Bacteriology
Dr. Donya A Makki Mycobacteria
1
The mycobacteria are rod-shaped, aerobic bacteria that do not form
spores.
Although they do not stain readily, once stained they resist
decolorization by acid or alcohol and are therefore called "acid-fast"
bacilli.
Mycobacterium tuberculosis causes tuberculosis and is a very
important pathogen of humans. Mycobacterium leprae causes leprosy.
Mycobacterium avium-intracellulare and other nontuberculous
mycobacteria frequently infect patients with AIDS, are opportunistic
pathogens in other immunocompromised persons, and occasionally
cause disease in patients with normal immune systems.
There are more than 125 Mycobacterium species, including many that
are saprophytes (a saprophyte is an organism that obtains its
nutrients from non-living organic matter, usually dead and decaying
plant or animal matter).
Bacteriology
Dr. Donya A Makki Mycobacteria
2
A. Typical Organisms
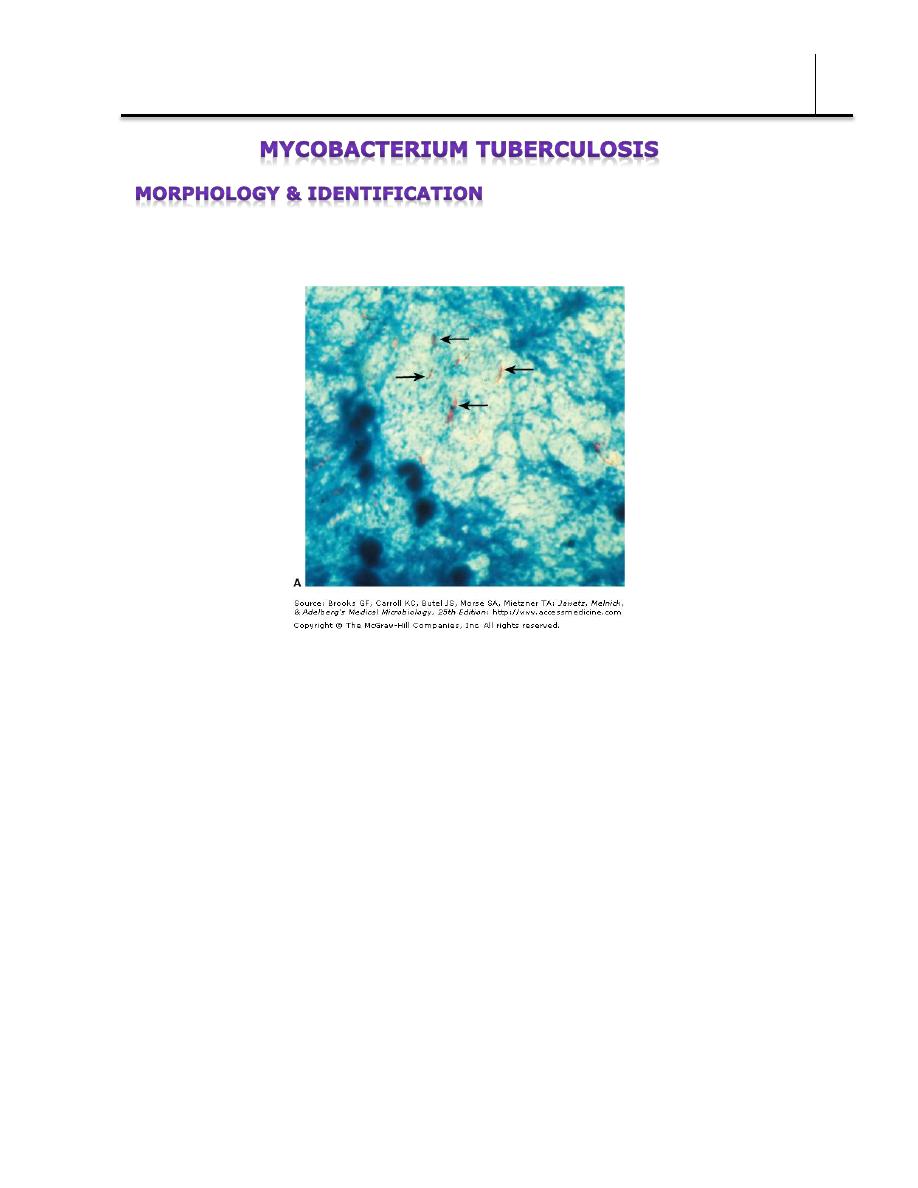
In tissue, tubercle bacilli are thin straight rods measuring 0.4 x 3 µm .
Mycobacterium tuberculosis (arrows) in a processed sputum specimen stained by Ziehl
Neelsen stain. The Mycobacterium tuberculosis is red against a blue background.
On artificial media, coccoid and filamentous forms are seen with
variable morphology from one species to another.
Mycobacteria cannot be classified as either gram-positive or gram-
negative. Once stained by basic dyes they cannot be decolorized by
alcohol. True tubercle bacilli are characterized by "acid-fastness"—ie,
95% ethyl alcohol containing 3% hydrochloric acid (acid-alcohol)
quickly decolorizes all bacteria except the mycobacteria. The Ziehl-
Neelsen technique of staining is employed for identification of acid-fast
bacteria.
