
380
CHAPTER 9
The Upper Limb
Fractures of the Radius and Ulna
A small subcutaneous bursa is present over the olecranon pro
Colles’ fracture because the distal fragment is displaced anteri
is a fracture of the distal end of the radius
Colles’ fracture
process can be produced by the pull of the triceps muscle. Good
the pull of the triceps muscle, which is inserted on the olecranon
the proximal third of the radius is fractured
Galeazzi’s fracture,
the shaft of the ulna is fractured by a force applied from behind.
supination, the normal anatomic relationship of the radius, ulna,
fragment of the radius is pronated and pulled medially by the
can occur from falls on the
Fractures of the head of the radius
outstretched hand. As the force is transmitted along the radius,
the head of the radius is driven sharply against the capitulum,
splitting or splintering the head (Fig. 9.10).
Fractures of the neck of the radius occur in young children
from falls on the outstretched hand (Fig. 9.10).
Fractures of the shafts of the radius and ulna may or may
not occur together (Fig. 9.10). Displacement of the fragments is
usually considerable and depends on the pull of the attached
muscles. The proximal fragment of the radius is supinated by the
supinator and the biceps brachii muscles (Fig. 9.10). The distal
pronator quadratus muscle. The strength of the brachioradialis
and extensor carpi radialis longus and brevis shortens and angu-
lates the forearm. In fractures of the ulna, the ulna angulates
posteriorly. To restore the normal movements of pronation and
and interosseous membrane must be regained.
A fracture of one forearm bone may be associated with a dis-
location of the other bone. In Monteggia’s fracture, for example,
There is a bowing forward of the ulnar shaft and an anterior dis-
location of the radial head with rupture of the anular ligament. In
and the distal end of the ulna is dislocated at the distal radioulnar
joint.
Fractures of the olecranon process can result from a fall on
the flexed elbow or from a direct blow. Depending on the loca-
tion of the fracture line, the bony fragment may be displaced by
process (Fig. 9.10). Avulsion fractures of part of the olecranon
functional return after any of these fractures depends on the
accurate anatomic reduction of the fragment.
resulting from a fall on the outstretched hand. It commonly
occurs in patients older than 50 years. The force drives the dis-
tal fragment posteriorly and superiorly, and the distal articular
surface is inclined posteriorly (Fig. 9.50). This posterior displace-
ment produces a posterior bump, sometimes referred to as the
“dinner-fork deformity” because the forearm and wrist resemble
the shape of that eating utensil. Failure to restore the distal artic-
ular surface to its normal position will severely limit the range of
flexion of the wrist joint.
Smith’s fracture is a fracture of the distal end of the radius
and occurs from a fall on the back of the hand. It is a reversed
-
orly (Fig. 9.50).
Olecranon Bursitis
-
cess of the ulna, and repeated trauma often produces chronic
bursitis.
C L I N I C A L N O T E S
A
B
FIGURE 9.50
Fractures of the distal end of the radius.
of the medial cutaneous nerve of the forearm (Fig. 9.38).
neous nerve, and from the anterior and posterior branches
nerve of the forearm, a continuation of the musculocuta
the anterior and posterior branches of the lateral cutaneous
to the skin of the forearm is from
sensory nerve supply
The
hand and fingers are shown in Figures 9.51 and 9.52.
The important muscles attached to the bones of the
only two for the thumb.
There are three phalanges for each of the fingers but
surfaces are posterior, lateral, and medial.
concave forward and is triangular in transverse section. Its
and 9.52). The shaft of each metacarpal bone is slightly
knuckles, articulate with the proximal phalanges (Figs. 9.51
distal row of the carpal bones; the heads, which form the
The bases of the metacarpal bones articulate with the
surface is directed laterally and not backward.
rotated medially through a right angle so that its extensor
the others but occupies a more anterior position. It is also
est and most mobile. It does not lie in the same plane as
The first metacarpal bone of the thumb is the short
(Figs. 9.51 and 9.52).
head
There are five metacarpal bones, each of which has a
Smith’s fracture.
Colles’ fracture.
A.
B.
The Metacarpals and Phalanges
base,
a shaft, and a
-
The Forearm
Skin
-
A narrow strip of skin down the middle of the
ior
poster
surface of the forearm is supplied by the posterior cutaneous
lateral side of the dorsal venous arch on the back of the
arises from the
cephalic vein
ficial fascia (Fig. 9.39). The
of the forearm lie in the super
superficial veins
The
nerve of the forearm.
-
Basic Anatomy
381
scaphoid
trapezoid
tubercle of scaphoid
abductor pollicis brevis
flexor pollicis brevis
opponens pollicis
ridge of trapezium
abductor pollicis longus
