1
Lecture (1). Lecturer name: Dr. Saad Y. Sulaiman
The nose
Embryology:
The nose develops from a number of mesenchymal processes around the primitive
mouth .The nasal cavity is first recognizable in the 4
th
week of intrauterine life as an
ectodermal thickening called olfactory or nasal placode. Any interruption to
pregnancy at this time (4
th
week) will lead to congenital anomaly of the nose.
Anatomy:
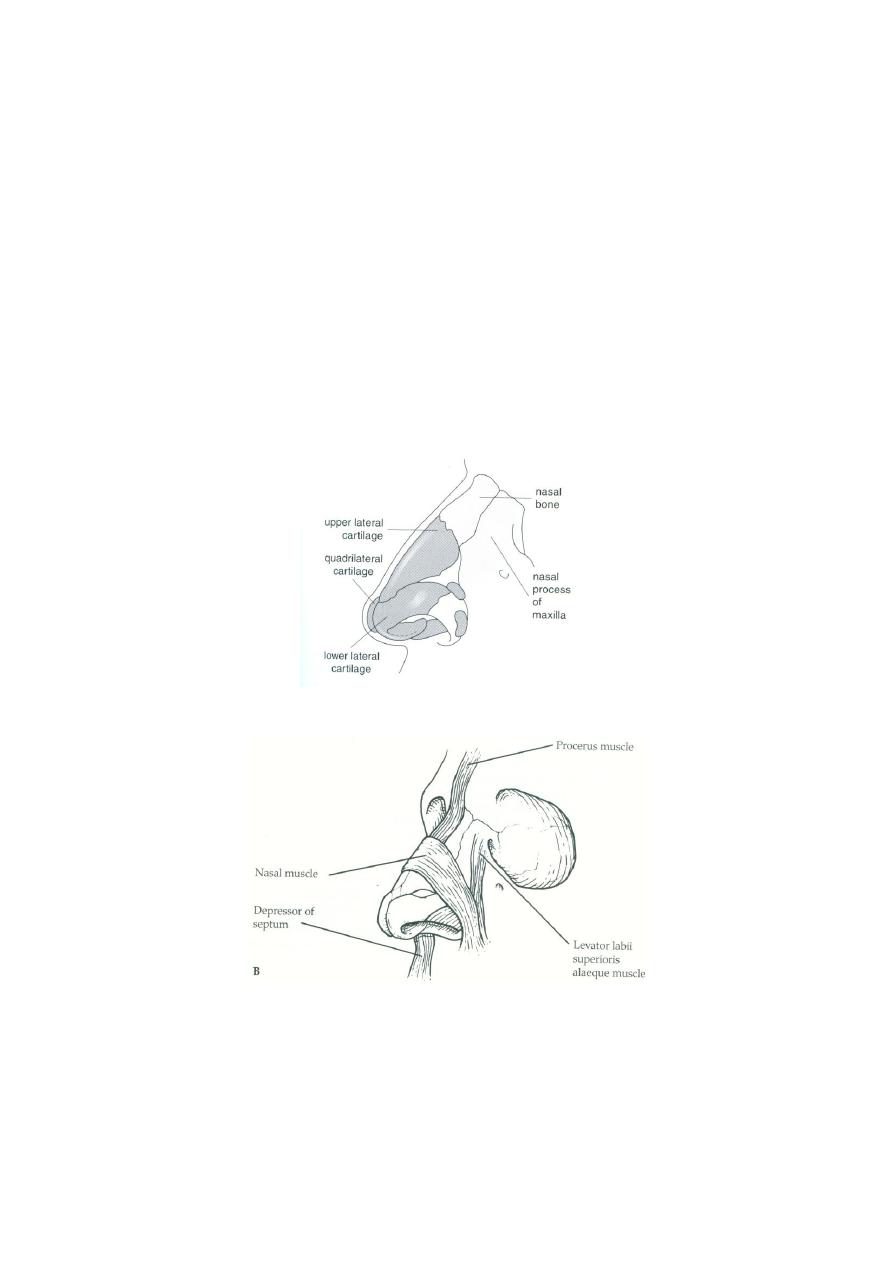
The external nose
(fig.1&2)
is supported by bone and cartilage. Attached to the
cartilages are the muscles for dilating the nares.