Bacteriology
Dr. Donya A Makki Mycobacteria
3
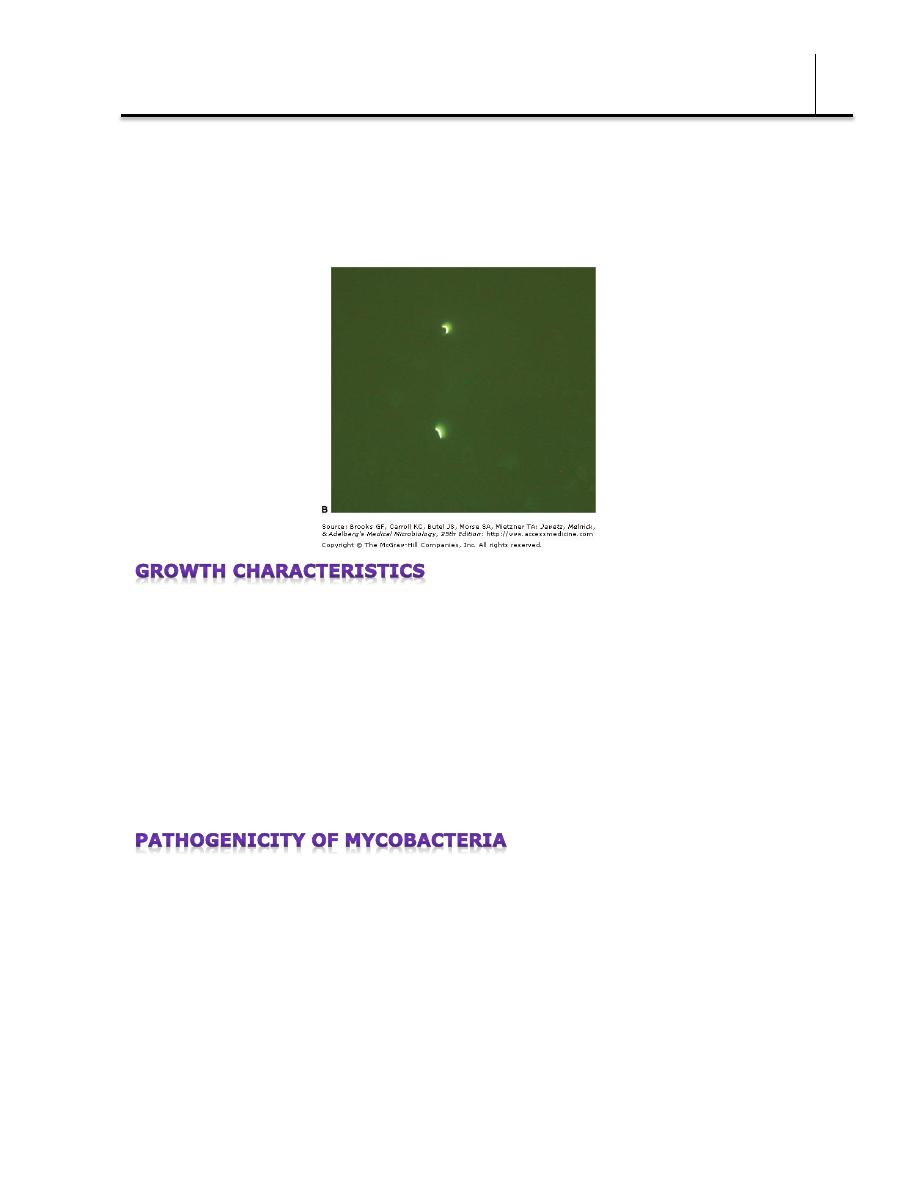
In smears of sputum or sections of tissue, mycobacteria can be
demonstrated by yellow-orange fluorescence after staining with
fluorochrome stains.
Mycobacteria are obligate aerobes (need oxygen) and derive energy
from the oxidation of many simple carbon compounds. Increased CO2
tension enhances growth. The growth rate is much slower than that of
most bacteria. The doubling time of tubercle bacilli is about 18 hours.
Saprophytic forms tend to grow more rapidly, to proliferate well at 22–
33°C, to produce more pigment, and to be less acid-fast than
pathogenic forms.
There are marked differences in the ability of different mycobacteria to
cause lesions in various host species. Humans and guinea pigs are
highly susceptible to M tuberculosis infection, whereas fowl and cattle
are resistant. M tuberculosis and Mycobacterium bovis are equally
pathogenic for humans. The route of infection (respiratory versus
intestinal) determines the pattern of lesions. In developed countries, M
Bacteriology
Dr. Donya A Makki Mycobacteria
4
bovis has become very rare. Some "atypical" mycobacteria, now
designated as nontuberculous (eg, Mycobacterium kansasii) produce
human disease indistinguishable from tuberculosis; others (eg,
Mycobacterium fortuitum) cause only surface lesions or act as
opportunists.
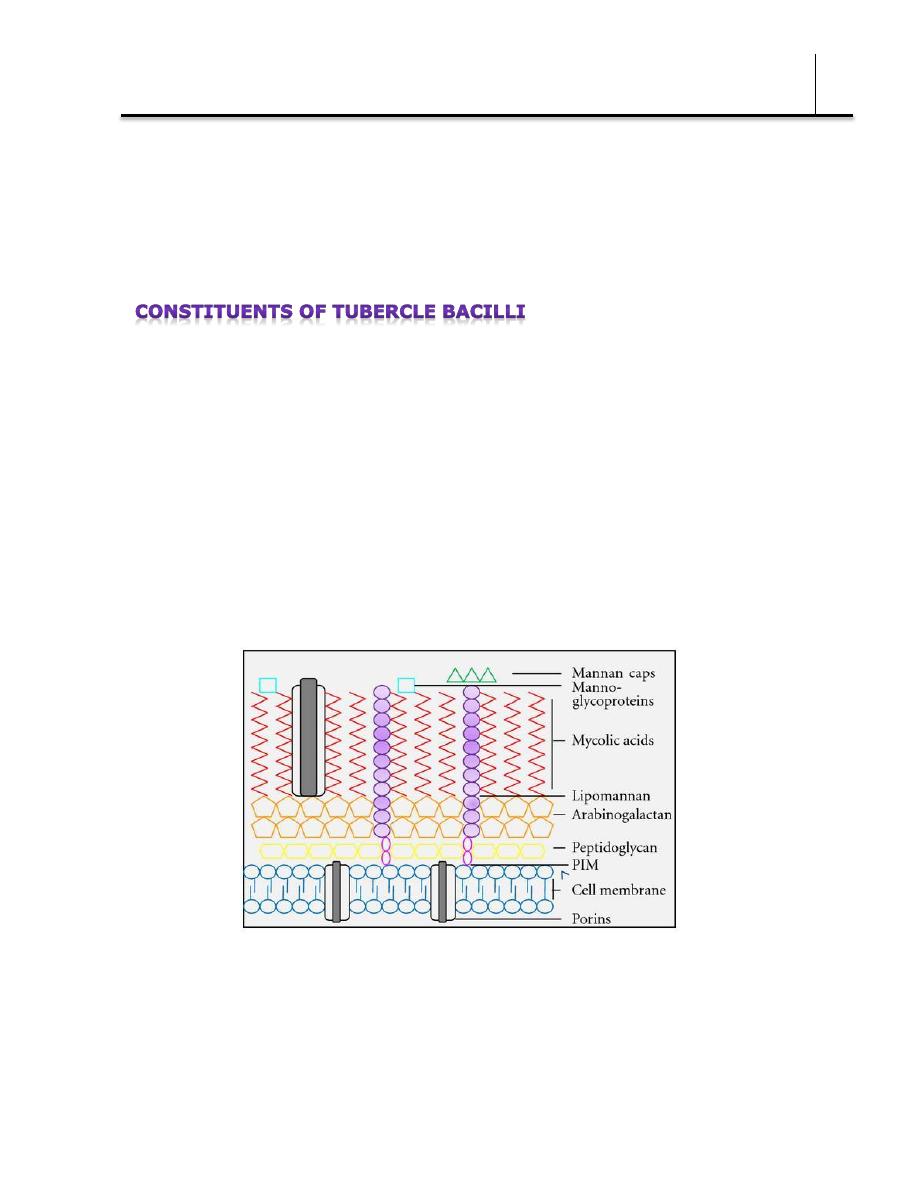
The constituents listed below are found mainly in cell walls.