oblique head of adductor pollicis
first palmar interosseous
flexor carpi radialis
opponens pollicis
second palmar interosseous
abductor and
flexor pollicis brevis
adductor pollicis and
first palmar interosseous
transverse head of
adductor pollicis
flexor pollicis longus
thumb
palmar interossei
flexor digitorum superficialis
index
flexor digitorum profundus
middle
ring
little
third palmar interosseous
abductor and
flexor digiti minimi
fourth palmar interosseous
opponens digiti minimi
pisometacarpal ligament
hook of hamate
flexor digiti minimi
pisohamate ligament
abductor digiti minimi
pisiform
flexor carpi ulnaris
triquetral
hamate
lunate
capitate
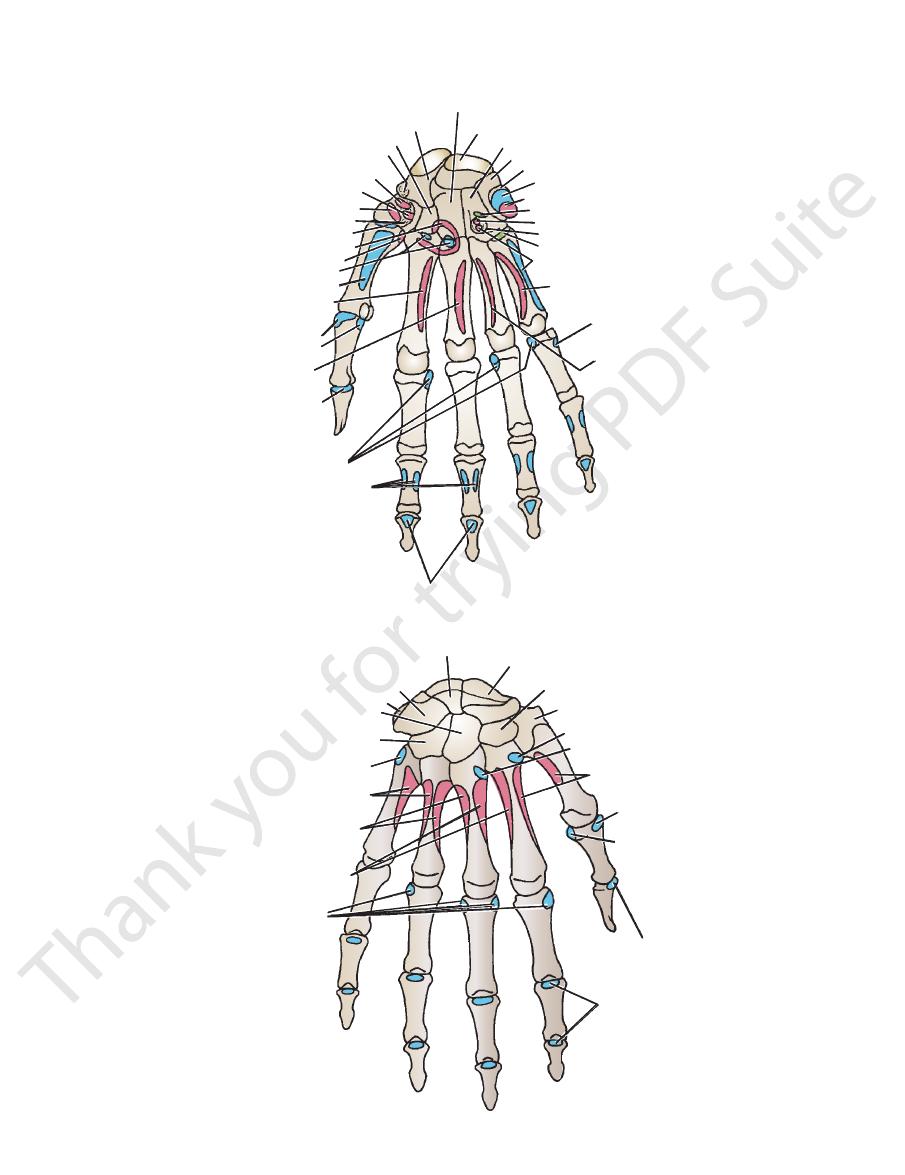
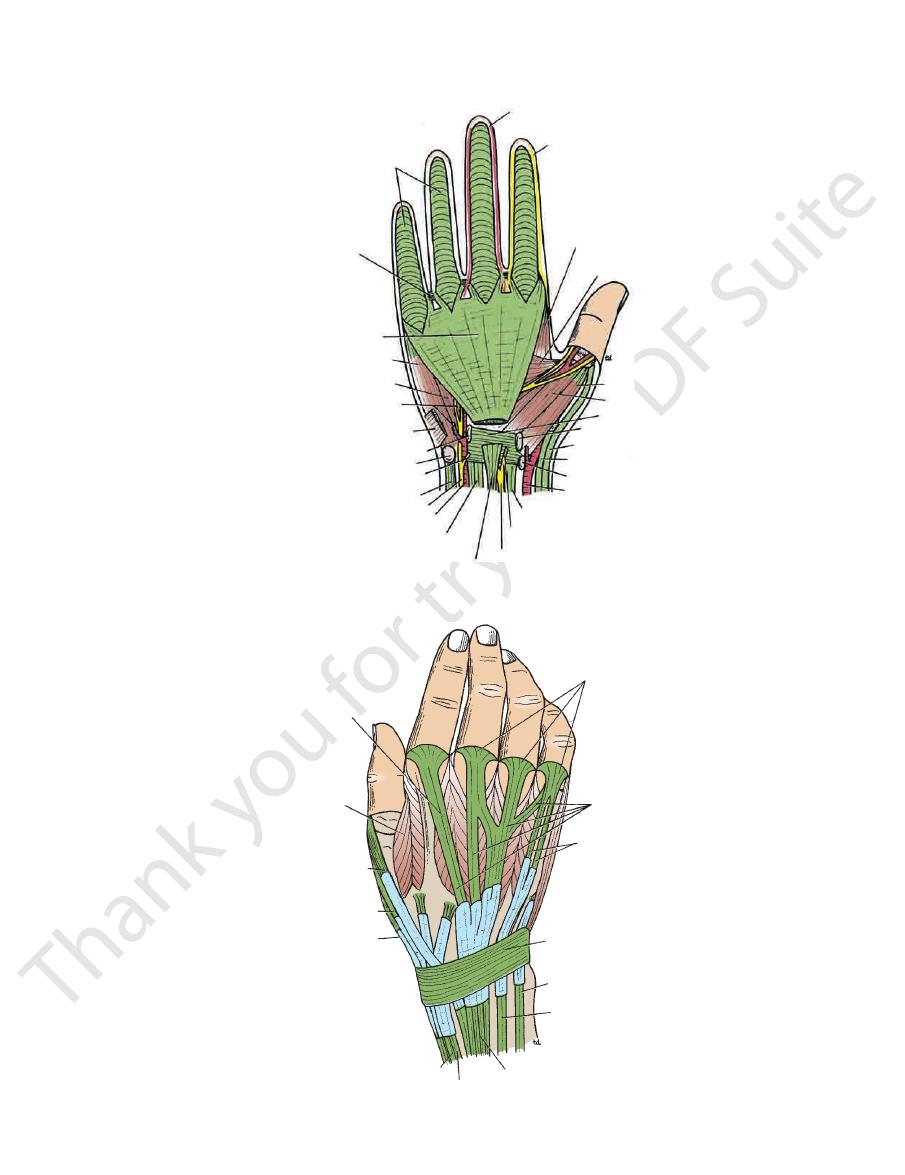
FIGURE 9.51
Important muscular attachments to the anterior surfaces of the bones of the hand.
lunate
triquetral
pisiform
capitate
hamate
extensor carpi ulnaris
fourth dorsal interosseous
third dorsal interosseous
second dorsal interosseous
dorsal interossei
extensor expansion
for extensor digitorum
extensor pollicis longus
adductor pollicis
extensor pollicis
brevis
first dorsal interosseous
extensor carpi radialis brevis
extensor carpi radialis longus
trapezium
trapezoid
scaphoid
FIGURE 9.52
Important muscular attachments to the posterior surfaces of the bones of the hand.
382
CHAPTER 9
blood supply.
compartments, each having its own muscles, nerves, and
intermuscular septa, divides the forearm into several
together with the interosseous membrane and fibrous
neous border of the ulna (Fig. 9.53). This fascial sheath,
is attached to the periosteum of the posterior subcuta
The forearm is enclosed in a sheath of deep fascia, which
also drain into the lateral axillary nodes (Fig. 9.40).
nodes. The efferent vessels from the supratrochlear node
axilla, where they drain into the lateral group of axillary
ers bypass the node and accompany the basilic vein to the
whereas oth
supratrochlear lymph node,
drain into the
basilic vein to the cubital fossa. Here, some of the vessels
the medial areas of the hand and the forearm follow the
of nodes (Fig. 9.40). Those from the medial fingers and
arm follow the cephalic vein to the infraclavicular group
lateral fingers and the lateral areas of the hand and fore
from the thumb and
superficial lymph vessels
The
posterior surfaces of the upper limb.
and a variable number of tributaries from the medial and
is described on page 351. It receives the median cubital vein
comitantes of the brachial artery to form the axillary vein,
the biceps (Fig. 9.39). Its termination, by joining the venae
tal fossa and up the front of the arm on the medial side of
medial border of the forearm; it then ascends into the cubi
venous arch on the back of the hand and winds around the
arises from the medial side of the dorsal
basilic vein
The
them by the bicipital aponeurosis.
chial artery and the median nerve, but it is separated from
tal fossa, the median cubital vein crosses in front of the bra
upward and medially and joins the basilic vein. In the cubi
a branch of the cephalic vein in the cubital fossa, runs
vein,
median cubital
terior surfaces of the limb (Fig. 9.39). The
a variable number of tributaries from the lateral and pos
As the cephalic vein passes up the upper limb, it receives
axillary vein in the deltopectoral triangle (see page 419).
arm on the lateral side of the biceps. It terminates in the
then ascends into the cubital fossa and up the front of the
hand and winds around the lateral border of the forearm; it
The Upper Limb
-
-
-
-
-
-
Fascial Compartments of the Forearm
-
Injuries to the Bones of the Hand
direct violence, such as the clenched fist striking a hard object.
adults who fall on the outstretched hand in a way that causes
outstretched hand in a young adult makes one suspicious of a
Fracture of the scaphoid bone is common in young adults; unless
treated effectively, the fragments will not unite, and permanent
weakness and pain of the wrist will result, with the subsequent
development of osteoarthritis. The fracture line usually goes
through the narrowest part of the bone, which, because of its
location, is bathed in synovial fluid. The blood vessels to the
scaphoid enter its proximal and distal ends, although the blood
supply is occasionally confined to its distal end. If the latter
occurs, a fracture deprives the proximal fragment of its arte-
rial supply, and this fragment undergoes avascular necrosis.
Deep tenderness in the anatomic snuffbox after a fall on the
fractured scaphoid.
Dislocation of the lunate bone occasionally occurs in young
hyperextension of the wrist joint. Involvement of the median
nerve is common.
Fractures of the metacarpal bones can occur as a result of
The fracture always angulates dorsally. The “boxer’s fracture”
commonly produces an oblique fracture of the neck of the fifth
and sometimes the fourth metacarpal bones. The distal fragment
is commonly displaced proximally, thus shortening the finger
posteriorly.
