418
CHAPTER 9
The Upper Limb
fo
glenoid
ateral
la
r
dial
rib
fir
acoid proces
ity
uberos
t
greater
hum erus
head of
acrom ion
cor
s
clavicle
st
m e
borde of scapu
l
border of scapula
ssa
anatom
l
surgica neck
ic neck
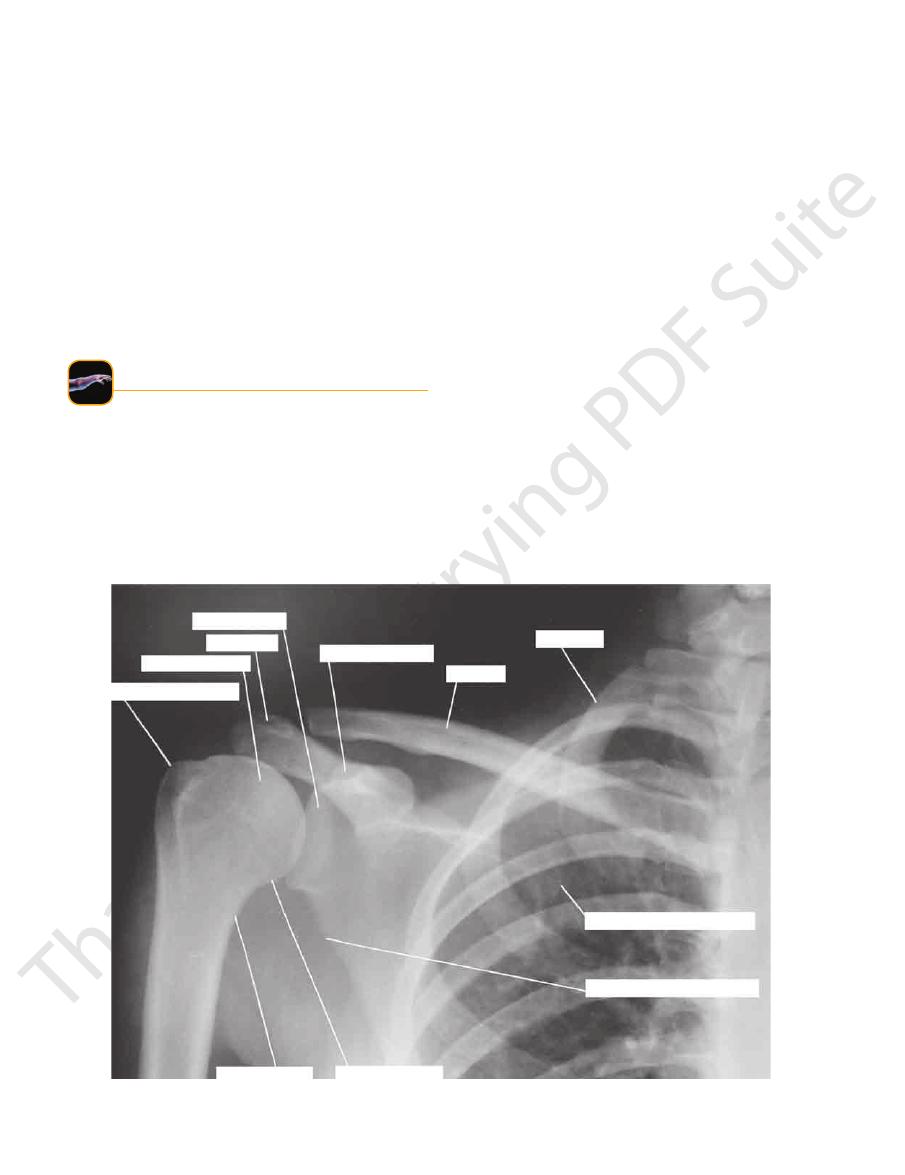
FIGURE 9.86
Anteroposterior radiograph of the shoulder region in the adult.
natomy
aphic
adiog
R
R
a
Radiographic Appearances of the
(Fig. 9.94).
useful to demonstrate the soft tissues around the bones
Magnetic resonance imaging of the upper limb can be
Figures 9.86 through 9.93.
radiographic appearances of the upper limb are shown in
dons, and nerves blend into a homogeneous mass. The
mainly on the bony structures because the muscles, ten
Radiologic examination of the upper limb concentrates
Upper Limb
-
natomy
face
s
uR
a
Anterior Surface of the Chest
projects above the margin of the manubrium sterni.
easily identified. Note that the medial end of the clavicle
of the sternoclavicular and acromioclavicular joints can be
easily palpated (Figs. 9.95, 9.96, and 9.97). The positions
out its entire length lies just beneath the skin and can be
The clavicle is situated at the root of the neck and through
9.96, and 9.97).
ribs and the ends of the 11th and 12th cartilages (Figs. 9.95,
is formed by the cartilages of the 7th, 8th, 9th, and 10th
The costal margin is the lower boundary of the thorax and
sternum and the body of the sternum (Fig. 9.97).
The xiphisternal joint is between the xiphoid process of the
costal cartilage joins the lateral margin of the sternum.
the body of the sternum (Fig. 9.95); at this level, the 2nd
The sternal angle is the angle between the manubrium and
medial ends of the clavicles in the midline (Figs. 9.95 and 9.96).
brium sterni and is easily palpated between the prominent
The suprasternal notch is the superior margin of the manu
Suprasternal Notch
-
Sternal Angle (Angle of Louis)
Xiphisternal Joint
Costal Margin
Clavicle
-

Surface Anatomy
is formed by the lower margin
anterior axillary fold
The
and deltoid muscles (Figs. 9.95 and 9.96).
third of the clavicle and is bounded by the pectoralis major
This small, triangular depression is situated below the outer
Deltopectoral Triangle
column) and counting down from there.
sternal angle and the 2nd costal cartilage (see previous
(Fig. 9.97). Each rib can be identified by first palpating the
them downward over the lateral surface of the chest wall
pressing the fingers upward into the axilla and drawing
The lateral surfaces of the remaining ribs can be felt by
The 1st rib lies deep to the clavicle and cannot be palpated.
