
valuable to the infant.
Cardiac Output.
an especially low cardiac output caused by hemorrhage
of much of its blood volume from the placenta at birth.
Arterial Pressure.
much slower rise during the subsequent years until the
Blood Characteristics.
blood cell count rises an additional 0.5 to 0.75 million
new red blood cells are formed in the infant during the
stimulus of fetal life is no longer present to stimulate
average red blood cell count falls to less than 4 million
the appropriate stimulus for returning the red blood cell
storing proteins. Indeed, with an adequate diet, as much
The neonate is especially capable of synthesizing and
in the blood is unstable and low.
at least the first week of life, the glucose concentration
Third, because the liver functions imperfectly during
milk, is frequently inadequately absorbed.
sequently, milk with a high fat content, such as cow’s
tract is somewhat less than that in the older child. Con-
Second, absorption of fats from the gastrointestinal
is deficient, so that the neonate uses starches less ade-
First, secretion of pancreatic amylase in the neonate
older child, with the following three exceptions.
In general, the ability of the neonate to digest, absorb,
Metabolism of Energy Foods;
Digestion, Absorption, and
4. The liver of the neonate usually also forms too
until sufficient feeding can occur.
mg/dl (about 40 per cent of normal), and the infant
particularly deficient. As a result, the blood glucose
3. The gluconeogenesis function of the liver is
plasma proteins, so that the plasma protein
2. The liver of the neonate is deficient in forming
life.
1. The liver of the neonate conjugates bilirubin with
neonate may be quite deficient, as evidenced by the
During the first few days of life, liver function in the
tion, and, more rarely, overhydration.
important problems of infancy are acidosis, dehydra-
of acid, one can readily understand that among the most
sidering the immaturity of the kidneys, together with the
instead of the adult three to four times. Therefore, con-
instance, the kidneys of the neonate can concentrate
until the end of about the first month of life. For
which gives a tendency toward acidosis in the infant.
great in relation to body mass as in the adult, which
The rate of metabolism in the infant is also twice as
cause rapidly developing abnormalities.
weight as in the adult, which means that even a slight
The rate of fluid intake and fluid excretion in the
and Renal Function
Fluid Balance, Acid-Base Balance,
seriously in 1 of every 50 to 100 neonates.
cal therapeutics, this condition occurred either mildly or
quate red cells. Before the advent of modern obstetri-
releasing extreme quantities of bilirubin into the fetus’s
blood cells, and her antibodies destroy fetal red cells,
against the Rh-positive factor (a protein) in the fetus’s
Rh negative. The mother then becomes immunized
positive red cells from the father, while the mother is
erythroblastotic baby
mother. Briefly, the
erythroblastosis fetalis,
However, by far the most important abnormal cause
a week or two.
infant’s skin and especially of the sclerae of its eyes for
is shown in Figure 83–6, and it
liver becomes functional. This effect, called
1 mg/dl to an average of 5 mg/dl during the first 3 days
excretion into the bile. Consequently, the plasma biliru-
neonate’s own liver, which for the first week or so of life
mother, but immediately after birth, the only means
neonate is about 45,000 per cubic millimeter, which is
ately after birth, the white blood cell count of the
count to normal within another 2 to 3 months. Immedi-
1048
Unit XIV
Endocrinology and Reproduction
about five times as great as that of the normal adult.
Neonatal Jaundice and Erythroblastosis Fetalis.
Biliru-
bin formed in the fetus can cross the placenta into
the mother and be excreted through the liver of the
for ridding the neonate of bilirubin is through the
functions poorly and is incapable of conjugating signi-
ficant quantities of bilirubin with glucuronic acid for
bin concentration rises from a normal value of less than
of life and then gradually falls back to normal as the
physiologic
hyperbilirubinemia,
is associated with mild jaundice (yellowness) of the
of serious neonatal jaundice is
which is discussed in detail in Chapter 32 in relation
to Rh factor incompatibility between the fetus and
inherits Rh-
plasma and often causing fetal death for lack of ade-
newborn infant is seven times as great in relation to
percentage alteration of fluid intake or fluid output can
means that twice as much acid is normally formed,
Functional development of the kidneys is not complete
urine to only 1.5 times the osmolality of the plasma
marked fluid turnover in the infant and rapid formation
Liver Function
following effects:
glucuronic acid poorly and therefore excretes
bilirubin only slightly during the first few days of
concentration falls during the first weeks of life to
15 to 20 per cent less than that for older children.