Bennett’s fracture is a fracture of the base of the metacarpal
of the thumb caused when violence is applied along the long axis
of the thumb or the thumb is forcefully abducted. The fracture is
oblique and enters the carpometacarpal joint of the thumb, caus-
ing joint instability.
Fractures of the phalanges are common and usually follow
direct injury.
C L I N I C A L N O T E S
Compartment Syndrome of the Forearm
diagnosis is made, the deep fascia must be incised surgically
by pressure on the arteries within the compartment). Once the
by edema), and absence of capillary refill in the nail beds (caused
tenderness of the skin over the compartment (a late sign caused
that pass through the compartment (caused by muscle ischemia),
within the compartment), pain on passive stretching of muscles
pain disproportionate to any injury (caused by pressure on nerves
emia of the sensory nerves passing through the compartment),
Soft tissue injury is a common cause, and early diagnosis is
of the ulna (Fig. 9.53). This fascial sheath, together with the inter
The forearm is enclosed in a sheath of deep fascia, which is
attached to the periosteum of the posterior subcutaneous border
-
osseous membrane and fibrous intermuscular septa, divides the
forearm into several compartments, each having its own mus-
cles, nerves, and blood supply. There is very little room within
each compartment, and any edema can cause secondary vascu-
lar compression of the blood vessels; the veins are first affected,
and later the arteries.
critical. Early signs include altered skin sensation (caused by isch-
C L I N I C A L N O T E S
(continued)
Basic Anatomy
and the flexor tendons of the thumb and fingers (Fig. 9.54).
for the passage of the median nerve
carpal tunnel,
nel, the
cave anterior surface of the hand into an osteofascial tun
stretches across the front of the wrist and converts the con
holds the long flexor tendons in position at the wrist. It
The flexor retinaculum is a thickening of deep fascia that
Flexor Retinaculum
position at the wrist.
fascia that hold the long flexor and extensor tendons in
The flexor and extensor retinacula are strong bands of deep
Flexor and Extensor Retinacula
muscles.
seous membrane provides attachment for neighboring
position—that is, the position of function. The interos
Its fibers are taut when the forearm is in the midprone
to the ulna and from there to the humerus and scapula.
the outstretched hand) is transmitted from the radius
applied to the lower end of the radius (e.g., falling on
ers run obliquely downward and medially so that a force
to their interosseous borders (Figs. 9.49 and 9.53). Its fib
unites the shafts of the radius and the ulna; it is attached
The interosseous membrane is a strong membrane that
Interosseous Membrane
383
-
-
-
-
to decompress the affected compartment. A delay of as little as
langeal joints are extended, and the interphalangeal joints
Both the flexor and extensor muscles of the forearm are
4 hours can cause irreversible damage to the muscles.
Volkmann’s Ischemic Contracture
Volkmann’s ischemic contracture is a contracture of the mus-
cles of the forearm that commonly follows fractures of the distal
end of the humerus or fractures of the radius and ulna. In this
syndrome, a localized segment of the brachial artery goes into
spasm, reducing the arterial flow to the flexor and the exten-
sor muscles so that they undergo ischemic necrosis. The flexor
muscles are larger than the extensor muscles, and they are
therefore the ones mainly affected. The muscles are replaced
by fibrous tissue, which contracts, producing the deformity. The
arterial spasm is usually caused by an overtight cast, but in some
cases the fracture itself may be responsible. The deformity can
be explained only by understanding the anatomy of the region.
Three types of deformity exist:
■
■
The long flexor muscles of the carpus and fingers are more
contracted than the extensor muscles, and the wrist joint is
flexed; the fingers are extended. If the wrist joint is extended
passively, the fingers become flexed.
■
■
The long extensor muscles to the fingers, which are inserted
into the extensor expansion that is attached to the proximal
phalanx, are greatly contracted; the metacarpophalangeal
joints and the wrist joint are extended, and the interphalan-
geal joints of the fingers are flexed.
■
■
contracted. The wrist joint is flexed, the metacarpopha-
are flexed.
palmaris longus
ulnar nerve and artery
flexor carpi ulnaris
anterior interosseous
nerve and artery
flexor digitorum profundus
ulna
extensor pollicis longus
extensor carpi ulnaris
extensor digiti minimi
posterior interosseous nerve and artery
abductor pollicis longus
supinator
radius
extensor digitorum
extensor carpi
radialis brevis
extensor carpi
radialis longus
brachioradialis
flexor pollicis
longus
pronator teres
superficial branch of
radial nerve
radial artery
flexor carpi radialis
median nerve
flexor digitorum superficialis
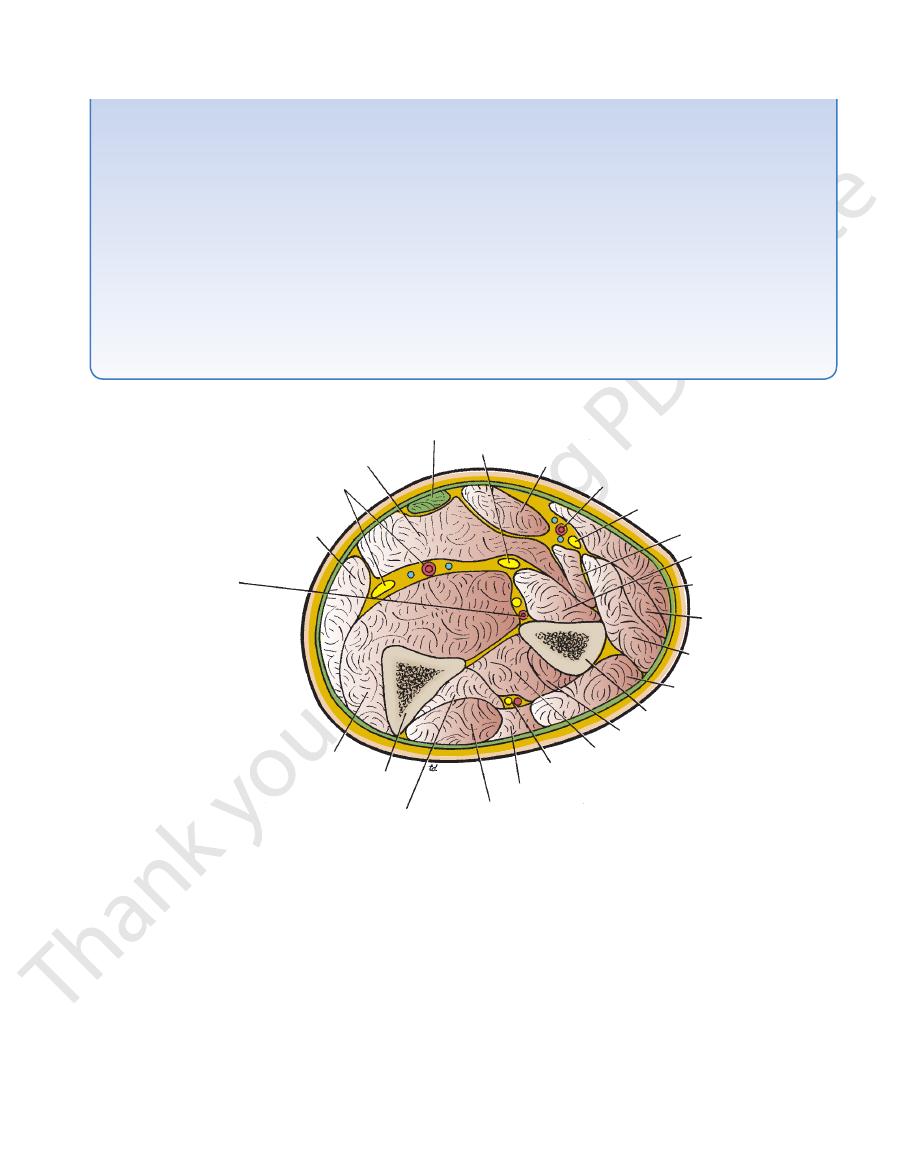
FIGURE 9.53
Cross section of the forearm at the level of insertion of the pronator teres muscle.