419
Ribs
Axillary Folds
of the pectoralis major muscle and can be palpated between
and the pectoral muscles relaxed. With the arm by the side,
The axilla should be examined with the forearm supported
be easily palpated between the finger and thumb (Fig. 9.98).
around the lower border of the teres major muscle. It can
is formed by the tendon of latissimus dorsi as it passes
fold
posterior axillary
her hand against the ipsilateral hip. The
be made to stand out by asking the patient to press his or
the finger and thumb (Figs. 9.95, 9.96, and 9.97). This can
Axilla
humerus
lateral epicondyle
capitulum
radial fossa
neck
head
bicipital tuberosity
ulna
radius
coronoid process
trochlea
medial epicondyle
olecranon fossa
FIGURE 9.87
Anteroposterior radiograph of the elbow region in the adult.
Surface Anatomy
423
flexor
pollicis
longus
flexor
digitorum
profundus
ulna
brachioradialis
radius
basilic
vein
extensor
carpi
ulnaris
cephalic
vein
interosseous
membrane
radial artery and
superficial branch
of radial nerve
anterior median vein
of forearm
flexor
carpi
radialis
flexor
digitorum
superficialis
extensor
pollicis
longus
median nerve
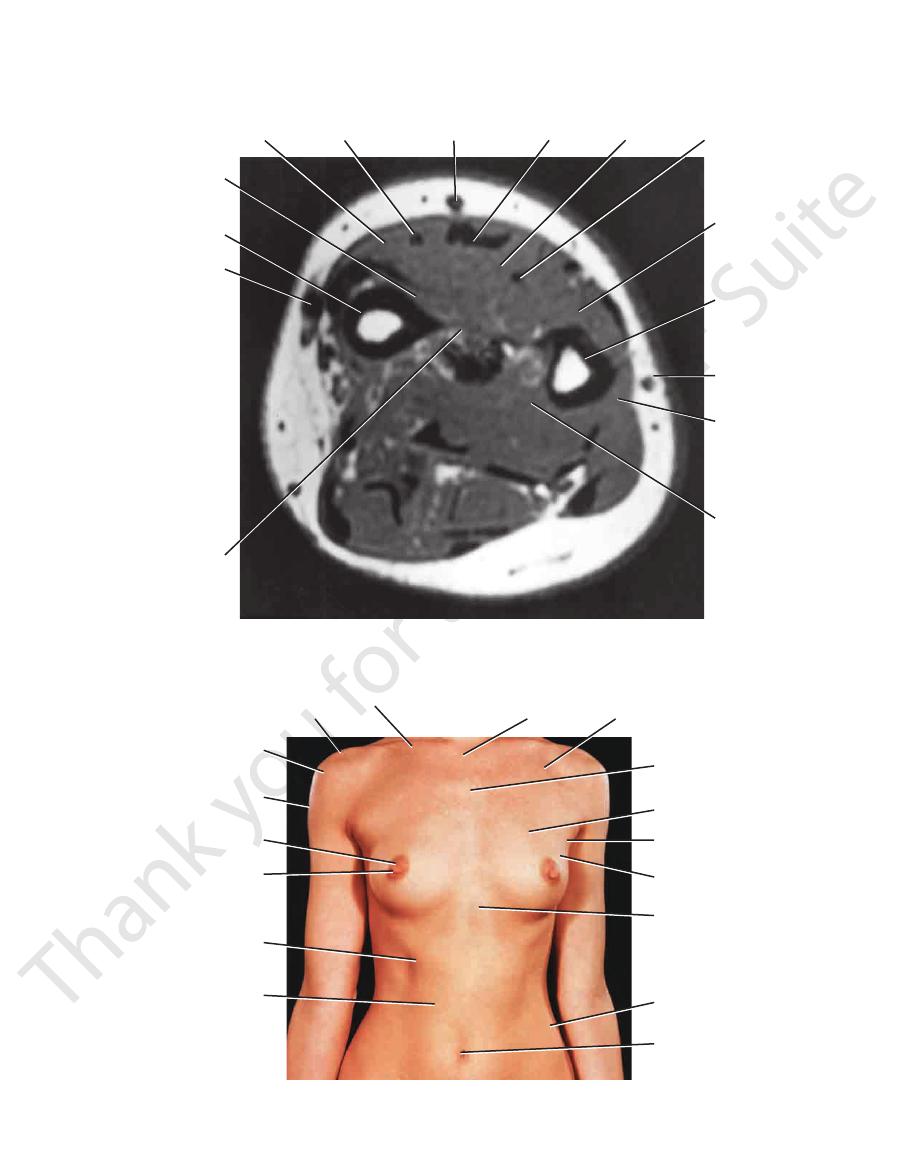
FIGURE 9.94
Transverse (axial) magnetic resonance image of the upper part of the right forearm (as seen from below).
clavicle
acromion process
greater tuberosity
of humerus
deltoid
areola
nipple
costal margin
rectus abdominis
umbilicus
iliac crest
xiphoid process
axillary tail
of mammary gland
anterior
axillary fold
pectoralis major
sternal angle
(angle of Louis)
deltopectoral triangle
suprasternal
notch
FIGURE 9.95
Anterior view of the thorax and abdomen in a 29-year-old woman.