Mycobacterial cell walls can induce delayed hypersensitivity and some
resistance to infection and can replace whole mycobacterial cells in
Freund's adjuvant. Mycobacterial cell contents only elicit delayed
hypersensitivity reactions in previously sensitized animals.
Lipids
Mycobacteria are rich in lipids. These include mycolic acids (long-chain
fatty acids C78–C90), waxes, and phosphatides. In the cell, the lipids
are largely bound to proteins and polysaccharides.
Muramyl dipeptide (from peptidoglycan) complexed with mycolic acids
can cause granuloma formation; phospholipids induce caseous necrosis
(a form of cell death in which the tissue maintains a cheese-like
appearance). Lipids are to some extent responsible for acid-fastness.
Bacteriology
Dr. Donya A Makki Mycobacteria
5
Their removal with hot acid destroys acid-fastness, which depends on
both the integrity of the cell wall and the presence of certain lipids.
Virulent strains of tubercle bacilli form microscopic "serpentine cords"
in which acid-fast bacilli are arranged in parallel chains.
Cord formation is correlated with virulence. A "cord factor" (trehalose-
6, 6'-dimycolate) has been extracted from virulent bacilli with
petroleum ether. It inhibits migration of leukocytes, causes chronic
granulomas, and can serve as an immunologic "adjuvant."
Proteins
Each type of mycobacterium contains several proteins that elicit the
tuberculin reaction. Proteins bound to a wax fraction can, upon
injection, induce tuberculin sensitivity. They can also elicit the
formation of a variety of antibodies.
Polysaccharides
Mycobacteria contain a variety of polysaccharides. Their role in the
pathogenesis of disease is uncertain. They can induce the immediate
type of hypersensitivity and can serve as antigens in reactions with
sera of infected persons.
Mycobacteria are emitted in droplets <25 µm in diameter when
infected persons cough, sneeze, or speak. The droplets evaporate
Bacteriology
Dr. Donya A Makki Mycobacteria
6
leaving organisms which are small enough, when inhaled, to be
deposited in alveoli.
Once inside the alveoli, the host's immune system responds by release
of cytokines and lymphokines that stimulate monocytes and
macrophages. Mycobacteria begin to multiply within macrophages.
Some of the macrophages develop an enhanced ability to kill the
organism while others may be killed by the bacilli. After 1–2 months
following exposure, pathogenic lesions associated with infection,
appear in the lung. Resistance and hypersensitivity of the host greatly
influence development of disease and the type of lesions that are seen.
The production and development of lesions and their healing or
progression are determined chiefly by (1) the number of mycobacteria
in the inoculum and their subsequent multiplication, and (2) the type
of host.
A. Two Principal Lesions
1. Exudative type—This consists of an acute inflammatory reaction,
with edema fluid, polymorphonuclear leukocytes, and, later,
monocytes around the tubercle bacilli. This type is seen particularly in
lung tissue, where it resembles bacterial pneumonia. It may :
a. heal by resolution, so that the entire exudate becomes absorbed;
b. it may lead to massive necrosis of tissue;
c. or it may develop into the second (productive) type of lesion.
During the exudative phase, the tuberculin test becomes positive.
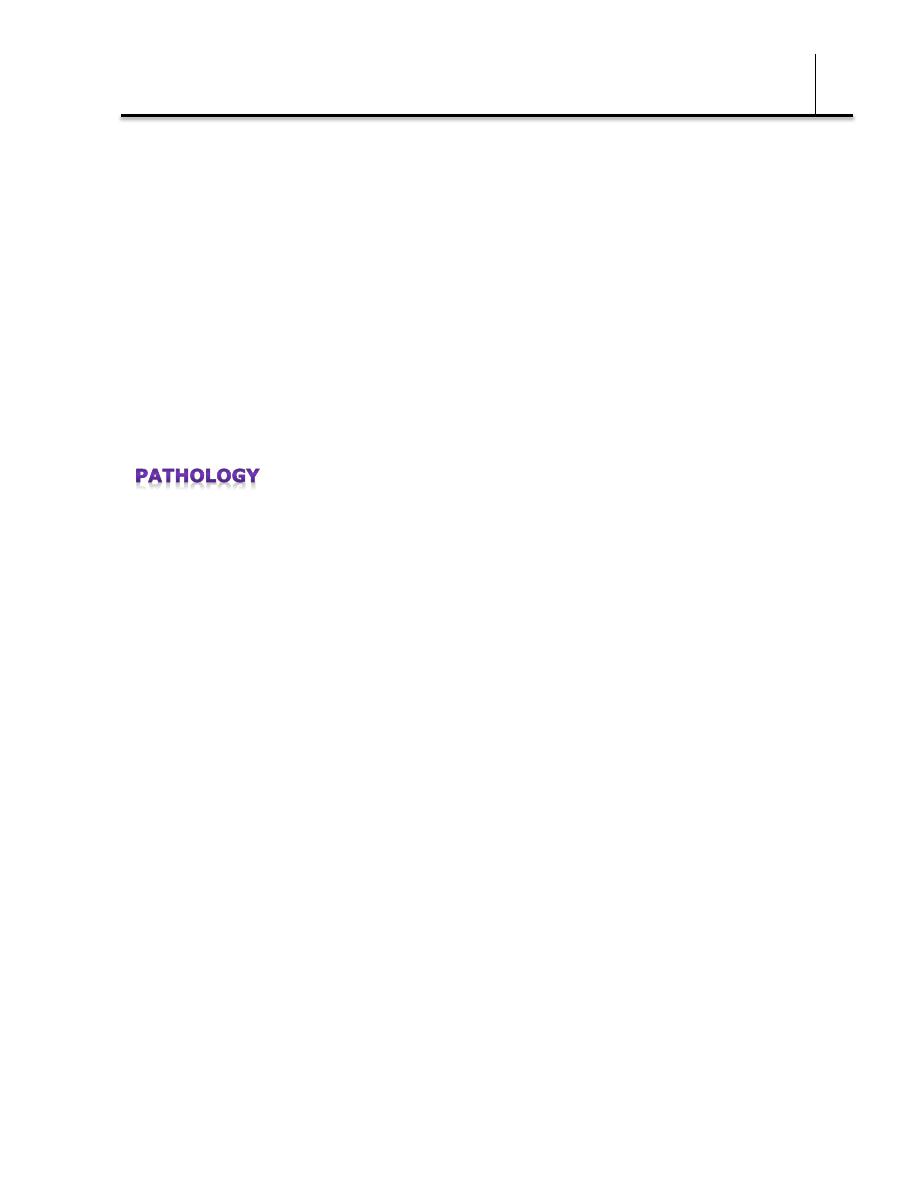
2. Productive type—When fully developed, this lesion, a chronic
granuloma, consists of three zones:
(1) a central area of large, multinucleated giant cells containing
Bacteriology
Dr. Donya A Makki Mycobacteria
7
tubercle bacilli;
(2) a mid zone of pale epithelioid cells, often arranged radially; and
(3) a peripheral zone of fibroblasts, lymphocytes, and monocytes.