384
CHAPTER 9
from one another by fibrous septa that pass from the deep
retinaculum on the tendons. The tunnels are separated
with a synovial sheath, which extends above and below the
passage of the long extensor tendons. Each tunnel is lined
ends of the radius and ulna into six separate tunnels for the
It converts the grooves on the posterior surface of the distal
long extensor tendons in position (Figs. 9.56 and 9.57).
that stretches across the back of the wrist and holds the
The extensor retinaculum is a thickening of deep fascia
Extensor Retinaculum
(Fig. 9.55).
The lower border is attached to the palmar aponeurosis
and is continuous with the deep fascia of the forearm.
to the distal transverse skin crease in front of the wrist
The upper border of the retinaculum corresponds
radialis.
lined tunnel for passage of the tendon of the flexor carpi
consists of superficial and deep parts and forms a synovial-
and the trapezium bones. The attachment to the trapezium
of the hamate and laterally to the tubercle of the scaphoid
It is attached medially to the pisiform bone and the hook
The Upper Limb
surface of the retinaculum to the bones.
bone and the hook of the hamate and laterally to the
The retinaculum is attached medially to the pisiform
distal end of the radius. The upper and lower borders of
the retinaculum are continuous with the deep fascia of the
nerve.
digitorum profundus, which are supplied by the ulnar
flexor carpi ulnaris and the medial part of the flexor
plied by the median nerve and its branches, except the
All the muscles are sup
Nerve supply to the muscles:
Ulnar and radial arteries
Blood supply to the muscles:
digitorum profundus, and the pronator quadratus
consisting of the flexor pollicis longus, the flexor
group
deep
sisting of the flexor digitorum superficialis; and a
con
intermediate group
and the flexor carpi ulnaris; an
tor teres, the flexor carpi radialis, the palmaris longus,
consisting of the prona
superficial group,
A
Muscles:
of the Forearm
Contents of the Anterior Fascial Compartment
further details, see page 398.
rum superficialis and the flexor carpi radialis muscles. For
between the tendons of the flexor digito
restricted space
the carpal tunnel (Fig. 9.54). The median nerve lies in a
The bones of the hand and the flexor retinaculum form
Carpal Tunnel
naculum are described on page 397.
The contents of the tunnels beneath the extensor reti
forearm and hand, respectively.
-
-
■
■
-
-
■
■
■
■
-
palmaris longus
flexor retinaculum
palmar cutaneous branch
of ulnar nerve
muscles of
hypothenar eminence
ulnar artery
ulnar nerve
flexor digitorum
superficialis
flexor digitorum
profundus
hook of hamate
flexor synovial sheath
extensor carpi ulnaris
posterior cutaneous branch of
ulnar nerve
basilic vein
extensor digiti minimi
extensor digitorum
extensor indicis
extensor retinaculum
extensor pollicis longus
extensor carpi radialis
longus and brevis
cephalic vein
radial artery
superficial branch
of radial nerve
extensor pollicis brevis
abductor pollicis longus
flexor pollicis longus
ridge of trapezium
flexor carpi radialis
muscles of thenar eminence
palmar cutaneous branch of median nerve
median nerve
hamate
capitate
trape-
zoid
trap
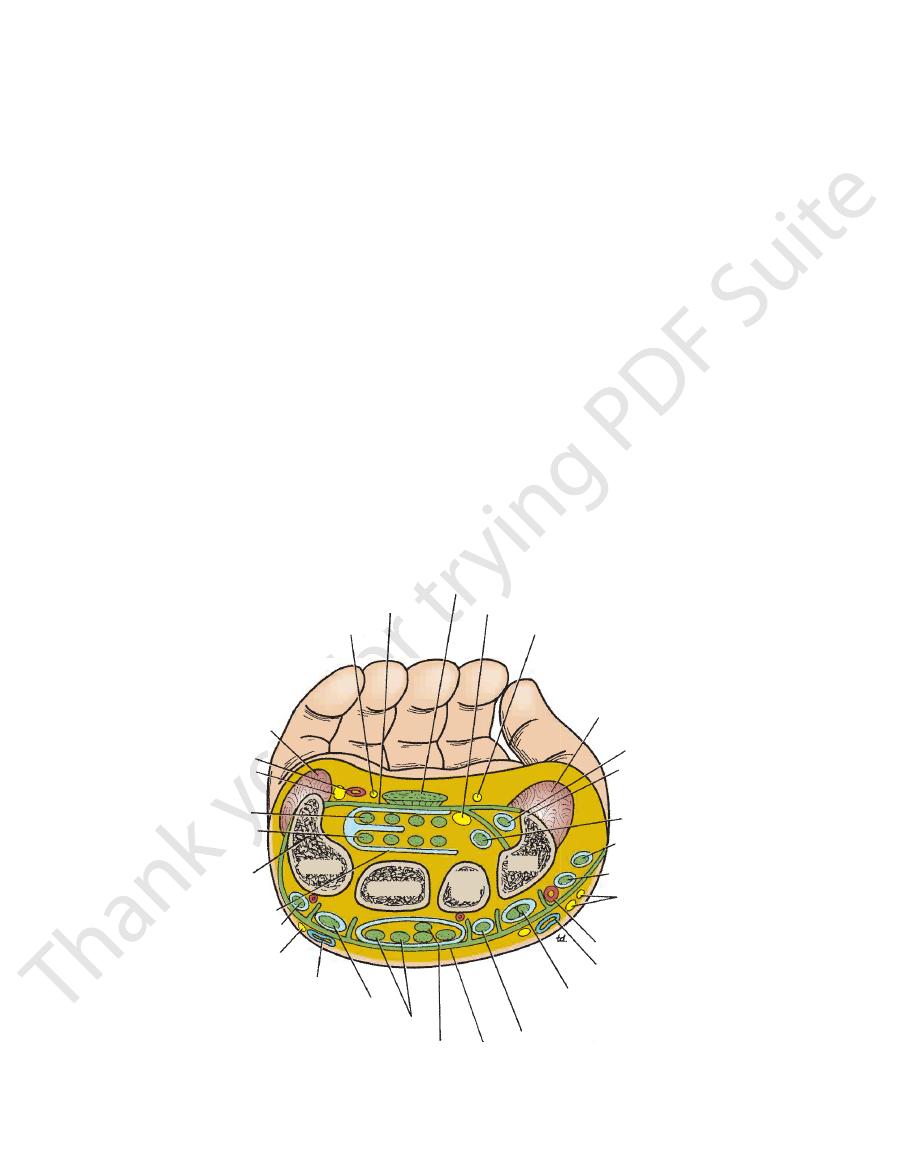
FIGURE 9.54
xor and extensor
Cross section of the hand showing the relation of the tendons, nerves, and arteries to the fle
retinacula.
Basic Anatomy
385
fibrous flexor sheath
deep transverse palmar ligament
palmar aponeurosis
abductor digiti minimi
flexor digiti minimi
deep branch of ulnar nerve and artery
palmaris brevis
hook of hamate
pisiform
palmar cutaneous branchof ulnar nerve
flexor carpi ulnaris
ulnar nerve
ulnar artery
flexor digitorum superficialis
palmaris longus
median nerve
palmar cutaneous branch
of median nerve
flexor carpi radialis
radial artery
tubercle of scaphoid
abductor pollicis longus
extensor pollicis brevis
ridge of trapezium
flexor retinaculum
flexor pollicis brevis
abductor pollicis brevis
adductor pollicis
first dorsal interosseous
palmar digital nerve
palmar digital artery
FIGURE 9.55
Anterior view of the palm of the hand. The palmar aponeurosis has been left in position.