424
CHAPTER 9
The Upper Limb
deltoid
greater
tuberosity
of humerus
acromion
deltopectoral
triangle
trapezius
suprasternal
notch
sternocleidomastoid
supraclavicular
fossa
clavicle
clavicular head
of pectoralis major
sternocostal head
of pectoralis major
biceps
brachii
triceps
anterior
axillary fold
costal margin
rectus
abdominis
origin
of serratus
anterior
median
cubital
vein
cubital fossa
lateral
epicondyle
of humerus
xiphoid
process
medial
epicondyle
of humerus
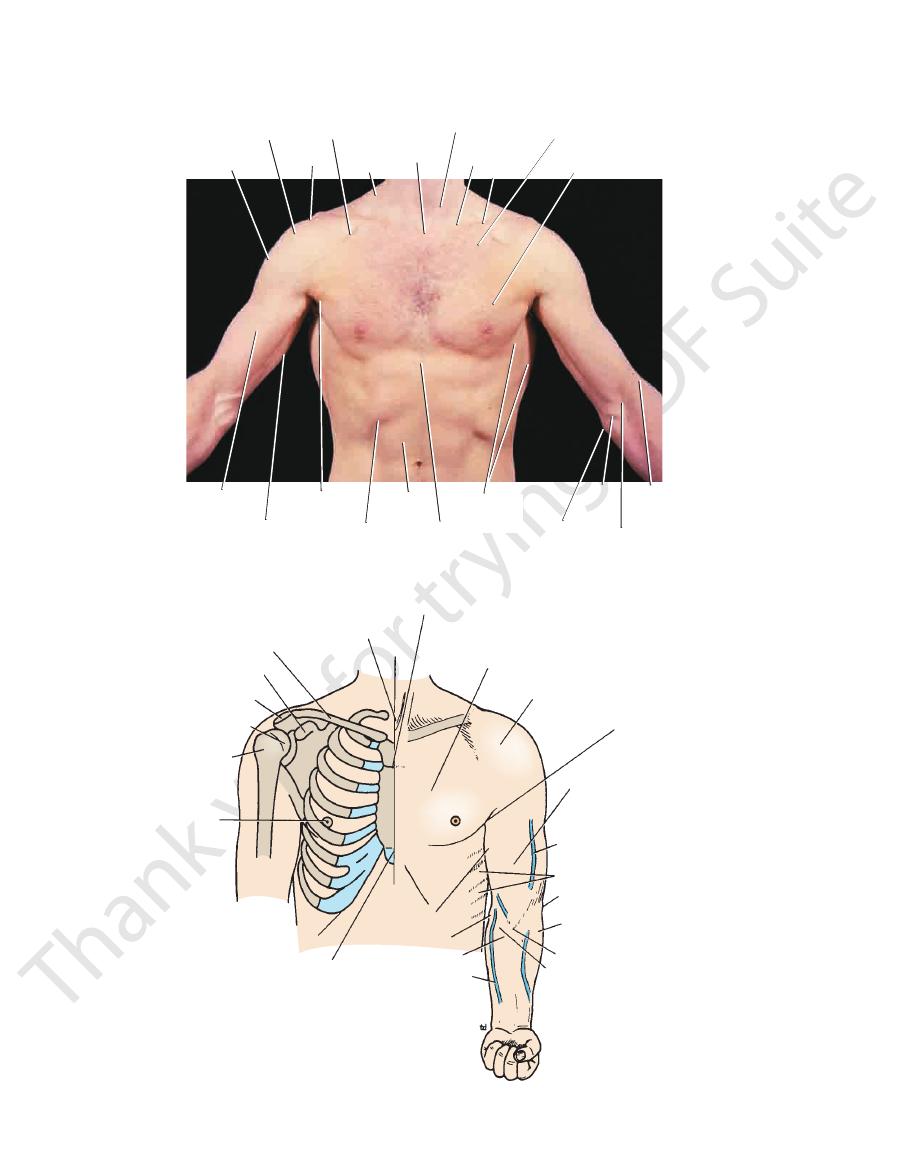
FIGURE 9.96
The pectoral region in a 27-year-old man.
sternal angle
pectoralis major
deltoid
anterior axillary fold
biceps
cephalic vein
serratus anterior
lateral epicondyle
brachioradialis
biceps tendon
bicipital aponeurosis
basilic vein
cubital fossa
medial epicondyle
coracobrachialis
xiphoid process
costal margin
nipple
greater
tuberosity
head of humerus
acromion
coracoid process
clavicle
suprasternal notch
1
2
3
4
5
6
7
8
FIGURE 9.97
Surface anatomy of the chest, shoulder, and upper limb as seen anteriorly.
Surface Anatomy
located (Figs. 9.95 and 9.96).
of the spine of the scapula. It is subcutaneous and easily
forms the lateral extremity
acromion
deltoid muscle. The
topectoral triangle; it is covered by the anterior fibers of the
can be felt on deep palpation in the lateral part of the del
of the scapula (Fig. 9.97)
coracoid process
The tip of the
ligamentum nuchae.
cervical vertebrae are covered by the large ligament called
of the thoracic vertebrae. The spines of the 1st through 6th
Below this level are the overlapping spines
bra prominens).
(verte
process to be felt is that of the 7th cervical vertebra
drawn downward in the nuchal groove. The first spinous
skin in the midline on the posterior surface of the neck and
riorly (Fig. 9.98). The index finger should be placed on the
The spinous processes can be palpated in the midline poste
Thoracic Vertebrae
the humerus.
and the bicipital groove of
biceps brachii muscles
coracobrachia
(Fig. 9.96). The lateral wall is formed by the
tions of which can be seen and felt in a muscular subject
the serra
serratus anterior muscle,
covered by the
ribs
upper
The medial wall of the axilla is formed by the
cords of the brachial
around the artery can be palpated the
can be felt high up in the axilla, and
axillary artery
of the
ily palpated through the floor of the axilla. The pulsations
can be eas
head of the humerus
the inferior part of the
425
-
plexus.