Occasionally the protein concentration falls so low
that the infant develops hypoproteinemic edema.
level of the unfed neonate falls to about 30 to 40
must depend mainly on its stored fats for energy
little of the blood factors needed for normal blood
coagulation.
and Nutrition
and metabolize foods is no different from that of the
quately than do older children.
0
2
4
6
8
10
12
14
16
0
1
2
3
4
5
Age in weeks
Bilirubin
Red blood count
Serum bilirubin (mg/dl)
0
1
2
3
4
5
Red blood cell count (millions/mm
3
)
Changes in the red blood cell count and in serum bilirubin con-
Figure 83–6
centration during the first 16 weeks of life, showing physiologic
anemia at 6 to 12 weeks of life and physiologic hyperbilirubine-
mia during the first 2 weeks of life.
1. If a pregnant mother bearing a female child is
special instances in which the endocrinology of infancy
immediate endocrine abnormalities. However, there are
developed at birth, and the infant seldom exhibits any
Ordinarily, the endocrine system of the infant is highly
appear. This relation of immunity to allergy is discussed
nity develop, these allergic manifestations usually dis-
trointestinal abnormalities, and even anaphylaxis. As
can develop, often resulting in serious eczema, gas-
antibodies first begin to form, extreme allergic states
Several months later, however, when the infant’s own
The newborn infant is seldom subject to allergy.
Allergy.
life.
therefore, for full safety, the infant requires immuniza-
Conversely, the inherited antibodies against whooping
diseases before 6 months is usually unnecessary.
and polio. Therefore, immunization against these
hood infectious diseases, including diphtheria, measles,
birth, the antibodies inherited from the mother protect
months.
antibodies, and the gamma globulin concentration
after, the baby’s own immunity system begins to form
level, with a corresponding decrease in immunity.There-
bodies, have decreased to less than one half the original
the baby’s gamma globulins, which contain the anti-
own to a significant extent. By the end of the first month,
However, the neonate does not form antibodies of its
mother’s blood through the placenta into the fetus.
The neonate inherits much immunity from the mother
acid are often prescribed by the third week of life.
this reason, orange juice or other sources of ascorbic
which has only one fourth as much as human milk. For
poor supplies of ascorbic acid, especially cow’s milk,
lular structures of the infant. Furthermore, milk has
proper formation of cartilage, bone, and other intercel-
quantities in the fetal tissues; yet it is required for
third month of life.
sonably large quantities of iron, or the administration of
feeding of the infant with egg yolk, which contains rea-
about 3 months of life. To prevent this possibility, early
diet, severe anemia is likely to occur in the infant after
birth. But if the mother has had insufficient iron in her
diet, the liver of the infant usually has stored enough
even less effectively than those of normal infants.
weeks. This is particularly true in premature babies
absence of vitamin D. Therefore, the vitamin D–
adequately by the usual diet of milk. Yet absorption of
throughout infancy is needed. This is ordinarily supplied
bones at birth, so that a ready supply of calcium
The neonate is in a stage of rapid ossification of its
are provided in the diet. However, three specific prob-
more, function of the gastrointestinal system is usually
vided the mother has had an adequate diet. Further-
neonate is usually in complete nutritional balance, pro-
At birth, a
Nutritional Needs During the Early Weeks of Life.