Later, peripheral fibrous tissue develops, and the central area
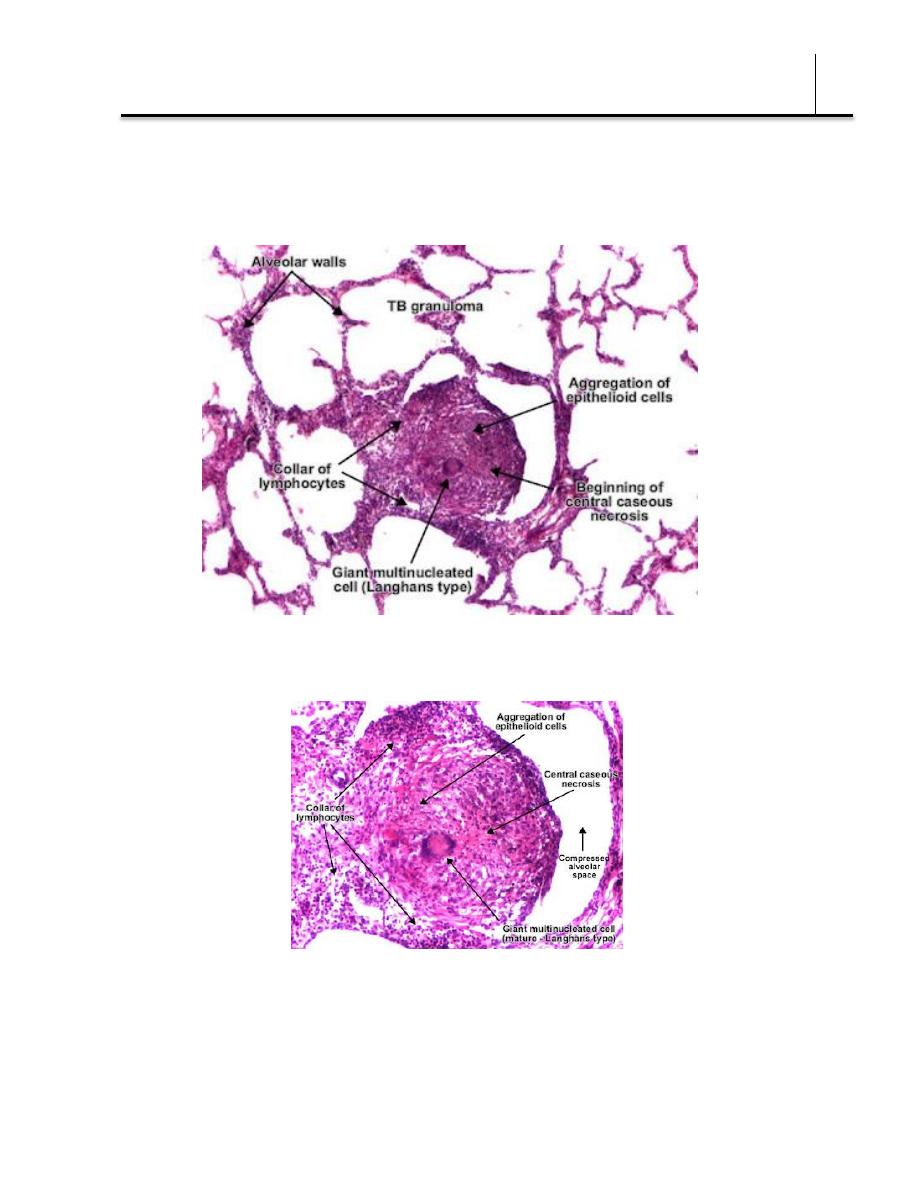
undergoes caseation necrosis. Such a lesion is called a tubercle.
Bacteriology
Dr. Donya A Makki Mycobacteria
8
necrotizing granuloma