-
-
lis and
Posterior Surface of the Chest
Spinous Processes of Cervical and
-
-
the
Scapula
-
third
thoracic
spine
seventh
thoracic
spine
posterior
axillary
fold
inferior
angle of
scapula
medial epicondyle
olecranon
process of ulna
lateral
epicondyle
head of humerus
acromion
spine of scapula
superior angle of scapula
greater tuberosity
of humerus
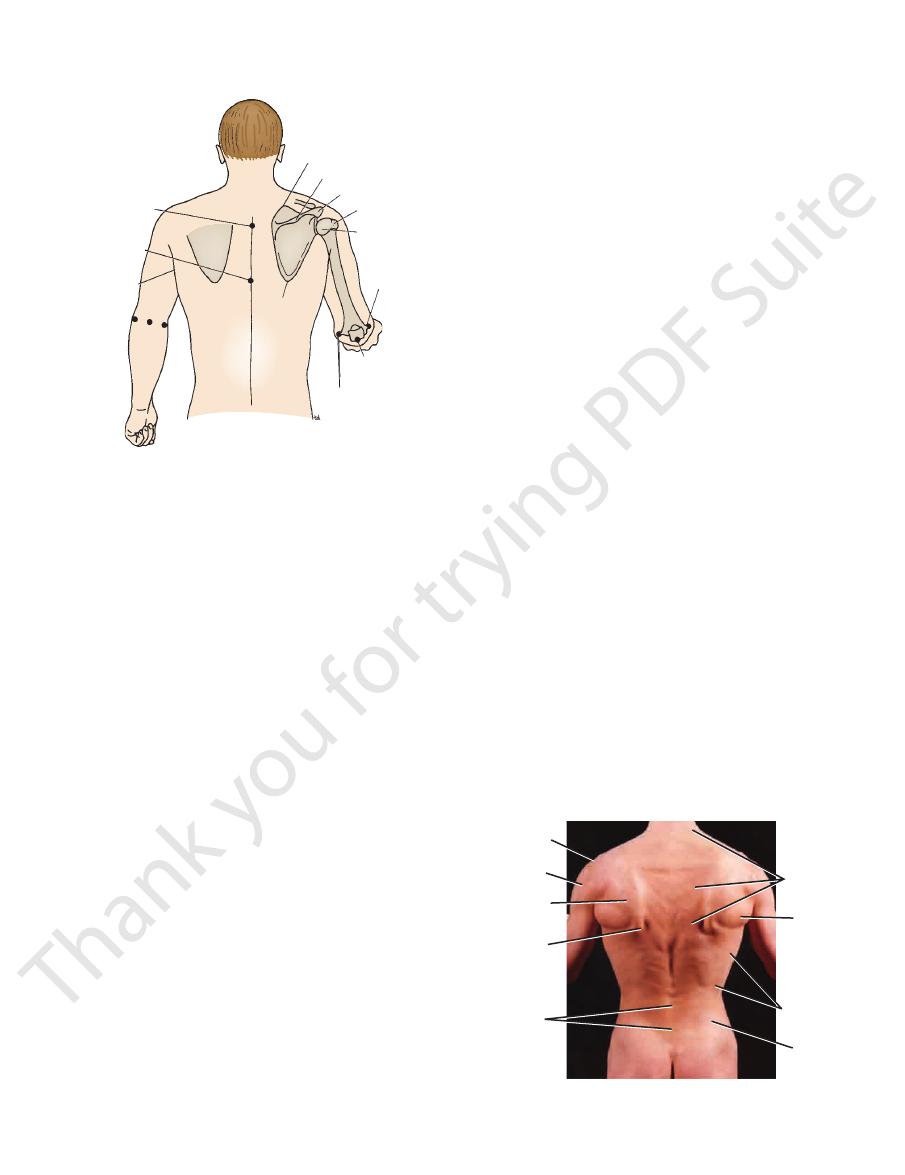
FIGURE 9.98
Surface anatomy of the scapula, shoulder, and
Immediately below the lateral edge of the acromion
elbow regions as seen posteriorly.
is the smooth, rounded curve of the shoulder produced by
traced medially to the medial border of the scapula, which
can be palpated and
crest of the spine of the scapula
The
(Figs. 9.95 and 9.96).
the humerus
greater tuberosity of
which covers the
deltoid muscle,
the
it joins at the level of the 3rd thoracic spine (Fig. 9.98).
becomes darker in color in the second month of the first
(Fig. 9.95). Pink in color in the young girl, the areola
areola
rounded by a circular area of pigmented skin called the
(10 cm) from the midline. The base of the nipple is sur
usually lie over the fourth intercostal spaces about 4 in.
In males and immature females, the nipples are small and
ies greatly and depends on the development of the gland.
(Fig. 9.95), but its position in relation to the chest wall var
projects from the lower half of the breast
nipple
The
ency, produced by its glandular tissue.
open hand, the breast has a firm, overall lobulated consist
contained within it is fluid. On careful palpation with the
In the living subject, the breast is soft because the fat
the breast may be smaller.
breast may be large and pendulous, and in older women
axillary vessels. In middle-aged multiparous women the
(Fig. 9.95), where it comes into close relationship with the
lower border of the pectoralis major and enters the axilla
extends around the
(axillary tail)
Its upper lateral edge
superficial fascia and can be moved freely in all directions.
line (Fig. 9.95). The greater part of the breast lies in the
from the lateral margin of the sternum to the midaxillary
2nd to the 6th ribs and their costal cartilages, and extends
usually hemispherical and slightly pendulous, overlaps the
the pigmented areola. In young women (Fig. 9.95), it is
and the glandular tissue is confined to a small area beneath
In children and men, the breast anatomy is rudimentary
site the 7th thoracic spine (Figs. 9.98 and 9.99).
can be palpated oppo
inferior angle of the scapula
The
the trapezius muscle and lies opposite the 2nd thoracic
can be felt through
superior angle of the scapula
The
spine.