Fig.1
Fig.2
The vestibule
(fig.4)
is the dilated passageway leading from the external nares into
nasal cavity and is lined by skin bearing coarse hear (vibrissae), sebaceous glands and
sweat glands.
The nasal cavity is lined by mucus membrane (ciliated columnar epithelium ) and
divided by the nasal septum into two parts.
2
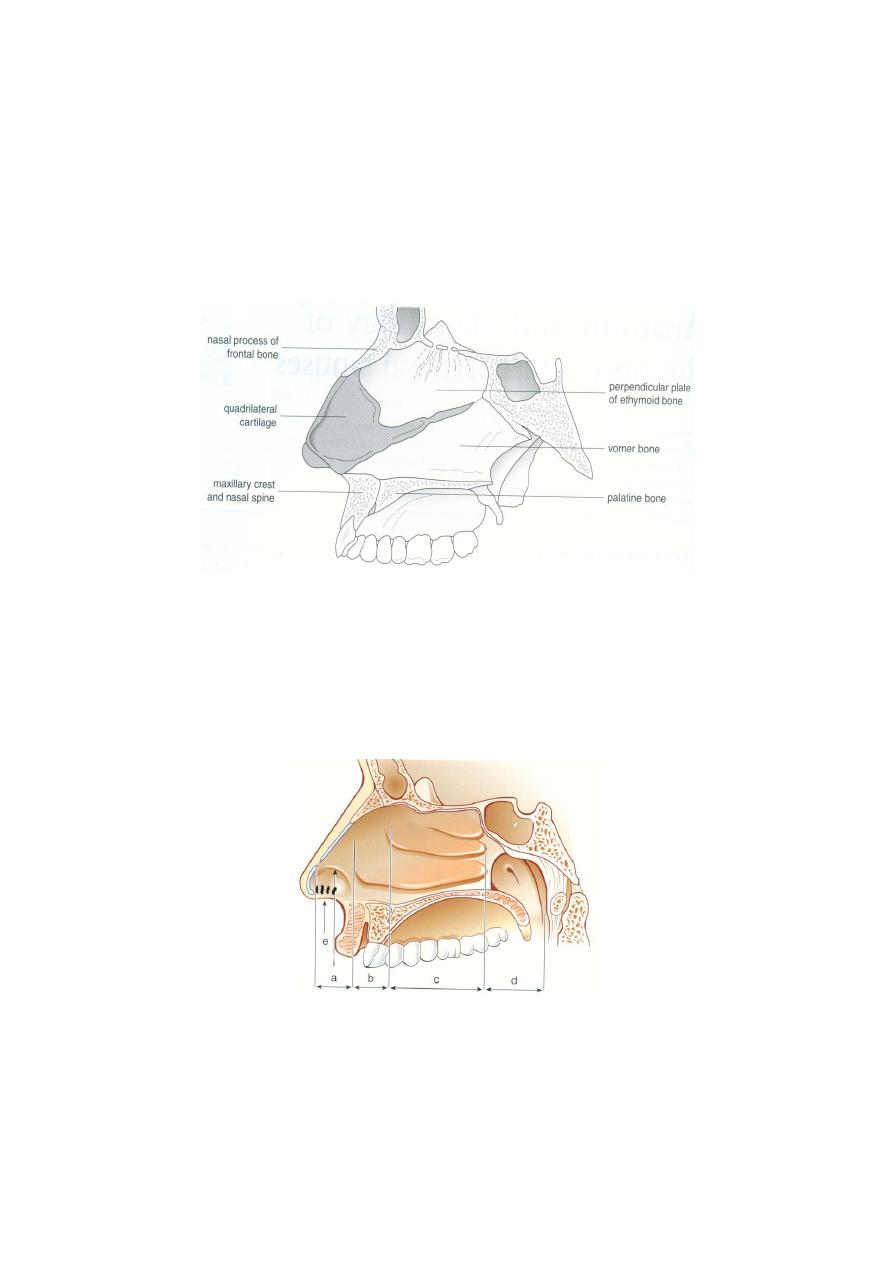
The septum (
fig.3)
is formed by:
Anteriorly
quadrilateral cartilage.