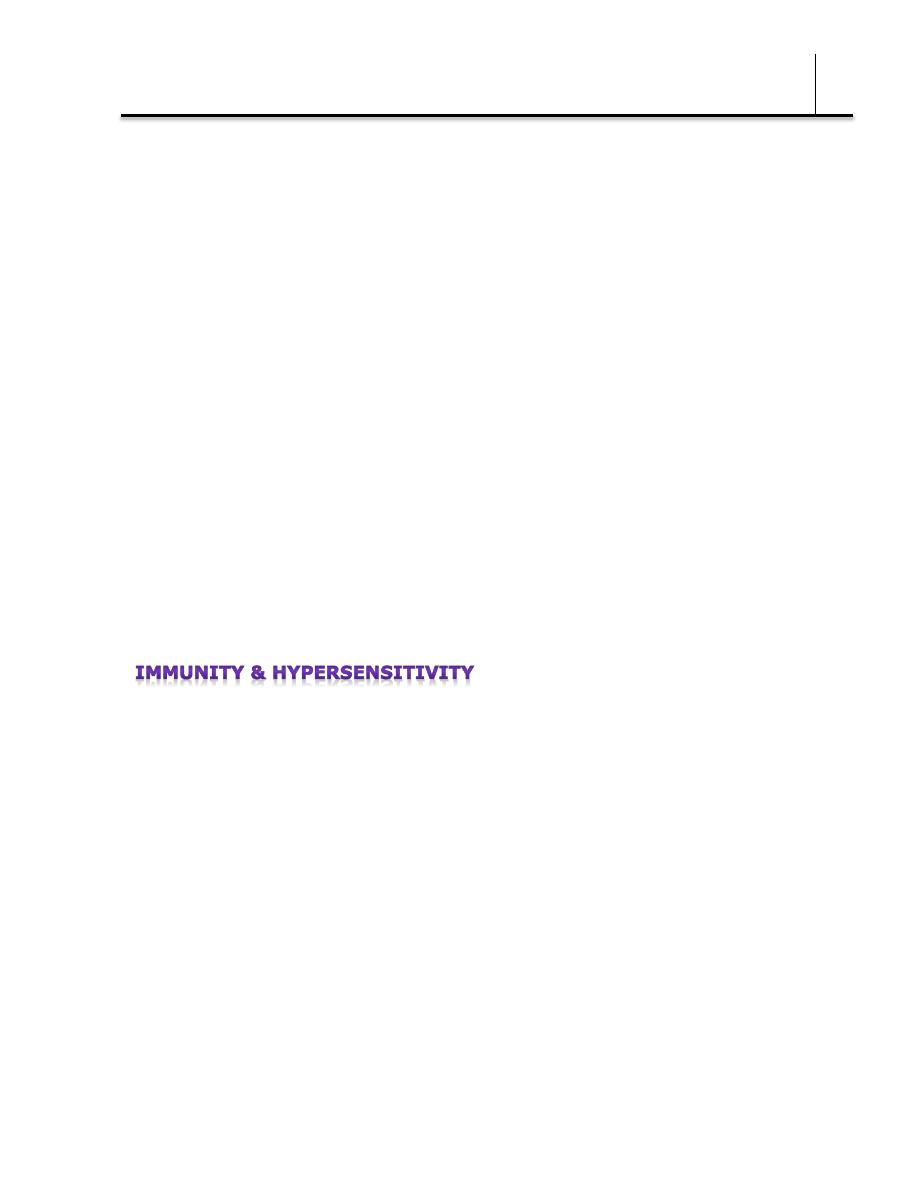
A caseous tubercle may break into a bronchus, empty its contents
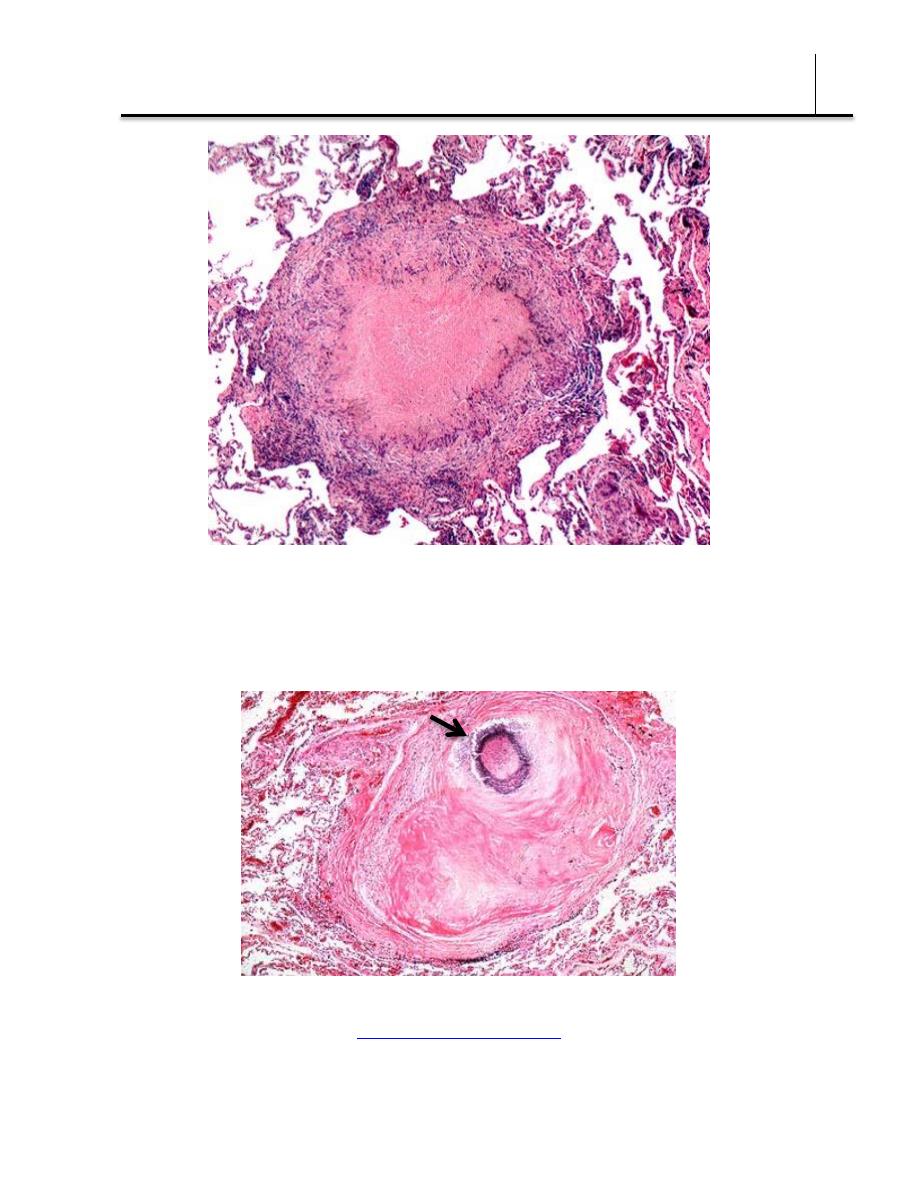
there, and form a cavity. It may subsequently heal by fibrosis or
calcification.