-
The Breast
-
-
-
acromion
deltoid
infraspinatus
inferior angle
of scapula
spinous
processes
of lumbar
vertebrae
trapezius
teres
major
latissimus
dorsi
iliac
crest
FIGURE 9.99
The back in a 27-year-old man.
426
CHAPTER 9
The Upper Limb
pregnancy and never regains its former tint. Tiny
cles
tuber
The “anatomic snuffbox” is an important area. It is a skin
Anatomic Snuffbox
Lateral Side of the Wrist
Important Structures Lying on the
(Fig. 9.100).
The ulnar nerve lies immediately medial to the ulnar artery
Ulnar Nerve
tendon of flexor carpi ulnaris (Fig. 9.100).
The pulsations of the ulnar artery can be felt lateral to the
Ulnar Artery
fixing and stabilizing the wrist joint).
patient to clench the fist (the muscle contracts to assist in
9.100). The tendon can be made prominent by asking the
distally to its insertion on the pisiform bone (Figs. 9.48 and
placed tendon on the front of the wrist and can be followed
The tendon of the flexor carpi ulnaris is the most medially
Tendon of Flexor Carpi Ulnaris
fingers are flexed and extended.
longus and can be seen moving beneath the skin when the
group of four that lie medial to the tendon of palmaris
The tendons of the flexor digitorum superficialis are a
Tendons of Flexor Digitorum Superficialis
(Fig. 9.100).
don of flexor carpi radialis and overlies the median nerve
The tendon of the palmaris longus lies medial to the ten
Tendon of Palmaris Longus (If Present)
pulsating radial artery.
The tendon of the flexor carpi radialis lies medial to the
Tendon of Flexor Carpi Radialis
of flexor carpi radialis muscle.
it lies just beneath the skin and fascia lateral to the tendon
to the distal third of the radius (Figs. 9.48 and 9.100). Here,
The pulsations of the radial artery can easily be felt anterior
Radial Artery
the Wrist
Important Structures Lying in Front of
flexor retinaculum.
transverse crease corresponds to the proximal border of the
verse crease lies at the level of the wrist joint. The distal
important landmarks (Fig. 9.100). The proximal trans
seen in front of the wrist are
transverse creases
The
a fingerbreadth distal and lateral to the pisiform bone.
can be felt on deep palpation of the hypothenar eminence,
hook of the hamate bone
creases (Figs. 9.48 and 9.100). The
the anterior aspect of the wrist between the two transverse
can be felt on the medial side of
pisiform bone
The
distinguished from the more distal pointed styloid process.
eral side of the wrist (Fig. 9.75). The rounded head can be
pronated; the head then stands out prominently on the lat
is most easily felt with the forearm
head of the ulna
The
terior surface of the distal end of the radius (Fig. 9.100).
is palpable on the pos
dorsal tubercle of the radius
The
lies about 0.75 in. (1.9 cm) distal to that of the ulna.
can be palpated. The styloid process of the radius
(Fig. 9.100)
styloid processes of the radius
At the wrist, the
The Wrist and Hand
and can be palpated along its entire length.
is subcutaneous
posterior border of the ulna bone
The
radius, it divides into the radial and ulnar arteries.
tal aponeurosis, and, at a level just below the head of the
biceps muscle. In the cubital fossa, it lies beneath the bicipi
down the arm, overlapped by the medial border of the
can be felt to pulsate as it passes
brachial artery
The
sation is felt along the medial part of the hand.
cord, and when it is compressed, a “pins and needles” sen
medial epicondyle of the humerus. It feels like a rounded
can be palpated where it lies behind the
ulnar nerve
The
joint is flexed against resistance.
The tendon and aponeurosis are most easily felt if the elbow
cia on the medial side of the forearm (Figs. 9.48 and 9.97).
can be felt as it leaves the tendon to join the deep fas
rosis
bicipital aponeu
passes downward into the fossa, and the
can be palpated as it
tendon of the biceps muscle
ary. The
boundary and the pronator teres forms the medial bound
seen and felt; the brachioradialis muscle forms the lateral
elbow (Figs. 9.48 and 9.97), and the boundaries can be
is a skin depression in front of the
cubital fossa
The
forearm.
be felt to rotate during pronation and supination of the
distal to the lateral epicondyle. The head of the radius can
sion on the posterolateral aspect of the extended elbow,
can be palpated in a depres
head of the radius
The
an equilateral triangle.
elbow is flexed, these three points form the boundaries of
these bony points lie on the same straight line; when the
be palpated (Fig. 9.98). When the elbow joint is extended,
9.96 and 9.98) and the olecranon process of the ulna can
of the humerus (Figs.
lateral epicondyles
medial
The
glands.
areolar
on the areola are produced by the underlying
The Elbow Region
and
-
-
-
-
-
-
and ulna
-
-
-
-
box as it ascends the forearm.