extensor indicis
first dorsal interosseous
extensor pollicis longus
extensor pollicis brevis
abductor pollicis longus
extensor carpi radialis longus
extensor carpi radialis brevis
extensor digitorum
extensor digiti minimi
extensor carpi ulnaris
extensor retinaculum
extensor digiti minimi
extensor digitorum
dorsal extensor expansion
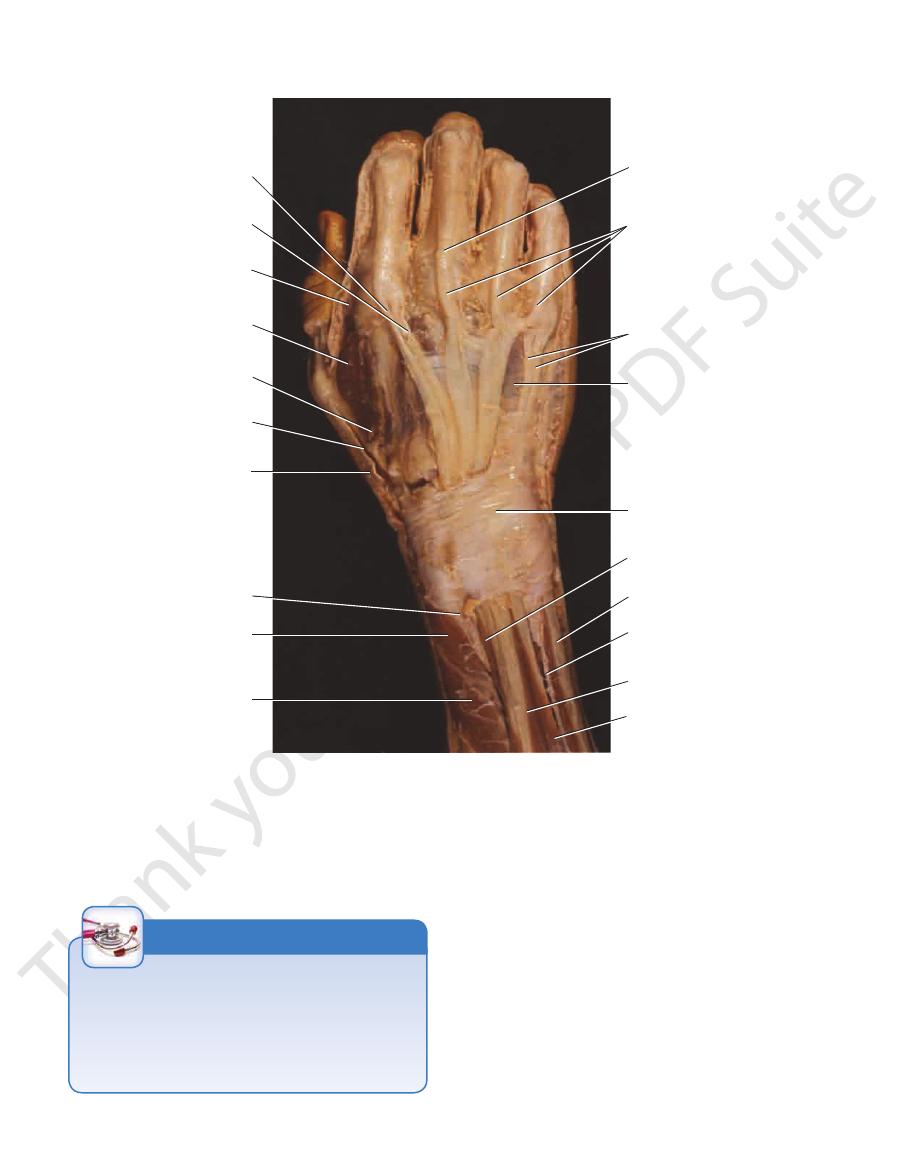
FIGURE 9.56
Dorsal surface of the hand showing the long extensor tendons and their synovial sheaths.
386
CHAPTER 9
The Upper Limb
extensor
digitorum
extensor
expansion
extensor
digitorum
extensor
digiti
minimi
extensor
digiti
minimi
extensor
retinaculum
extensor
pollicis
longus
extensor
carpi
ulnaris
extensor
digitorum
ulna
fourth
dorsal
interosseous
extensor
indicis
digital
vein
first
dorsal
interosseous
radial
artery
extensor
pollicis
longus
abductor
pollicis
longus
extensor
pollicis
brevis
extensor
pollicis
brevis
radius
FIGURE 9.57
Dissection of the dorsal surface of the right hand showing the long extensor tendons and the extensor retinaculum.
Absent Palmaris Longus
The palmaris longus muscle may be absent on one or both
sides of the forearm in about 10% of persons. Others show
variation in form, such as centrally or distally placed muscle
belly in the place of a proximal one. Because the muscle is
relatively weak, its absence produces no disability.
C L I N I C A L N O T E S
Muscles of the Anterior Fascial Compartment of
minal branches of the brachial artery (Figs. 9.42 and 9.60).
The ulnar artery is the larger of the two ter
Ulnar Artery
the Forearm
Arteries of the Anterior Fascial Compartment of
epicondyle of the humerus.
common tendon of origin, which is attached to the medial
9.6. Note that the superficial group of muscles possesses a
Figures 9.58, 9.59, 9.60, and 9.61 and are described in Table
The muscles of the anterior fascial compartment are seen in
the Forearm
-
Basic Anatomy
bone and is covered only by skin and fascia (site for taking
of the flexor retinaculum, it lies just lateral to the pisiform
the tendons of the flexor digitorum superficialis. In front
and lies between the tendons of the flexor carpi ulnaris and
to most of the flexor muscles. Below, it becomes superficial
In the upper part of its course, the ulnar artery lies deep
artery (Fig. 9.62).
tomosing with the superficial palmar branch of the radial
often anas
superficial palmar arch,
It ends by forming the
retinaculum in company with the ulnar nerve (Fig. 9.62).
the flexor
in front of
of the forearm and enters the palm
the radius. It descends through the anterior compartment
It begins in the cubital fossa at the level of the neck of
387
-
ulnar pulse).
Muscles of the Anterior Fascial Compartment of the Forearm
T A B L E 9 . 6
Pronator Teres
Muscle
Origin
Insertion
Nerve Supply
Nerve
Roots
a
Action
Humeral head
Medial epicondyle of
humerus
Lateral aspect of shaft
of radius
Median nerve
C6, 7
Pronation and flexion of
forearm
Ulnar head
Medial border of
coronoid process of
ulna
Flexor carpi
radialis
Medial epicondyle of
humerus
Bases of second and
third metacarpal
bones
Median nerve
C6, 7
Flexes and abducts
hand at wrist joint
Palmaris
longus
Medial epicondyle of
humerus
Flexor retinaculum and
palmar aponeurosis
Median nerve
C7, 8
Flexes hand
Flexor Carpi Ulnaris
Humeral head
Medial epicondyle of
humerus
Pisiform bone, hook of
the hamate, base at
fifth metacarpal bone
Ulnar nerve
C8; T1
Flexes and adducts
hand at wrist joint
Ulnar head
Medial aspect of
olecranon process
and posterior border
of ulna
Flexor Digitorum Superficialis
Humeroulnar
head
Medial epicondyle of
humerus; medial
border of coronoid
process of ulna
Middle phalanx of
medial four fingers
Median nerve
C7, 8; T1
Flexes middle phalanx
of fingers and assists
in flexing proximal
phalanx and hand
Radial head
Oblique line on anterior
surface of shaft of
radius
Flexor pollicis
longus
Anterior surface of shaft
of radius
Distal phalanx of thumb
Anterior interosseous
branch of median
nerve
C8; T1
Flexes distal phalanx of
thumb
Flexor
digitorum
profundus
Anteromedial surface of
shaft of ulna
Distal phalanges of
medial four fingers
Ulnar (medial half)
and median (lateral
half) nerves
C8; T1
Flexes distal phalanx
of fingers; then
assists in flexion of
middle and proximal
phalanges and wrist
Pronator
quadratus
Anterior surface of shaft
of ulna
Anterior surface of shaft
of radius
Anterior interosseous
branch of median
nerve
C8; T1
Pronates forearm
a
The predominant nerve root supply is indicated by boldface type.