Posterosuperiorly
perpendicular plate of ethmoid.
Posteroinferiorly
vomer.
The septum is covered with perichondrium where there is cartilage, with periostium
where there is bone, and superficially with mucus membrane.
Fig.3
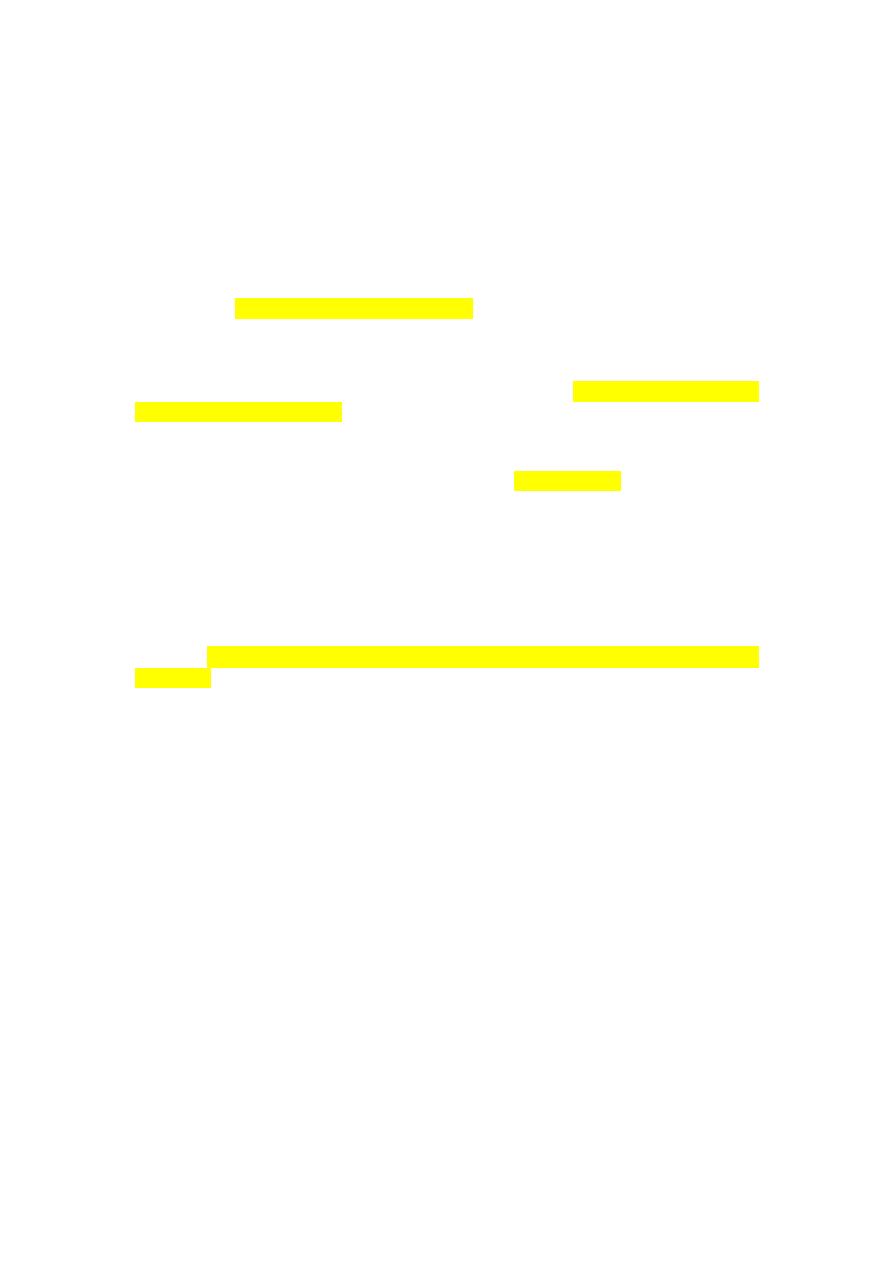
On the lateral wall
(Fig.4)
there is a system of ridges known as the turbinates
(chonchae), each of which overhangs a groove known as a meatus .There are three
turbinates: inferior, middle and superior. The inferior turbinate forms a bone by itself,
attached to the lateral wall of the nose. The middle and superior turbinates are part of
the ethmoid bone .The turbinates are covered with mucous membrane (columnar
ciliated epithelium). Underlying the mucous membrane there is erectile tissue.