can also sometimes be recognized crossing the snuff
vein
cephalic
to reach the dorsum of the hand (Fig. 9.100). The
as the artery winds around the lateral margin of the wrist
can be palpated within the snuffbox
radial artery
ble). The
(felt but not identifia
trapezium
scaphoid
the thumb (distally); between these bones beneath the floor
of
base of the first metacarpal bone
(proximally) and the
styloid process of the radius
its floor can be palpated the
(Fig. 9.100). In
extensor pollicis brevis
pollicis longus
tendons of abductor
and laterally by the
pollicis longus
tendon of extensor
radius. It is bounded medially by the
depression that lies distal to the styloid process of the
and
lie the
and the
-
-
Surface Anatomy
427
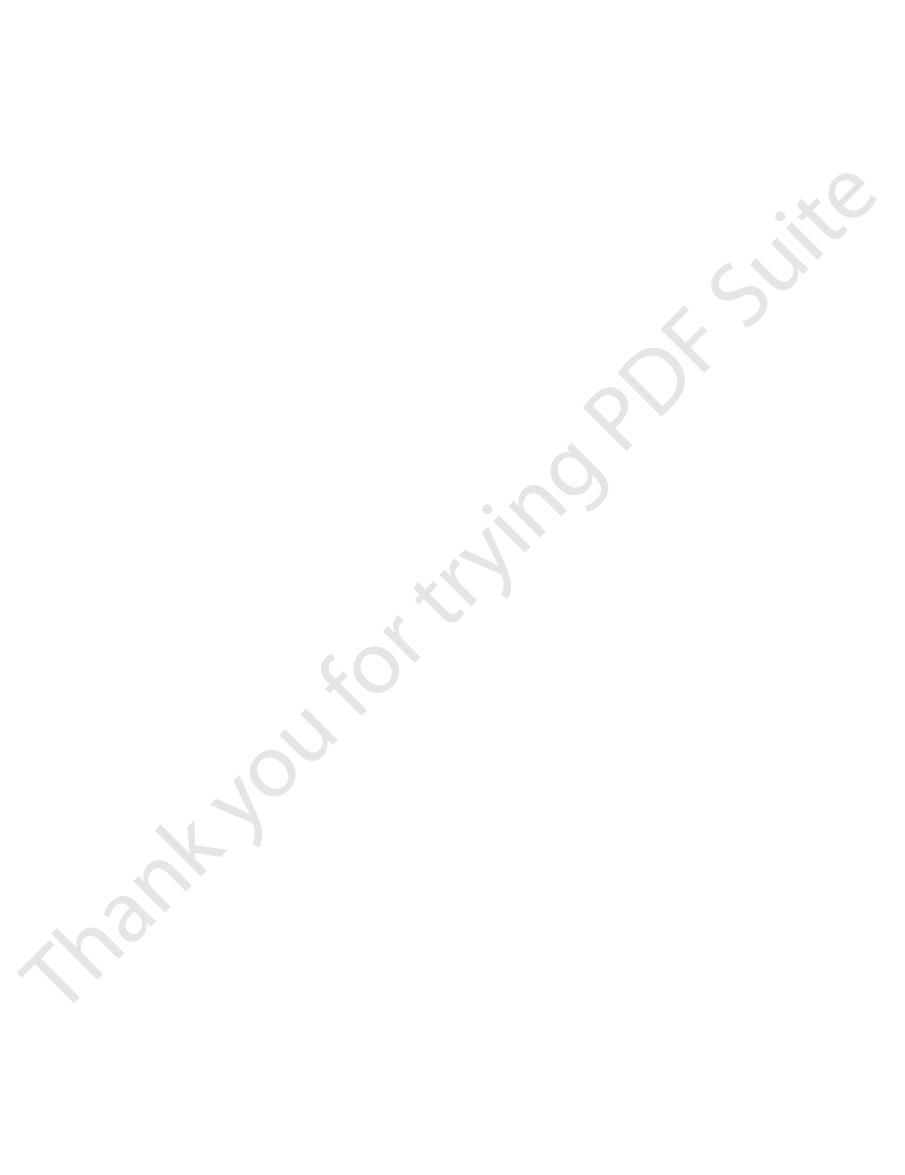
superficial
palmar arch
deep palmar arch
hook of hamate
deep branch of ulnar artery
ulnar nerve
distal transverse crease
pisiform bone
proximal transverse crease
flexor carpi ulnaris
ulnar artery
palmaris longus
median nerve
dorsal tubercle of radius
superficial palmar branch
flexor carpi radialis
radial artery
tubercle of scaphoid
ridge of trapezium
of radial artery
A
base of first metacarpal
trapezium
scaphoid
styloid process of radius
abductor pollicis longus
extensor pollicis brevis
cephalic vein
extensor pollicis
longus
extensor indicis
radial artery
extensor digitorum
extensor digiti minimi
dorsal venous network
B
extensor retinaculum
flexor retinaculum
FIGURE 9.100
Surface anatomy of the wrist region.
428
CHAPTER 9
pass distally to the bases of the fingers (Fig. 9.100).
can be seen and felt as they
extensor digiti minimi
extensor indicis,
tendons of extensor digitorum,
The
Important Structures Lying on the
finger creases.
lie at the level of the middle and distal
phalangeal joints
inter
level of the distal transverse palmar crease. The
The metacarpophalangeal joints lie approximately at the
Metacarpophalangeal Joints
extended thumb.
the palm at the level of the proximal border of the fully
part of the palm (Fig. 9.100) and lies on a line drawn across
The deep palmar arterial arch is also located in the central
Deep Palmar Arterial Arch
extended thumb.
across the palm at the level of the distal border of the fully
tral part of the palm (Fig. 9.100) and lies on a line drawn
The superficial palmar arterial arch is located in the cen
Superficial Palmar Arterial Arch
of the scaphoid (Fig. 9.62).
ulum and lies about one fingerbreadth distal to the tubercle
nence curves around the lower border of the flexor retinac
The recurrent branch to the muscles of the thenar emi
Recurrent Branch of the Median Nerve
Important Structures Lying in the Palm
when the wrist joint is flexed.