healed, fibrotic granuloma shows calcification (blue circle)
Bacteriology
Dr. Donya A Makki Mycobacteria
9
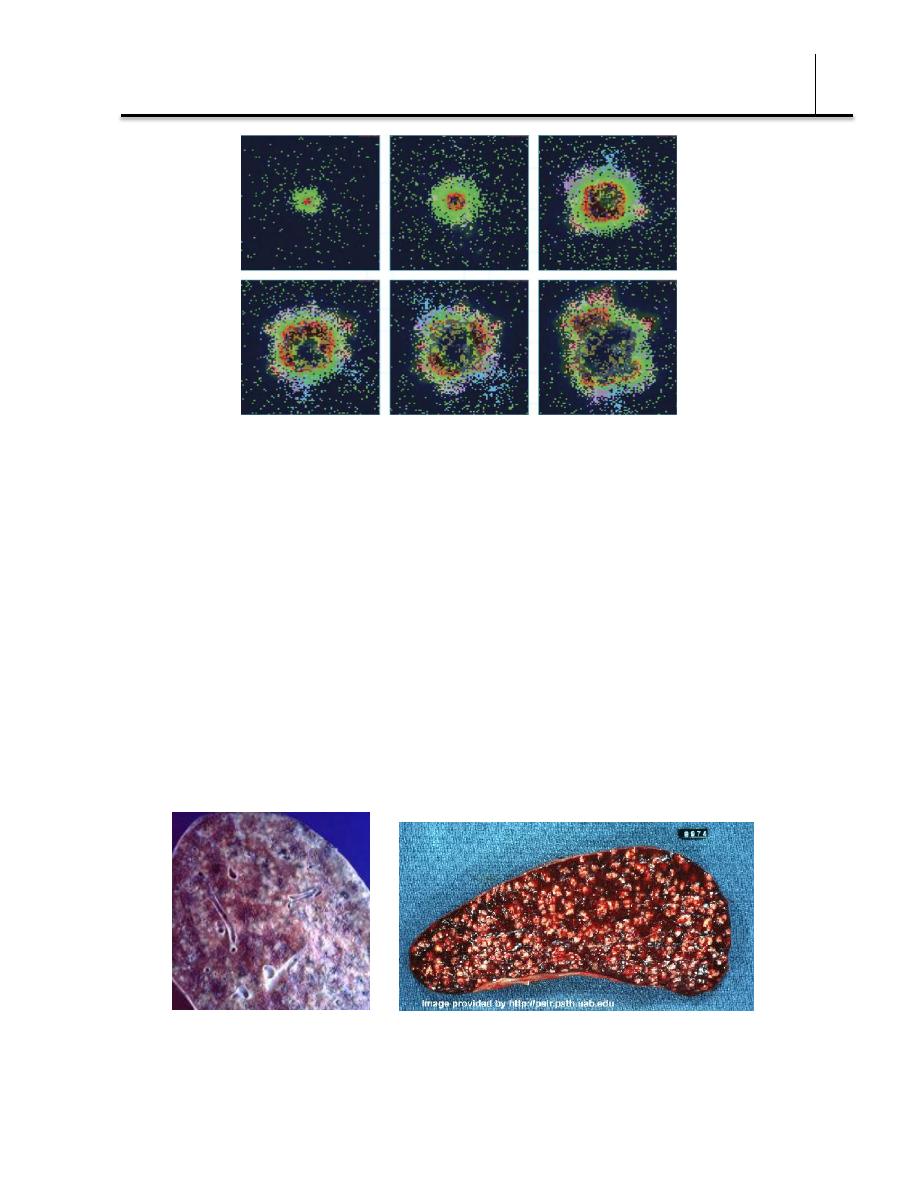
time-lapse simulation of a granuloma forming after infection with Mycobacterium tuberculosis
(days 0, 50, 75, 100, 150, 200), (green resting macrophage, red infected macrophage, brown
caseation, pink and light blue T cells)
©
Katharine Miller
B. Spread of Organisms in the Host
Tubercle bacilli spread in the host by direct extension, through the
lymphatic channels and bloodstream, and via the bronchi and
gastrointestinal tract.
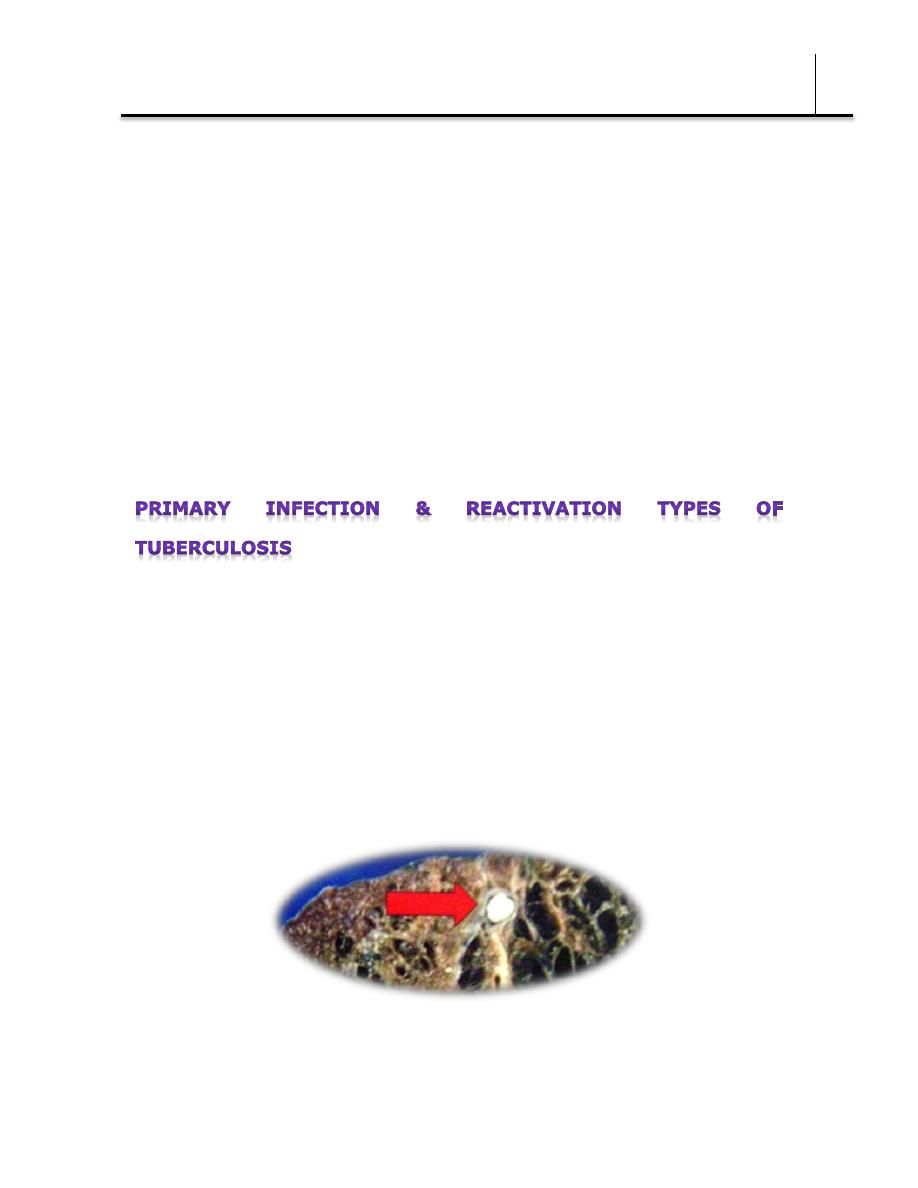
In the first infection, tubercle bacilli always spread from the initial site
via the lymphatics to the regional lymph nodes. The bacilli may spread
farther and reach the bloodstream, which in turn distributes bacilli to
all organs (miliary distribution).
A lung and spleen with miliary distribution of granulomas
The bloodstream can be invaded also by erosion of a vein by a
Bacteriology
Dr. Donya A Makki Mycobacteria
10
caseating tubercle or lymph node. If a caseating lesion discharges its
contents into a bronchus, they are aspirated and distributed to other
parts of the lungs or are swallowed and passed into the stomach and
intestines.