388
CHAPTER 9
and
anterior
divides into the
the upper part of the ulnar artery and after a brief course
which arises from
common interosseous artery,
The
around the wrist joint
Branches that take part in the arterial anastomosis
mosis around the elbow joint (Fig. 9.61)
that take part in the arterial anasto
Recurrent branches
to neighboring muscles
Muscular branches
Branches
The Upper Limb
■
■
■
■
-
■
■
■
■
posterior
osseous
inter
(Fig. 9.61). The interosseous arteries are
arteries
distributed to the muscles lying in front of and behind
its lateral side.
course, the superficial branch of the radial nerve lies on
deep muscles of the forearm. In the middle third of its
beneath the brachioradialis muscle and resting on the
9.58, 9.59, and 9.60). It passes downward and laterally,
cubital fossa at the level of the neck of the radius (Figs.
minal branches of the brachial artery. It begins in the
The radial artery is the smaller of the ter
Radial Artery
ies to the radius and ulna bone.
the interosseous membrane; they provide nutrient arter-
-
musculocutaneous nerve becoming
lateral cutaneous nerve of forearm
brachioradialis
extensor carpi radialis longus
biceps tendon
extensor carpi radialis brevis
supinator
superficial branch of radial nerve
pronator teres
abductor pollicis longus
radial artery
extensor pollicis brevis
pronator quadratus
abductor pollicis longus
radius
flexor retinaculum
median nerve
ulnar nerve and artery
flexor digitorum superficialis
flexor carpi ulnaris
palmaris longus
flexor carpi radialis
bicipital aponeurosis
ulnar artery
pronator teres
medial intermuscular septum
median nerve
brachial artery
brachialis
biceps brachii
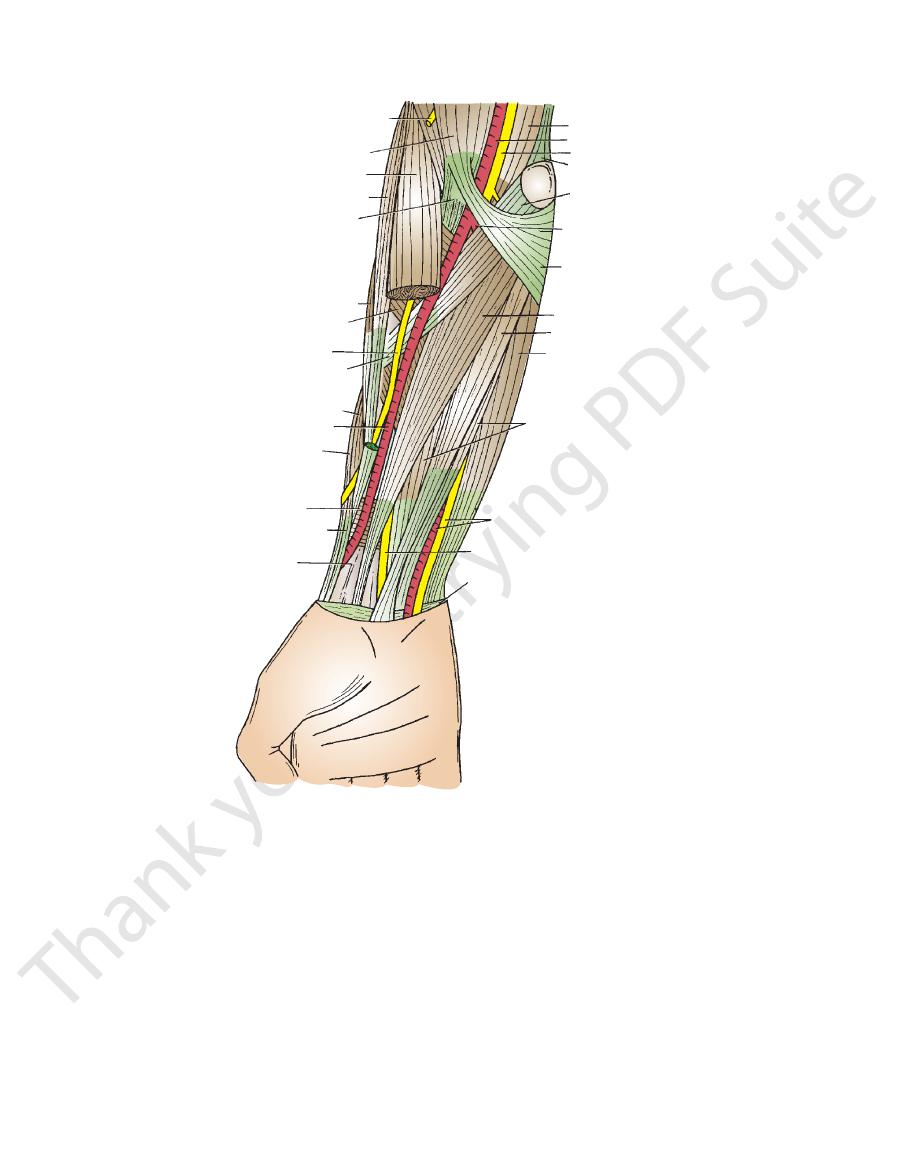
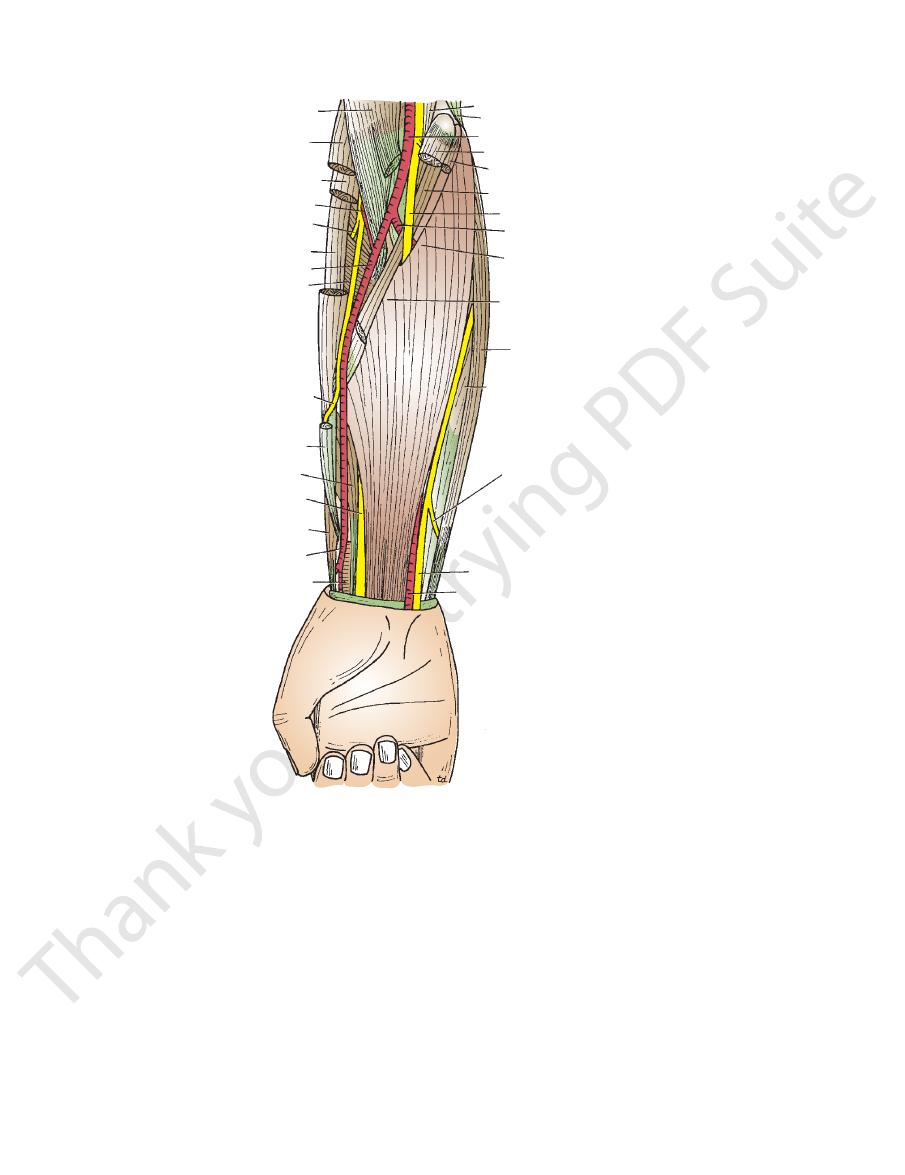
FIGURE 9.58
he middle portion of the brachioradialis muscle has been removed to display the
Anterior view of the forearm. T
superficial branch of the radial nerve and the radial artery.