be palpated just distal to the dorsal tubercle of the radius
The lunate lies in the proximal row of carpal bones. It can
Lunate
of the Wrist
Important Structures Lying on the Back
The Upper Limb
-
-
-
-
Dorsum of the Hand
the
and the
Arterial Injury
are distributed to the arteries within the branches of the plexus.
the 2nd to 8th thoracic segments of the spinal cord. They ascend
nerves. The preganglionic fibers originate from cell bodies in
ing of the fists closes off the superficial and deep palmar arterial
press the radial arteries against the anterior surface of each
nerve. The artery is commonly damaged here in laceration
artery on the other wrist; occasionally, a congenitally abnormal
carpi radialis; it is here that the clinician takes the radial pulse
artery, as it crosses the first rib to become the axillary artery, can
be palpated or compressed in an emergency. The subclavian
lateral circulation are not diseased and the patient’s general cir
gangrene, provided, of course, that the arteries forming the col
ing wounds or may require ligation in amputation operations.
The arteries of the upper limb can be damaged by penetrat-
Because of the existence of an adequate collateral circulation
around the shoulder, elbow, and wrist joints, ligation of the main
arteries of the upper limb is not followed by tissue necrosis or
-
-
culation is satisfactory. Nevertheless, it can take days or weeks
for the collateral vessels to open sufficiently to provide the distal
part of the limb with the same volume of blood as previously sup-
plied by the main artery.
Palpation and Compression of Arteries
A clinician must know where the arteries of the upper limb can
be palpated in the root of the posterior triangle of the neck (Fig.
9.31). The artery can be compressed here against the first rib to
stop a catastrophic hemorrhage. The third part of the axillary
artery can be felt in the axilla as it lies in front of the teres major
muscle (Fig. 9.17). The brachial artery can be palpated in the arm
as it lies on the brachialis and is overlapped from the lateral side
by the biceps brachii (Fig. 9.43).
The radial artery lies superficially in front of the distal end of
the radius, between the tendons of the brachioradialis and flexor
(Fig. 9.58). If the pulse cannot be felt, try feeling for the radial
radial artery can be difficult to feel. The radial artery can be less
easily felt as it crosses the anatomic snuffbox (Fig. 9.100).
The ulnar artery can be palpated as it crosses anterior to the
flexor retinaculum in company with the ulnar nerve. The artery
lies lateral to the pisiform bone, separated from it by the ulnar
wounds in front of the wrist.
Allen Test
The Allen test is used to determine the patency of the ulnar and
radial arteries. With the patient’s hands resting in the lap, com-
radius and ask the patient to tightly clench the fists. The clench-
arches. When the patient is asked to open the hands, the skin of
the palms is at first white, and then normally the blood quickly
flows into the arches through the ulnar arteries, causing the
palms to promptly turn pink. This establishes that the ulnar arter-
ies are patent. The patency of the radial arteries can be estab-
lished by repeating the test but this time compressing the ulnar
arteries as they lie lateral to the pisiform bones.
Arterial Innervation and Raynaud’s Disease
The arteries of the upper limb are innervated by sympathetic
in the sympathetic trunk and synapse in the middle cervical,
inferior cervical, 1st thoracic, or stellate ganglia. The postgan-
glionic fibers join the nerves that form the brachial plexus and
For example, the digital arteries of the fingers are supplied by
postganglionic sympathetic fibers that run in the digital nerves.
Vasospastic diseases involving digital arterioles, such as
Raynaud’s disease, may require a cervicodorsal preganglionic
sympathectomy to prevent necrosis of the fingers. The operation
is followed by arterial vasodilatation, with consequent increased
blood flow to the upper limb.
C L I N I C A L N O T E S O N T H E A R T E R I E S O F T H E U P P E R L I M P
430
CHAPTER 9
The Upper Limb
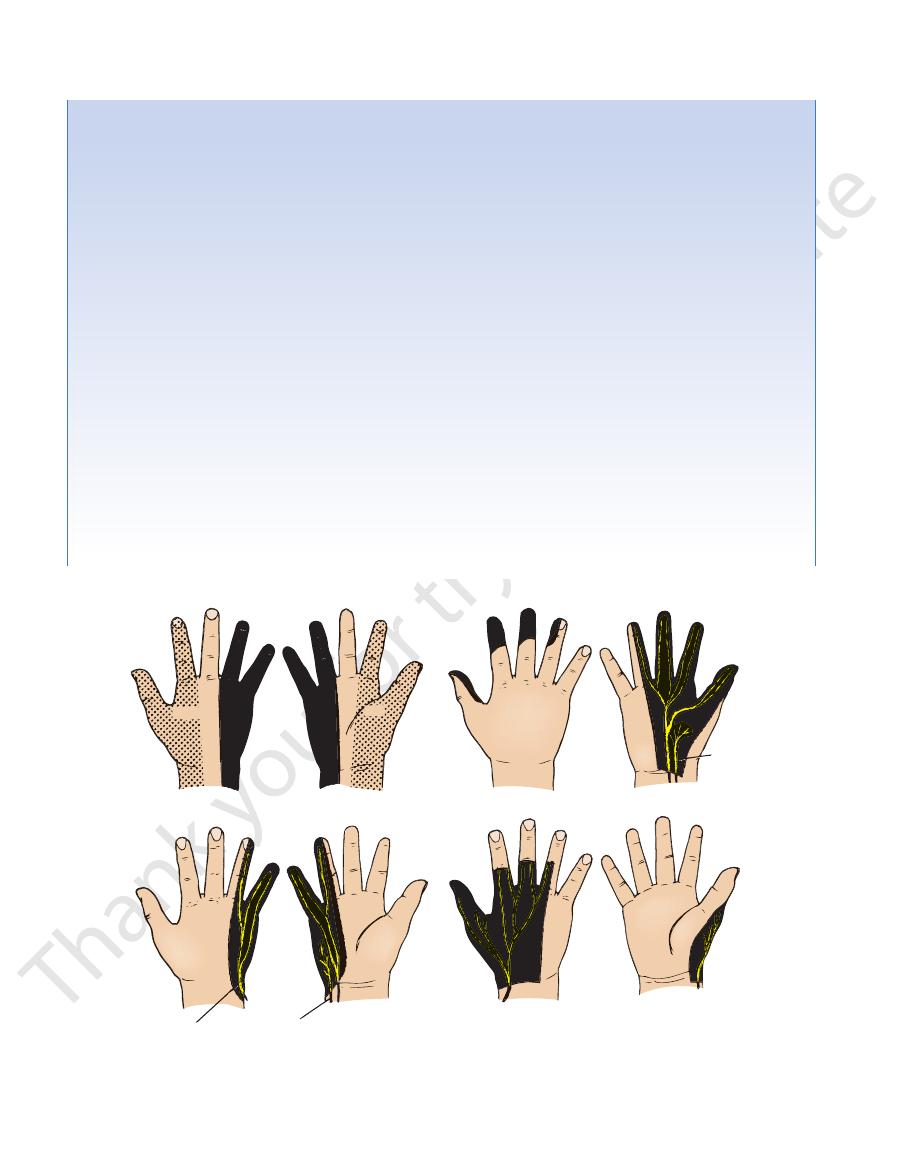
dermatomes
median nerve
palmar cutaneous
radial nerve
posterior cutaneous branch
palmar
cutaneous
branch
ulnar nerve
C6 C7
C8
C8
C7
C6