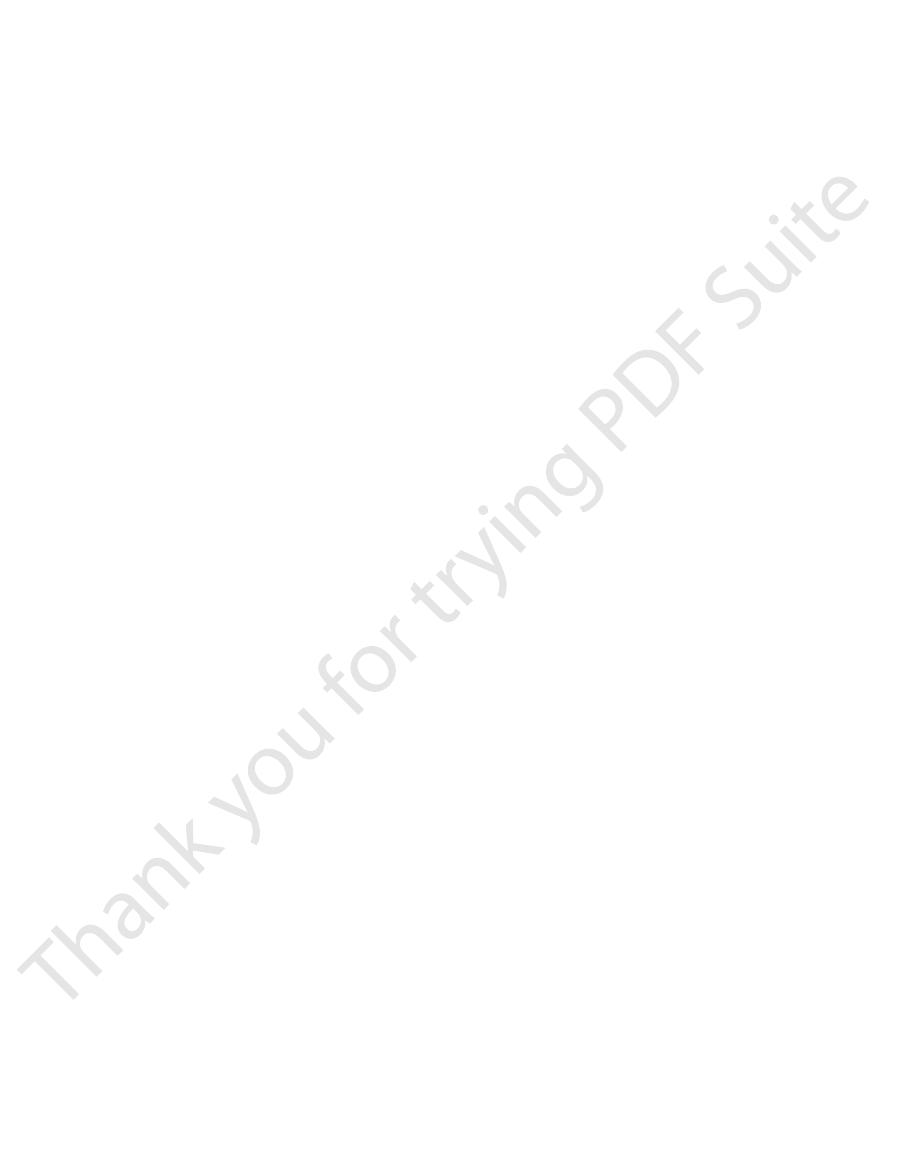
temperature, which are also shown in Figure 83–7.
the early days of life, allowing marked deviations in
returns to normal in 7 to 10 hours. Still, the body tem-
premature infants, falls easily. Figure 83–7 shows that
the body temperature of the neonate, particularly of
body mass, heat is readily lost from the body. As a result,
about twice that of the adult, which accounts also for
The normal meta-
Metabolic Rate and Body Temperature.
centage than in adults.
formation of body proteins. This is a much higher per-
Fetal and Neonatal Physiology
Chapter 83
1049
as 90 per cent of the ingested amino acids are used for
bolic rate of the neonate in relation to body weight is
the twice as great cardiac output and twice as great
minute respiratory volume in relation to body weight in
the infant.
Because the body surface area is large in relation to
the body temperature of even a normal infant often falls
several degrees during the first few hours after birth but
perature regulatory mechanisms remain poor during
more than adequate to digest and assimilate all the
nutritional needs of the infant if appropriate nutrients
lems do occur in the early nutrition of the infant.
Need for Calcium and Vitamin D
calcium by the gastrointestinal tract is poor in the
deficient infant can develop severe rickets in only a few
because their gastrointestinal tracts absorb calcium
Necessity for Iron in the Diet
If the mother has had adequate amounts of iron in her
iron to keep forming blood cells for 4 to 6 months after
iron in some other form is desirable by the second or
Vitamin C Deficiency in Infants
Ascorbic acid (vitamin C) is not stored in significant
Immunity
because many protein antibodies diffuse from the
returns essentially to normal by the age of 12 to 20
Despite the decrease in gamma globulins soon after
the infant for about 6 months against most major child-
cough are normally insufficient to protect the neonate;
tion against this disease within the first month or so of
the child grows older and still higher degrees of immu-
in Chapter 34.