Fig.4
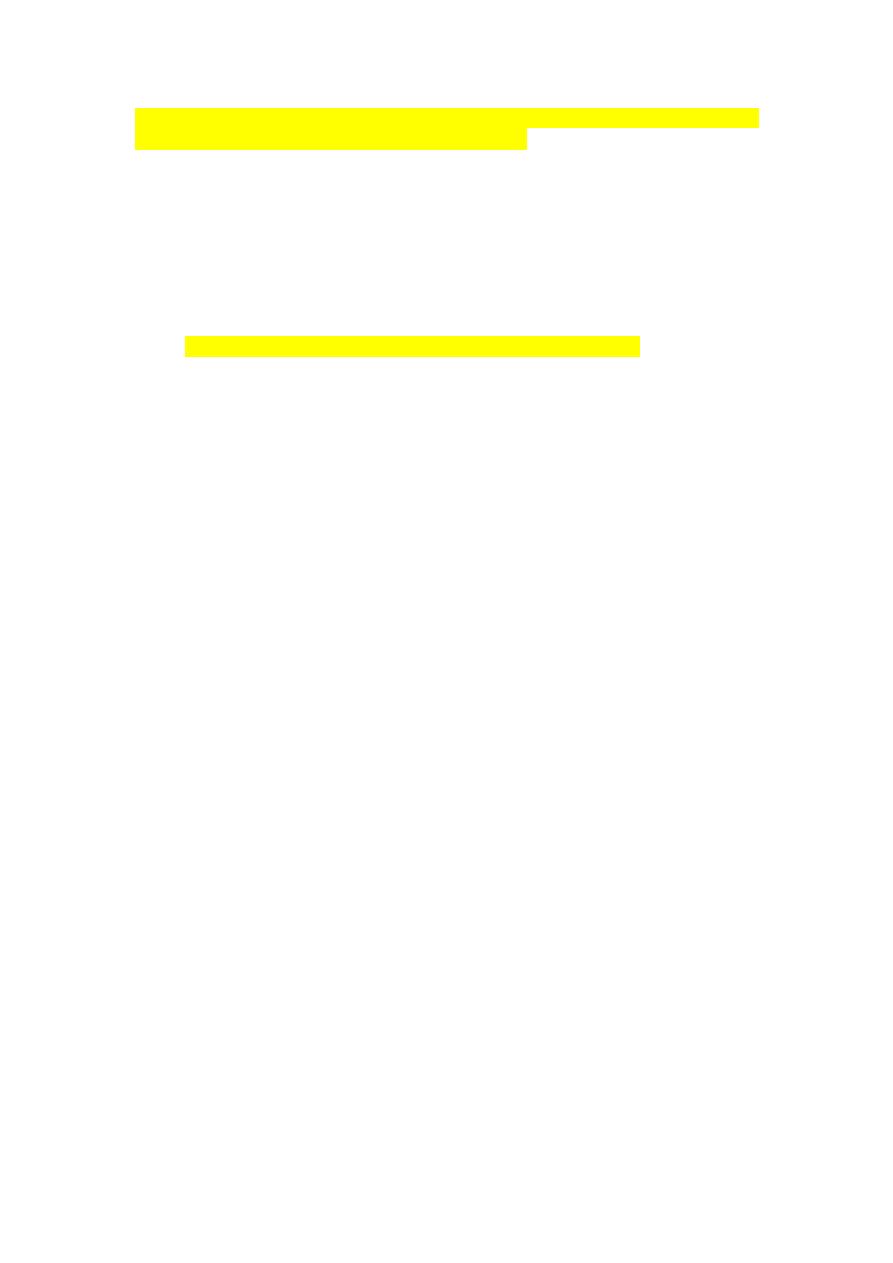
In the inferior meatus, the nasolacrimal duct is opened and trauma to the inferior
turbinate may affect this duct
(Fig5) .