Basic Anatomy
389
palmar
digital arteries
and nerves
flexor pollicis
brevis
abductor pollicis
brevis
abductor digiti
minimi
abductor pollicis
longus
flexor
retinaculum
radial artery
flexor carpi
radialis
brachioradialis
flexor digitorum
superficialis
tendons of
flexor digitorum
superficialis
median nerve
ulnar artery
pisiform bone
ulnar nerve
superficial palmar
arch
fibrous flexor
sheath
FIGURE 9.59
uctures.
Dissection of the front of the left forearm and hand showing the superficial str
(Fig. 9.61). It ends on the anterior surface of the carpus.
flexor pollicis longus and the flexor digitorum profundus
anterior surface of the interosseous membrane, between the
two heads of the pronator teres. It passes downward on the
arises from the median nerve as it emerges from between the
The anterior interosseous nerve
Anterior Interosseous Nerve
lateral part of the palm (Fig. 9.38).
of the forearm and is distributed to the skin over the
This arises in the lower part
Palmar cutaneous branch.
Anterior interosseous nerve
to the elbow joint
Articular branches
the flexor digitorum superficialis (Fig. 9.22)
teres, the flexor carpi radialis, the palmaris longus, and
in the cubital fossa to the pronator
Muscular branches
Branches
the flexor retinaculum (see pages 394
behind
longus (Figs. 9.58, 9.59, and 9.60). It enters the palm by
cialis muscle and lies behind the tendon of the palmaris
from the lateral border of the flexor digitorum superfi
itorum profundus. At the wrist, the median nerve emerges
torum superficialis and rests posteriorly on the flexor dig
(Fig. 9.60). It continues downward behind the flexor digi
by passing between the two heads of the pronator teres
The median nerve leaves the cubital fossa
Median Nerve
the Forearm
Nerves of the Anterior Fascial Compartment of
palmar arch
superficial
quently joins the ulnar artery to form the
wrist (Fig. 9.60), enters the palm of the hand, and fre
which arises just above the
Superficial palmar branch,
tomosis around the elbow joint (Fig. 9.60)
which takes part in the arterial anas
Recurrent branch,
to neighboring muscles
Muscular branches
Branches in the Forearm
of the hand (see page 406).
the lateral aspect of the wrist to reach the posterior surface
The radial artery leaves the forearm by winding around
carpi radialis on its medial side (site for taking the radial
chioradialis on its lateral side and the tendon of flexor
by skin and fascia. Here, the artery has the tendon of bra
on the anterior surface of the radius and is covered only
In the distal part of the forearm, the radial artery lies
-
pulse).
■
■
■
■
-
■
■
-
-
-
-
passing
and 395).
■
■
■
■
■
■
■
■
390
CHAPTER 9
to the elbow joint
Articular branches
(Fig. 9.23)
to the medial half of the flexor digitorum profundus
to the flexor carpi ulnaris and
Muscular branches
Branches
here, it has the ulnar artery lateral to it (see page 394).
the flexor retinaculum and lateral to the pisiform bone;
in front
ulnar nerve enters the palm of the hand by passing
digitorum superficialis muscles (Figs. 9.58 and 9.59). The
between the tendons of the flexor carpi ulnaris and flexor
At the wrist, the ulnar nerve becomes superficial and lies
artery lies on the lateral side of the ulnar nerve (Fig. 9.61).
muscles. In the distal two thirds of the forearm, the ulnar
flexor carpi ulnaris and the flexor digitorum profundus
carpi ulnaris. It then runs down the forearm between the
the forearm by passing between the two heads of the flexor
medial ligament of the elbow joint, and enters the front of
behind the medial epicondyle of the humerus, crosses the
The ulnar nerve (Fig. 9.61) passes from
Ulnar Nerve
joints. It also supplies the joints of the hand.
to the wrist and distal radioulnar
Articular branches
rum profundus
nator quadratus, and the lateral half of the flexor digito
to the flexor pollicis longus, the pro
Muscular branches
Branches
The Upper Limb
■
■
-
-
■
■
of
■
■
■
■
biceps brachii
brachioradialis
extensor carpi radialis longus
radial recurrent artery
deep branch of radial nerve
extensor carpi radialis brevis
radial artery
supinator
superficial branch of radial nerve
brachioradialis
flexor pollicis longus
median nerve
abductor pollicis longus
radial artery
pronator quadratus
ulnar artery
ulnar nerve
posterior cutaneous branch of ulnar nerve
flexor digitorum profundus
flexor carpi ulnaris
radial head of flexor digitorum superficialis
humeral head of flexor digitorum superficialis
median nerve
ulnar head of pronator teres
flexor carpi radialis
humeral head of pronator teres
brachial artery
medial intermuscular septum
brachialis
ulnar artery
FIGURE 9.60
e been removed to display the flexor digitorum
Anterior view of the forearm. Most of the superficial muscles hav
teres separates the median nerve from the ulnar artery.
superficialis, median nerve, superficial branch of the radial nerve, and radial artery. Note that the ulnar head of the pronator

Basic Anatomy
Brachioradialis and extensor carpi radialis
Muscles:
the posterior fascial compartment.
The lateral fascial compartment may be regarded as part of
the Forearm
Contents of the Lateral Fascial Compartment of
surface of the hand and fingers.
ulnaris and the ulna and is distributed on the posterior
passes medially between the tendon of the flexor carpi
branch that arises in the distal third of the forearm. It
is a large
dorsal posterior cutaneous branch
The
plies the skin over the hypothenar eminence.
arises in the middle of the forearm (Fig. 9.38) and sup
is a small branch that
palmar cutaneous branch
The
391
■
■
-
■
■
■
■
longus
Radial and brachial arteries
Blood supply:
■
■
brachialis
radial nerve
lateral epicondyle
radial artery
superficial
branch of radial nerve
oblique cord
supinator
deep branch of radial nerve
radial head of flexor
digitorum superficialis
pronator teres
interosseous membrane
flexor pollicis longus
abductor pollicis longus
branch of anterior
interosseous artery
pronator quadratus
anterior interosseous nerve
anterior interosseous artery
flexor digitorum profundus
ulnar artery
ulnar nerve
posterior interosseous artery
common interosseous artery
posterior ulnar recurrent artery
medial epicondyle
anterior ulnar recurrent artery
median nerve
brachial artery
FIGURE 9.61
uctures.
Anterior view of the forearm showing the deep str

392
CHAPTER 9
the neck of the radius, within the supinator muscle
This winds around
Deep branch of the radial nerve.
to the elbow joint
Articular branches
eral part of the brachialis muscle (Fig. 9.25)
sor carpi radialis longus, and a small branch to the lat
to the brachioradialis, to the exten
Muscular branches
Branches
(Figs. 9.60 and 9.61).
epicondyle, it divides into superficial and deep branches
on the lateral side (Fig. 9.60). At the level of the lateral
and the brachioradialis and extensor carpi radialis longus
humerus, lying between the brachialis on the medial side
passes downward in front of the lateral epicondyle of the
passes forward into the cubital fossa (Fig. 9.47). It then
muscular septum in the lower part of the arm and
The radial nerve pierces the lateral inter
Radial Nerve
Nerve of the Lateral Compartment of the Forearm
and brachial arteries.