Endocrine Problems
is important:
treated with an androgenic hormone or if an
Hours after birth
Days after birth
2
20
0 2 4 6 8 10 12
4 6 8 10 12 14 16 18
93
99
98
97
96
95
94
Body temperature (
°
F)
Birth
and instability of body temperature during the first few days of life.
Fall in body temperature of the neonate immediately after birth,
Figure 83–7
limits of 20 to more than 100 mg/dl, depending princi-
brings on hypocalcemic tetany. Also, the blood glucose
because of immature liver development, often leading
Likewise, the blood protein concentration is usually low
when the rate of food intake varies from time to time.
acid-base balance can vary tremendously, particularly
homeostatic mechanisms of the body. For instance, the
Control Systems in the
Instability of the Homeostatic
phoid system, which often leads to serious infection.
which allows rapid development of anemia; and (4)
of the blood-forming mechanism of the bone marrow,
as to serious fluid balance abnormalities; (3) immaturity
body of acids, thereby predisposing to acidosis as well
of coagulation factors; (2) immaturity of the kidneys,
often a bleeding tendency as a result of poor formation
premature infant includes (1) immaturity of the liver,
vitamin D intake.
before the difficulty is recognized. For this reason,
calcium and, therefore, can develop severe rickets
mature infant must have a low-fat diet. Furthermore,
inadequate. The absorption of fat is so poor that the pre-
If the infant is more than 2 months premature, the
with periodic breathing of the Cheyne-Stokes type.
common cause of death. Also, the low functional resid-
As a consequence,
infant. Also, surfactant secretion is depressed or absent.
be underdeveloped in the premature infant. The vital
The respiratory system is especially likely to
in the premature infant, but some require particular
Immature Development of the
homeostatic control systems. Because of these effects, a
under the following two headings: (1) immaturity of
exacerbated in prematurity. They can be categorized
of Prematurity
Special Problems
This causes the condition called
6. In a fetus lacking thyroid hormone secretion, the
thyrotropin during gestation, and the child might be
woman had had her thyroid gland removed, her
thyroid gland. Conversely, if before pregnancy a
treated with excess thyroid hormone, the infant is
5. If a pregnant woman has hyperthyroidism or is
, which can
adrenal cortices, often resulting from
4. Occasionally a child is born with hypofunctional
earlier in the chapter.
, described
mortality rate. Two thirds of the infants who die
fetuses that do come to term, there is still a high
rate of intrauterine mortality, and among those
neonate are often impaired. Also, there is a high
mother, and growth and tissue maturation of the
(caused by lack of insulin secretion), fetal growth
increased fetal growth. However, most of the
weight. Increased supply of glucose and other
increases in plasma insulin concentration. The high
cause of large babies. Type II diabetes in the
only rarely develops.
neonate, unlike in the adult, insulin shock or coma
shortly after birth. Fortunately, however, in the
concentration may fall to lower than 20 mg/dl
As a consequence, the infant’s blood glucose
of the islets of Langerhans in the pancreas.
3. An infant born of an untreated diabetic mother will
develops.
then become inflamed, or infectious mastitis
during the first days of life. Sometimes the breasts
cause the neonate’s breasts to form milk
the mother’s glands during pregnancy occasionally
2. The sex hormones secreted by the placenta and by
masculinization of her sexual organs, thus resulting
androgenic tumor develops during pregnancy,
1050
Unit XIV
Endocrinology and Reproduction
the child will be born with a high degree of
in a type of hermaphroditism.
have considerable hypertrophy and hyperfunction
from this low level of blood glucose concentration
Maternal type II diabetes is the most common
mother is associated with resistance to the
metabolic effects of insulin and compensatory
levels of insulin are believed to stimulate fetal
growth factor and contribute to increased birth
nutrients to the fetus may also contribute to
increased fetal weight is due to increased body fat;
there is usually little increase in body length
although the size of some organs may be increased
(organomegaly).
In the mother with uncontrolled type I diabetes
may be stunted because of metabolic deficits in the
succumb to respiratory distress syndrome
agenesis of
the adrenal glands or exhaustion atrophy
occur when the adrenal glands have been vastly
overstimulated.
likely to be born with a temporarily hyposecreting
pituitary gland may secrete great quantities of
born with temporary hyperthyroidism.
bones grow poorly and there is mental retardation.
cretin dwarfism,
discussed in Chapter 76.