C. Intracellular Site of Growth
Once mycobacteria establish themselves in tissue, they reside
principally intracellularly in monocytes, reticuloendothelial cells, and
giant cells. The intracellular location is one of the features that makes
chemotherapy difficult and favors microbial persistence. Within the
cells of immune animals, multiplication of tubercle bacilli is greatly
inhibited.
When a host has first contact with tubercle bacilli, the following
features are usually observed:
(1) An acute exudative lesion develops and rapidly spreads to the
lymphatics and regional lymph nodes. The exudative lesion in tissue
often heals rapidly.
(2) The lymph node undergoes massive caseation, which usually
calcifies (Ghon lesion).
(3) The tuberculin test becomes positive.
Ghon lesion
This primary infection type occurred in the past, usually in childhood,
Bacteriology
Dr. Donya A Makki Mycobacteria
11
but now frequently in adults who have remained free from infection
and therefore tuberculin-negative in early life. In primary infections,
the involvement may be in any part of the lung but is most often at
the base.
The reactivation type is usually caused by tubercle bacilli that have
survived in the primary lesion. Reactivation tuberculosis is
characterized by chronic tissue lesions, the formation of tubercles,
caseation, and fibrosis. Regional lymph nodes are only slightly
involved, and they do not caseate. The reactivation type almost always
begins at the apex of the lung, where the oxygen tension (PO2) is
highest.
These differences between primary infection and reinfection or
reactivation are attributed to (1) resistance and (2) hypersensitivity
induced by the first infection. It is not clear to what extent each of
these components participates in the modified response in reactivation
tuberculosis.
During the first infection with tubercle bacilli, a certain resistance is
acquired and there is an increased capacity to localize tubercle bacilli,
retard their multiplication, limit their spread, and reduce lymphatic
dissemination. This can be attributed to the development of cellular
immunity, with evident ability of mononuclear phagocytes to limit the
multiplication of ingested organisms and even to destroy them.
In the course of primary infection, the host also acquires
hypersensitivity to the tubercle bacilli. This is made evident by the
development of a positive tuberculin reaction (see below). Tuberculin
sensitivity can be induced by whole tubercle bacilli or by
tuberculoprotein in combination with the chloroform-soluble wax D of
Bacteriology
Dr. Donya A Makki Mycobacteria
12
the tubercle bacillus, but not by tuberculoprotein alone.
Hypersensitivity and resistance appear to be distinct aspects of related
cell-mediated reactions.
Material
Old tuberculin is a concentrated filtrate of broth in which tubercle
bacilli have grown for 6 weeks. In addition to the reactive
tuberculoproteins, this material contains a variety of other constituents
of tubercle bacilli and of growth medium. A purified protein derivative
(PPD) is obtained by chemical fractionation of old tuberculin. PPD is
standardized in terms of its biologic reactivity as "tuberculin units"
(TU). First-strength tuberculin has 1 TU; intermediate-strength has 5
TU; and second-strength has 250 TU. Bioequivalency of PPD products
is not based on weight of the material but on comparative activity.
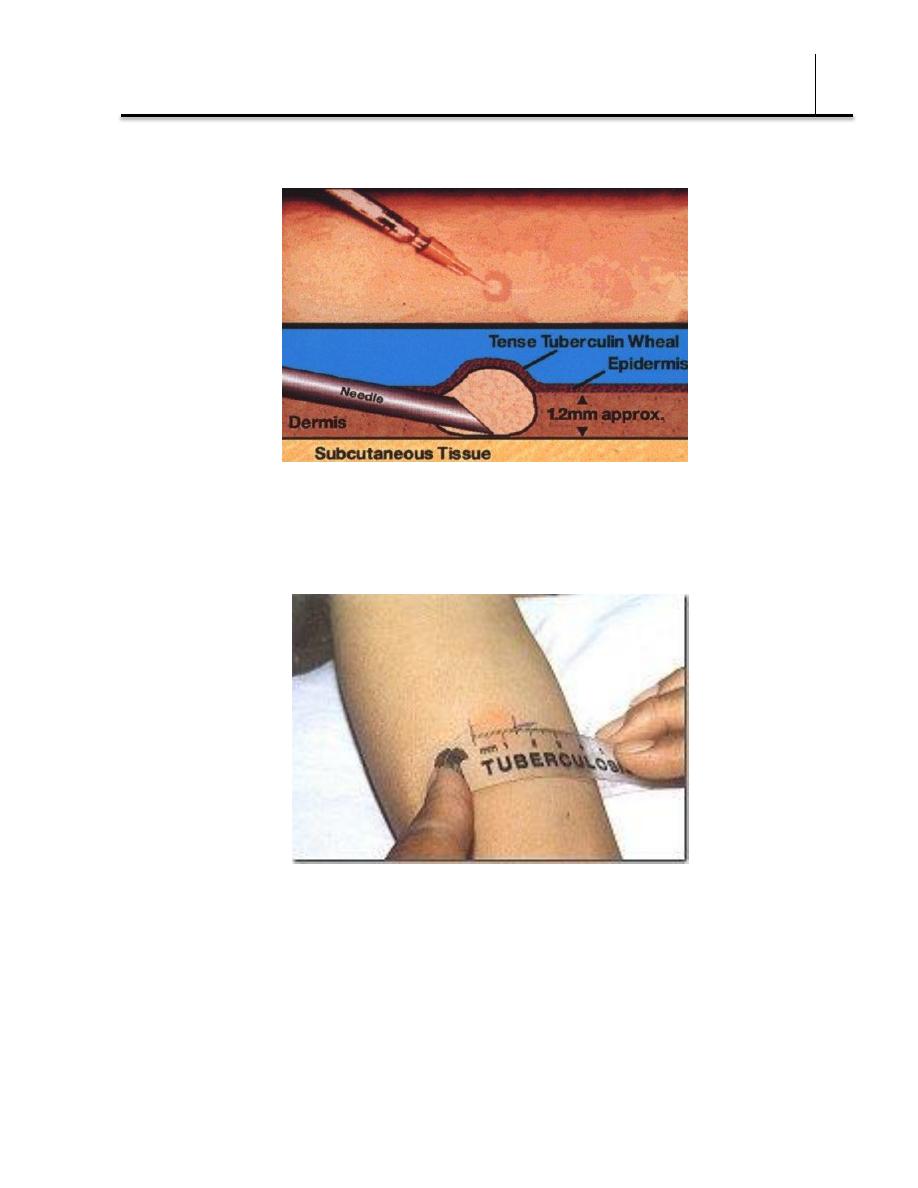
Dose of Tuberculin
A large amount of tuberculin injected into a hypersensitive host may
give rise to severe local reactions and a flare-up of inflammation and
necrosis at the main sites of infection (focal reactions). For this reason,
tuberculin tests in surveys employ 5 TU; in persons suspected of
extreme hypersensitivity, skin testing is begun with 1 TU. More
concentrated material (250 TU) is administered only if the reaction to
5 TU is negative. The volume is usually 0.1 mL injected
intracutaneously. The PPD preparation must be stabilized with
polysorbate 80 to prevent adsorption to glass.