FIGURE 9.102
Sensory innervation of the skin of the volar (palmar) and dorsal aspects of the hand; the arrangement of the
dermatomes is also shown.
and will protrude posteriorly, a condition known as
surface of the medial one and a half fingers; the exact cutaneous
branch supplies the extensor carpi radialis brevis and the supi
nerve and continues as the superficial radial nerve. The deep
dyle, it gives off three branches: the nerve to a small part of the
the lateral head of the triceps; and the nerve to the medial head
movement is much impaired. Paralysis of the teres minor is not
der dislocations or fractures of the surgical neck of the humerus.
cord of the brachial plexus (C5 and 6), can be injured by the pres
“winged
scapula” (Fig. 9.8).
Axillary Nerve
The axillary nerve (Fig. 9.24), which arises from the posterior
-
sure of a badly adjusted crutch pressing upward into the arm-
pit. The passage of the axillary nerve backward from the axilla
through the quadrangular space makes it particularly vulnerable
here to downward displacement of the humeral head in shoul-
Paralysis of the deltoid and teres minor muscles results. The
cutaneous branches of the axillary nerve, including the upper
lateral cutaneous nerve of the arm, are functionless, and con-
sequently there is a loss of skin sensation over the lower half of
the deltoid muscle. The paralyzed deltoid wastes rapidly, and the
underlying greater tuberosity can be readily palpated. Because
the supraspinatus is the only other abductor of the shoulder, this
recognizable clinically.
Radial Nerve
The radial nerve (Fig. 9.25), which arises from the posterior cord
of the brachial plexus, characteristically gives off its branches
some distance proximal to the part to be innervated.
In the axilla, it gives off three branches: the posterior cutaneous
nerve of the arm, which supplies the skin on the back of the arm
down to the elbow; the nerve to the long head of the triceps; and
the nerve to the medial head of the triceps.
In the spiral groove of the humerus, it gives off four branches:
the lower lateral cutaneous nerve of the arm, which supplies the
lateral surface of the arm down to the elbow; the posterior cuta-
neous nerve of the forearm, which supplies the skin down the
middle of the back of the forearm as far as the wrist; the nerve to
of the triceps and the anconeus.
In the anterior compartment of the arm above the lateral epicon-
brachialis, the nerve to the brachioradialis, and the nerve to the
extensor carpi radialis longus.
In the cubital fossa, it gives off the deep branch of the radial
-
nator in the cubital fossa and all the extensor muscles in the pos-
terior compartment of the forearm. The superficial radial nerve is
sensory and supplies the skin over the lateral part of the dorsum
of the hand and the dorsal surface of the lateral three and a half
fingers proximal to the nail beds (Fig. 9.102). (The ulnar nerve
supplies the medial part of the dorsum of the hand and the dorsal
areas innervated by the radial and ulnar nerves on the hand are
subject to variation.)
The radial nerve is commonly damaged in the axilla and in the
spiral groove.
(continued)
434
CHAPTER 9
basilic veins) links the cephalic and basilic veins in the
(or median cephalic and median
median cubital vein
The
pierces the deep fascia at about the middle of the arm.
the anterior aspect just below the elbow (Fig. 9.39). It
hand around the medial side of the forearm and reaches
can be traced from the dorsum of the
basilic vein
The
in the deltopectoral triangle and enters the axillary vein.
of the biceps (Fig. 9.39). It ends by piercing the deep fascia
then ascends into the arm and runs along the lateral border
winds around onto the anterior aspect of the forearm. It
crosses the anatomic snuffbox and
cephalic vein
The
the lateral cephalic vein and a medial basilic vein.
of the hand (Fig. 9.100). The network drains upward into
The network of superficial veins can be seen on the dorsum
Dorsal Venous Network
The Upper Limb
cubital fossa (Fig. 9.39).
this means, the veins become distended with blood.
the upper arm and repeatedly clench and relax the fist. By
To identify these veins easily, apply firm pressure around
www.thePoint.lww.com/Snell9e.
Clinical Cases
and
Review Questions
are available online at
FIGURE 9.105
Ulnar nerve palsy.