All the problems in neonatal life just noted are severely
certain organ systems and (2) instability of the different
premature baby seldom lives if it is born more than 3
months before term.
Premature Infant
Almost all the organ systems of the body are immature
attention if the life of the premature baby is to be saved.
Respiration.
capacity and the functional residual capacity of the
lungs are especially small in relation to the size of the
respiratory distress syndrome is a
ual capacity in the premature infant is often associated
Gastrointestinal Function.
Another major problem of the
premature infant is to ingest and absorb adequate food.
digestive and absorptive systems are almost always
the premature infant has unusual difficulty in absorbing
special attention must be paid to adequate calcium and
Function of Other Organs.
Immaturity of other organ
systems that frequently causes serious difficulties in the
which results in poor intermediary metabolism and
which are particularly deficient in their ability to rid the
depressed formation of gamma globulin by the lym-
Premature Infant
Immaturity of the different organ systems in the pre-
mature infant creates a high degree of instability in the
to hypoproteinemic edema. And inability of the infant
to regulate its calcium ion concentration frequently
concentration can vary between the extremely wide
the female.
because of much delayed uniting of the epiphyses, so
however, undergoes much more prolonged growth
age—mainly between ages 13 and 17 years. The male,
the male, which causes extra growth at a slightly later
ceases. This contrasts with the effect of testosterone in
14th to 16th year of life, so that growth in height then
the ages of 11 and 13 years, the female estrogens begin
exactly until the end of the first decade of life. Between
girls from the time of birth until the age of 20 years.
Figure 83–8 shows the changes in heights of boys and
tions of this book on metabolism and endocrinology.
for growth, which have been fully covered in the sec-
The major physiologic problems of the child beyond the
Growth and Development
breathed, but some child physiologists believe that com-
causes permanent blindness. For this reason, it is par-
This condition, known as
eye’s clear vitreous humor should be.
from the pupil to the retina. And still later, the vessels
growing all through the vitreous humor, blocking light
therapy is stopped, the blood vessels try to make up for
new blood vessels in the retina. Then when oxygen
The reason is that too much oxygen stops the growth of
especially in early prematurity, can lead to blindness.
that use of excess oxygen in treating premature infants,
treating prematurity. However, it has been discovered
tory distress, oxygen therapy has often been used in
in the Premature Infant
the incubator in treatment of prematurity.
of death, which explains the almost mandatory use of
the low 90°s or even in the 80°s F. Statistical studies
temperature, the infant’s temperature may stabilize in
approach that of its surroundings. At normal room
normal body temperature. Its temperature tends to
Instability of Body Temperature.
ment of the premature infant, that mortality is high.
pally on the regularity of feeding. It is no wonder, then,
Fetal and Neonatal Physiology
Chapter 83
1051
with these extreme variations in the internal environ-
One of the particular prob-
lems of the premature infant is inability to maintain
show that a body temperature maintained below 96°F
(35.5°C) is associated with a particularly high incidence
Danger of Blindness Caused
by Excess Oxygen Therapy
Because premature infants frequently develop respira-
lost time and burst forth with a great mass of vessels
are replaced with a mass of fibrous tissue where the
retrolental fibroplasia,
ticularly important to avoid treatment of premature
infants with high concentrations of respiratory oxygen.
Physiologic studies indicate that the premature infant is
usually safe with up to 40 per cent oxygen in the air
plete safety can be achieved only at normal oxygen con-
centration in the air that is breathed.
of the Child
neonatal period are related to special metabolic needs
Note especially that these parallel each other almost
to be formed and cause rapid growth in height but early
uniting of the epiphyses of the long bones at about the
that his final height is considerably greater than that of
Age in months
Age in years
20 24
4 8 12 16
8
12
16
0
20
4
20
70
60
50
40
30
Boys
Height (inches)
Girls
Average height of boys and girls from infancy to 20 years of age.
Figure 83–8
Vocalizes
Vocalizes
Walks with support
Walks with support
Walks alone
Walks alone
12
12
11
11
10
10
9
9
8
8
7
7
6
6
5
5
4
4
3
3
2
2
1
1
0
0
Age in months
Birth
Birth
Stands alone
Stands alone
Pulls up
Pulls up
Grasps
Grasps
Crawls
Crawls
Sits briefly
Sits briefly
Rolls over
Rolls over
Hand control
Hand control
Head control
Head control
Smiles
Smiles
Suckles
Suckles
Figure 83–9
Behavioral development of the infant during the first year of life.