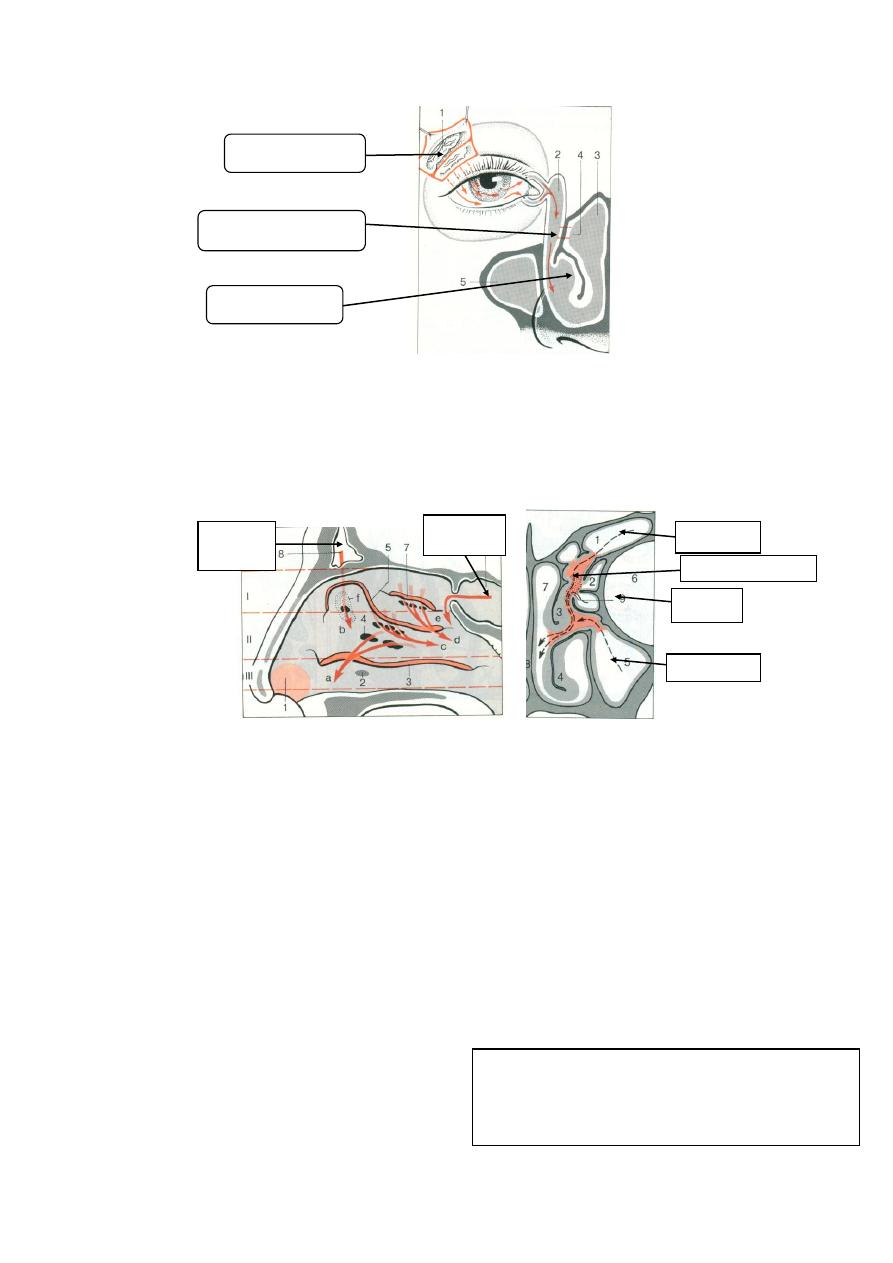
3
(Fig5)
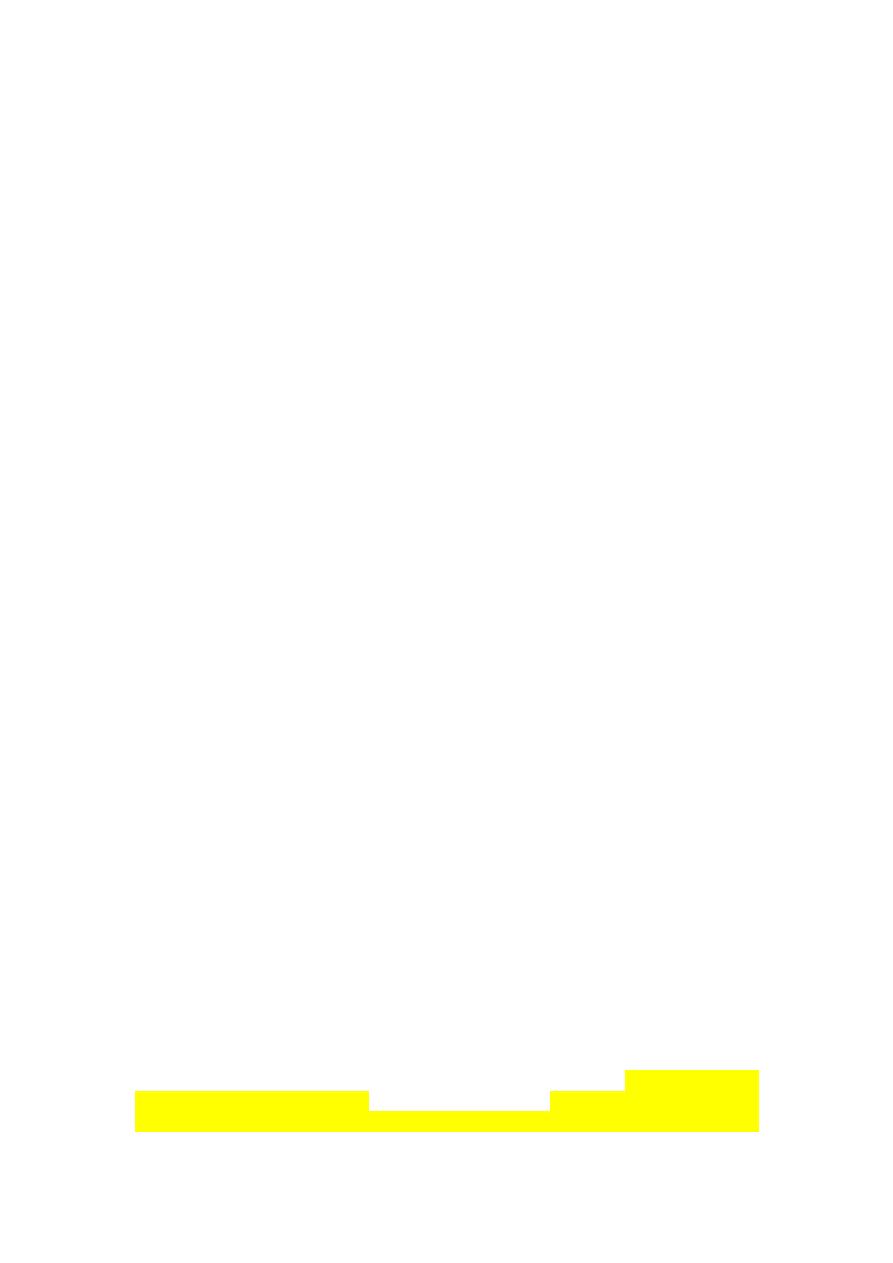
Most of paranasal sinuses opened into the middle meatus (maxillary, anterior
ethmoid and frontal sinuses)
(Fig6 &7)
. Therefore evaluation of the middle meatus and
its surrounding is considered the most important step during nasoendoscopy and this
entire area is called osteo-meatal complex and pathology in this region is indicative of
underlying sinus disease
(Fig.7)
. The posterior ethmoid sinus opens into the superior
meatus and the sphenoid into the sphenoethmoidal recess.