Reactions to Tuberculin
In an individual who has not had contact with mycobacteria, there is
no reaction to PPD-S. An individual who has had a primary infection
with tubercle bacilli develops induration, edema, erythema in 24–48
Bacteriology
Dr. Donya A Makki Mycobacteria
13
hours, and, with very intense reactions, even central necrosis.
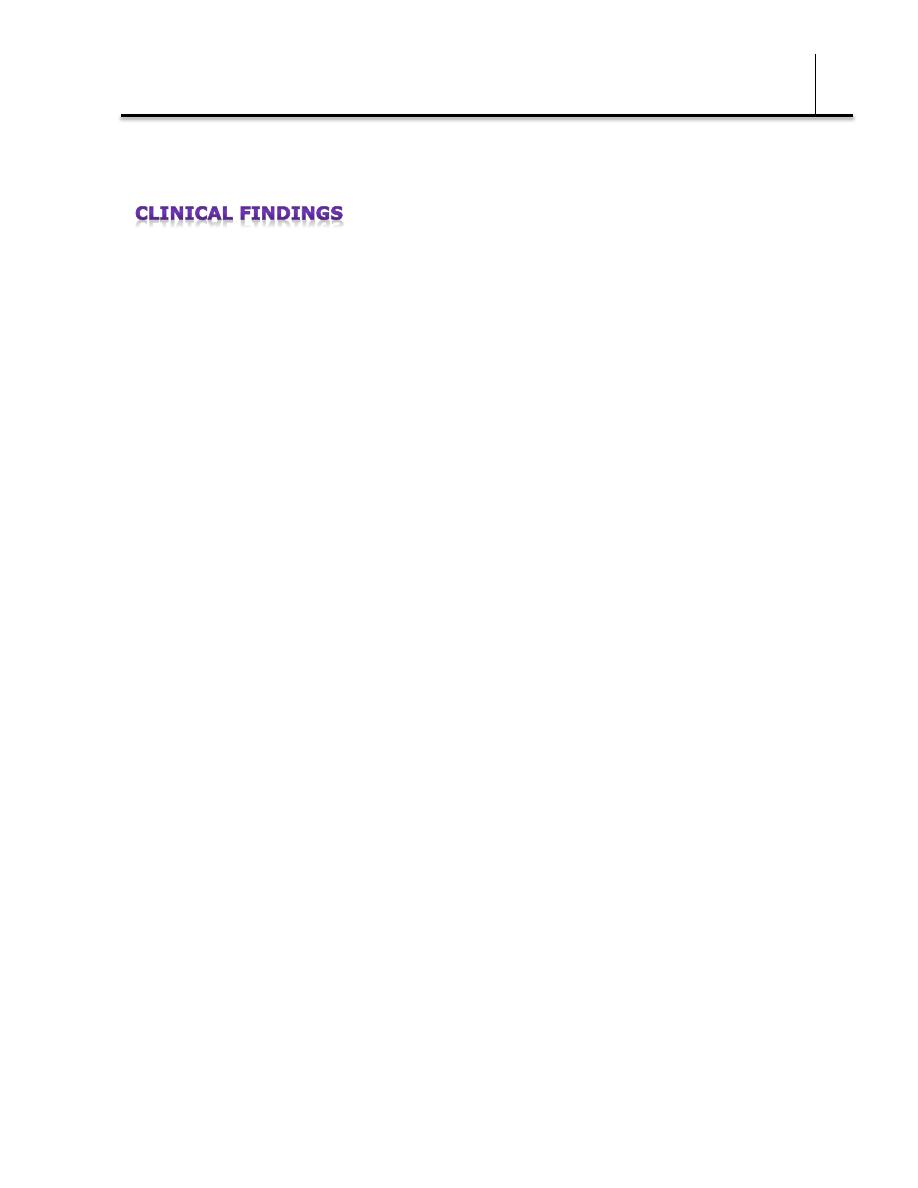
The skin test should be read in 48 or 72 hours. It is considered
positive if the injection of 5 TU is followed by induration 10 mm or
more in diameter.
Positive tests tend to persist for several days. Weak reactions may
disappear more rapidly.
The tuberculin test becomes positive within 4–6 weeks after infection
(or injection of avirulent bacilli).
It may be negative in the presence of tuberculous infection when
anergy (immune unresponsiveness) develops due to overwhelming

Bacteriology
Dr. Donya A Makki Mycobacteria
14
tuberculosis, measles, Hodgkin disease, sarcoidosis, AIDS, or
immunosuppression.
A positive tuberculin test may occasionally revert to negative upon
isoniazid treatment of a recent converter.
After BCG vaccination, people convert to a positive test, but this may
last for only 3–7 years.
Only the elimination of viable tubercle bacilli results in reversion of the
tuberculin test to negative. However, persons who were PPD-positive
years ago and are healthy may fail to give a positive skin test. When
such persons are retested 2 weeks later, their PPD skin test—
"boosted" by the recent antigen injection—will give a positive size of
induration again.
Interpretation of Tuberculin Test
A positive tuberculin test indicates that an individual has been infected
in the past. It does not imply that active disease or immunity to
disease is present. Tuberculin-positive persons are at risk of
developing disease from reactivation of the primary infection, whereas
tuberculin-negative persons who have never been infected are not
subject to that risk, though they may become infected from an
external source.
Gamma Interferon Release Assays for Detection of Tuberculosis
Sometimes the results of the tuberculin skin test are unclear,
particularly in persons who have been vaccinated with BCG or who live
in areas where nontuberculous mycobacteria are highly prevalent in
the environment. In an effort to improve diagnostic accuracy, whole-
blood gamma interferon release assays have been commercially
developed. These assays are based on the host's immune responses to
specific M tuberculosis antigens which are absent from most
nontuberculous mycobacteria and BCG. The tests detect interferon
Bacteriology
Dr. Donya A Makki Mycobacteria
15
gamma that is released by sensitized CD4 T cells in response to these
antigens.
Since the tubercle bacillus can involve every organ system, its clinical
manifestations are variable. Fatigue, weakness, weight loss, fever, and
night sweats may be signs of tuberculous disease.
Pulmonary involvement giving rise to chronic cough and spitting of
blood usually is associated with far-advanced lesions.
Meningitis or urinary tract involvement can occur in the absence of
other signs of tuberculosis.
Bloodstream dissemination leads to miliary tuberculosis with lesions in
many organs and a high mortality rate.