Physiol 277:R1541, 1999.
reflex responses to hypotension during fetal life. Am J
Wood CE, Tong H: Central nervous system regulation of
congenital heart disease. Annu Rev Physiol 63:451, 2001.
Srivastava D: Genetic assembly of the heart: implications for
tions in the developing lung. Annu Rev Physiol 66:625,
Shannon JM, Hyatt BA: Epithelial-mesenchymal interac-
Am J Physiol 274:R879, 1998.
Ross MG, Nijland MJ: Development of ingestive behavior.
tion of lung liquid transport. Annu Rev Physiol 66:77,
Olver RE, Walters DV, M Wilson S: Developmental regula-
282:L341, 2002.
ration, and plasticity. Am J Physiol Lung Cell Mol Physiol
McMurtry IF: Pre- and postnatal lung development, matu-
emphasis on venous return. Hum Reprod Update 6:177,
Matias A, Montenegro N, Areias JC, Leite LP: Haemody-
62:289, 2000.
cardiac growth control pathways. Annu Rev Physiol
MacLellan WR, Schneider MD: Genetic dissection of
Immunol 4:565, 2004.
taining an irreplaceable immunological resource. Nat Rev
Labbok MH, Clark D, Goldman AS: Breastfeeding: main-
lactation. Endocr Rev 18:832, 1997.
bone metabolism during pregnancy, puerperium, and
Kovacs CS, Kronenberg HM: Maternal-fetal calcium and
286:F202, 2004.
in mammalian nephrogenesis. Am J Physiol Renal Physiol
cellular matrix, its receptors, and cell adhesion molecules
Kanwar YS, Wada J, Lin S, Danesh FR, et al: Update of extra-
Rev Neurosci 2:475, 2001.
Johnson MH: Functional brain development in humans. Nat
steroids. Acta Physiol Scand 181:549, 2004.
system in kidney development: role of COX-2 and adrenal
Jensen BL, Stubbe J, Madsen K, et al: The renin-angiotensin
Physiol 547:11, 2003.
quences of abnormal fetal pancreatic development. J
Holemans K, Aerts L, Van Assche FA: Lifetime conse-
tory system. Physiol Rev 79:325, 1999.
Hilaire G, Duron B: Maturation of the mammalian respira-
Physiol Rev 84:239, 2004.
sulinism in infancy: from basic science to clinical disease.
Dunne MJ, Cosgrove KE, Shepherd RM, et al: Hyperin-
News Physiol Sci 18:130, 2003.
de Castro F: Chemotropic molecules: guides for axonal
Rev 21:514, 2000.
paracrine regulation of birth at term and preterm. Endocr
Challis JRG, Matthews SG, Gibb W, Lye SJ: Endocrine and
181:529, 2004.
system in kidney development. Acta Physiol Scand
Chen Y, Lasaitiene D, Friberg P: The renin-angiotensin
Regul Integr Comp Physiol 278:R1391, 2000.
depression during fetal and postnatal life. Am J Physiol
Bissonnette JM: Mechanisms regulating hypoxic respiratory
parison of this chart with the baby’s actual development
chart for the infant during the first year of life. Com-
2 years of life. Figure 83–9 shows a normal progress
fontanels and sutures of the skull, which allows only 20
second year. This is also associated with closure of the
the adult brain mass and 55 per cent at 1 year, but it
At birth, the infant brain mass is only 26 per cent of
occur.
ated functions, such as vision, seem to require several
fully functional at birth. The brain cortex and its associ-
until the end of the first year of life. For this reason,
nervous system from maturity caused by training.
of the nervous system. It is extremely difficult to
1052
Unit XIV
Endocrinology and Reproduction
Behavioral Growth
Behavioral growth is principally a problem of maturity
dissociate maturity of the anatomical structures of the
Anatomical studies show that certain major tracts in the
central nervous system are not completely myelinated
it is frequently stated that the nervous system is not
months after birth for final functional development to
reaches almost adult proportions by the end of the
per cent additional growth of the brain beyond the first
is used for clinical assessment of mental and behavioral
growth.
References
pathfinding and cell migration during CNS development.
namic evaluation of the first trimester fetus with special
2000.
2004.
2004.