Fig.6
Fig.7
The floor is formed by the hard palate and the roof is formed by the nasal bones,
cribriform plate and the body of sphenoid
(Fig.4)
.
Posteriorly, the nasal cavity is connected to the nasopharynx through two apertures
lying on both sides of the posterior end of the septum, known as posterior choanae.
The nasopharynx is connected to the middle ear via Eustachian tube; therefore,
rhinosinusitis may be a cause of otitis media
(Fig.4)
.
Nerve supply
:
The sensory nerve supply is from trigeminal nerve
Secretory nerve supply comes through Vidian nerve (nerve of pterygoid canal) which
is formed by the junction of the greater petrosal nerve, a branch of the facial nerve
(parasympathetic) and the deep petrosal nerve (sympathetic) derived from the
sympathetic plexus on the internal carotid artery .
The olfactory nerves enter the nose through the cribriform plate in the roof.
Frontal
s.
M axillary S.
Orbit
Osteo-meatal complex
Sphenoid
Sinus
Frontal
sinus
Lacrimal gland
Nasolacrimal duct
Inferior meatus
- Greater petrosal nerve (parasymp.)
Dilates
blood vessels + enhance gland secretion.
- Deep petrosal nerve (symp.)
constricts blood
vessels.
4
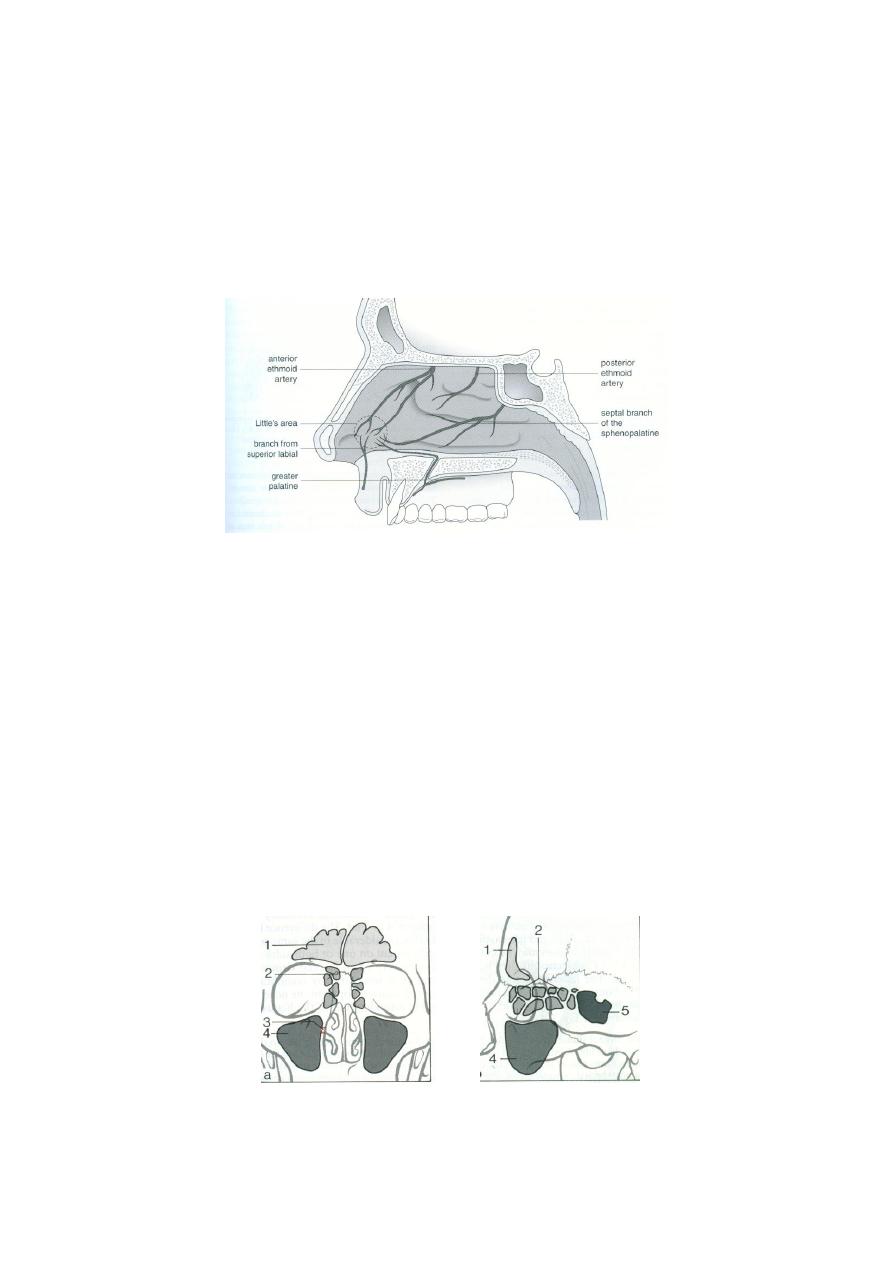
Arterial supply :
(
Fig.8)
The nose is supplied by branches from the int.&ext. carotid arteries, which
anastomose freely in the nose .An aggregation of poorly supported vessels on the
anterior part of the septum just behind the skin margin is known as Little`s area
(Kiesselbach`s plexus). This area is a common site of epistaxis and is formed by
anastomoses of anterior ethmoid artery, superior labial artery, sphenopalatine artery
and greater palatine artery.
( Fig.8)
Venous Drainage; Facial + ophthalmic vein
cavernous sinus.
The lymphatic vessels drain posteriorly to the superior deep cervical group.
Physiology of the nose
:
The chief functions of the nose are:
1) Olfaction.
2) Filtration.