The arterial supply is derived from branches of the radial
Forearm
Arteries of the Lateral Compartment of the
Table 9.7.
arm are seen in Figures 9.58 and 9.60 and are described in
The muscles of the lateral fascial compartment of the fore
Forearm
Muscles of the Lateral Fascial Compartment of the
Radial nerve
Nerve supply to the muscles:
The Upper Limb
■
■
-
-
■
■
-
-
■
■
■
■
(Fig. 9.61), and enters the posterior compartment of the
the tendon of the brachioradialis (Fig. 9.60). It reaches the
forearm, it leaves the artery and passes backward under
the lateral side of the radial artery. In the distal part of the
It runs down under cover of the brachioradialis muscle on
front of the lateral epicondyle of the humerus (Fig. 9.60).
nerve after its main stem has given off its deep branch in
branch of the radial nerve is the direct continuation of the
The superficial
Superficial Branch of the Radial Nerve
Superficial branch of the radial nerve
forearm (Fig. 9.61).
■
■
posterior surface of the wrist, where it divides into terminal
rior surface over the proximal phalanges of the lateral three
the posterior surface of the hand (Fig. 9.38) and the poste
branches that supply the skin on the lateral two thirds of
-
fibrous flexor sheaths
flexor digitorum superficialis
flexor digitorum profundus
palmar digital arteries and nerves
opponens digiti minimi
superficial palmar arch
flexor digiti minimi
abductor digiti minimi
hook of hamate
pisiform
flexor carpi ulnaris
flexor retinaculum
ulnar nerve and artery
flexor digitorum superficialis
flexor digitorum profundus
median nerve
flexor pollicis longus
flexor carpi radialis
tubercle of scaphoid
radial artery
abductor pollicis longus
ridge of trapezium
abductor pollicis brevis
flexor pollicis brevis
opponens pollicis
adductor pollicis
first dorsal interosseous
first lumbrical
FIGURE 9.62
xor retinaculum
Anterior view of the palm of the hand. The palmar aponeurosis and the greater part of the fle
tendons of the flexor digitorum superficialis have been removed to show the underlying tendons of the flexor digitorum
have been removed to display the superficial palmar arch, the median nerve, and the long flexor tendons. Segments of the
profundus.
Basic Anatomy
in Figures 9.64 and 9.65 and are described in Table 9.8.
The muscles of the posterior fascial compartment are seen
the Forearm
Muscles of the Posterior Fascial Compartment of
nerve
Deep branch of the radial
Nerve supply to the muscles:
Posterior and anterior interosseous arteries
Blood supply:
and extensor indicis.
longus, extensor pollicis brevis, extensor pollicis longus,
includes the supinator, abductor pollicis
deep group
attached to the lateral epicondyle of the humerus. The
muscles possess a common tendon of origin, which is
minimi, extensor carpi ulnaris, and anconeus. These
carpi radialis brevis, extensor digitorum, extensor digiti
includes the extensor
superficial group
The
Muscles:
of the Forearm
Contents of the Posterior Fascial Compartment
the dorsum of the hand is variable.
and a half fingers. The area of skin supplied by the nerve on
393
■
■
■
■
■
■
Stenosing Synovitis of the Abductor Pollicis
Longus and Extensor Pollicis Brevis Tendons
As a result of repeated friction between these tendons and the
styloid process of the radius, they sometimes become edema-
tous and swell. Later, fibrosis of the synovial sheath produces
a condition known as stenosing tenosynovitis in which move-
ment of the tendons becomes restricted. Advanced cases
require surgical incision along the constricting sheath.
C L I N I C A L N O T E S
Arteries of the Posterior Fascial Compartment of
around the wrist joint.
and bones. They end by taking part in the anastomosis
membrane, respectively, and supply the adjoining muscles
on the anterior and posterior surfaces of the interosseous
ulnar artery (Figs. 9.61 and 9.65). They pass downward
from the common interosseous artery, a branch of the
arise
posterior interosseous arteries
anterior
The
the Forearm
and
is bounded medially by the tendon of the extensor pollicis lon
triangular skin depression on the lateral side of the wrist that
tendon, which can then rupture. Rheumatoid arthritis can also
third of the radius. Roughening of the dorsal tubercle of the
Rupture of the Extensor Pollicis Longus Tendon
Rupture of this tendon can occur after fracture of the distal
radius by the fracture line can cause excessive friction on the
cause rupture of this tendon.
“Anatomic Snuffbox”
The anatomic snuffbox is a term commonly used to describe a
-
gus and laterally by the tendons of the abductor pollicis longus
and extensor pollicis brevis (Fig. 9.64). Its clinical importance
lies in the fact that the scaphoid bone is most easily palpated
here and that the pulsations of the radial artery can be felt
here (Fig. 9.100).
C L I N I C A L N O T E S
Tennis Elbow
Tennis elbow is caused by a partial tearing or degeneration of
the origin of the superficial extensor muscles from the lateral
epicondyle of the humerus. It is characterized by pain and ten-
derness over the lateral epicondyle of the humerus, with pain
radiating down the lateral side of the forearm; it is common in
tennis players, violinists, and housewives.
C L I N I C A L N O T E S
Muscles of the Lateral Fascial Compartment of the Forearm
T A B L E 9 . 7
Muscle
Origin
Insertion
Nerve Supply
Nerve Roots
a
Action
Brachioradialis
Lateral supracon-
dylar ridge of
humerus
Base of styloid pro-
cess of radius
Radial nerve
C5, 6, 7
Flexes forearm
at elbow joint;
rotates forearm
to the midprone
position
Extensor carpi
radialis longus
Lateral supracon-
dylar ridge of
humerus
Posterior surface
of base of sec-
ond metacarpal
bone
Radial nerve
C6, 7
Extends and
abducts hand at
wrist joint
a
The predominant nerve root supply is indicated by boldface type.

394
CHAPTER 9
Palmar cutaneous branch of the median nerve
aponeurosis
insertion into the flexor retinaculum and the palmar
(if present), passing to its
Palmaris longus tendon
Palmar cutaneous branch of the ulnar nerve
lies lateral to the ulnar nerve.
Ulnar artery
lies lateral to the pisiform bone.
Ulnar nerve
inaculum but is included for the sake of completeness.)
bone. (This tendon does not actually cross the flexor ret
ending on the pisiform
Flexor carpi ulnaris tendon,
naculum from medial to lateral (Fig. 9.54):
The following structures pass superficial to the flexor reti
Wrist
structures as possible.
time, examine your own wrist and identify as many of the
identify the structures from medial to lateral. At the same
In a transverse section through the wrist (Fig. 9.54),
for injury.
joint. From a clinical standpoint, the wrist is a common site
the tendons, arteries, and nerves in the region of the wrist
a student have a sound knowledge of the arrangement of
Before learning the anatomy of the hand, it is essential that
The Region of the Wrist
to the wrist and carpal joints
Articular branches
pollicis longus, and the extensor indicis
pollicis longus, the extensor pollicis brevis, the extensor
digiti minimi, the extensor carpi ulnaris, the abductor
and the supinator, the extensor digitorum, the extensor
to the extensor carpi radialis brevis
Muscular branches
Branches
face of the wrist joint.
muscles (Fig. 9.65). It eventually reaches the posterior sur
in the interval between the superficial and deep groups of
posterior compartment of the forearm. The nerve descends
of the radius in the substance of the muscle to reach the
supinator and winds around the lateral aspect of the neck
the humerus in the cubital fossa (Fig. 9.61). It pierces the
from the radial nerve in front of the lateral epicondyle of
The deep branch arises
Deep Branch of the Radial Nerve
Forearm
Nerve of the Posterior Fascial Compartment of the
The Upper Limb
-
■
■
■
■
Structures on the Anterior Aspect of the
-
■
■
-
■
■
■
■
■
■
■
■
■
■
FIGURE 9.63
Insertions of long flexor and extensor tendons in the fingers. Insertions of the lumbrical and interossei muscles
pophalangeal joints and extending the interphalangeal joints.
are also shown. The uppermost figure illustrates the action of the lumbrical and interossei muscles in flexing the metacar-
extensor digitorum
interossei and lumbrical muscles
axis of rotation
flexor digitorum profundus
flexor digitorum superficialis
vincula brevia
vincula longa
dorsal extensor expansion
lumbrical
extensor
digitorum
interosseous
third metacarpal
extensor digitorum
third metacarpal
interosseous
flexor digitorum profundus
flexor digitorum superficialis
lumbrical