3) Humidification.
There are other functions, such as vocal resonance, self-cleansing and the provision of
moisture for the protection of mucous membrane.
Paranasal sinuses:
Fig.9 (a) Ant. view Fig.9 (b)Lat..view
5
These are air spaces which develop in the bones of the skull and communicate with
the nasal cavity. They are arranged in pairs and are functionally divided into anterior
and posterior groups. All the anterior group – frontal anterior ethmoid and maxillary –
drain into the middle meatus. The posterior ethmoid cells drain into the superior
meatus and the sphenoid into the sphenoethmoid recess.
The maxillary sinus: (The antrum)
This sinus is pyramidal in shape. It is the largest sinus (average size 15 ml in adult).
Its roof is the floor of the orbit and its floor is related to the tooth roots, particularly
those of the second premolar and first molar, which may project into the sinus and
may be covered only by a thin plate of bone, therefore maxillary sinusitis may be due
to apical tooth abscess. Extraction of such poorly covered tooth can result in oroantral
fistula. Its medial boundary (the base) forms the lateral nasal wall. The ostium of the
sinus is sited high in the medial wall (1 cm) and hence drainage is dependent on
ciliary action and not gravity.
The frontal sinus:
The sinus is not present at birth but appear at the age of 5 years. The sinus is frontal
in location but ethmoidal in origin. The frontal sinuses are rarely symmetrical and
they are separated by a thin bone. The roof of the orbit forms the floor of the frontal
sinus
.
The ethmoid sinus (the ethmoid air cells):
The ethmoidal sinuses are multiple air cells (7-15) in number and divided into
anterior and posterior groups which drain respectively below and above the middle
turbinate. They are separated from the orbit by a thin plate of bone known as lamina
papyracea.
The sphenoidal sinus:
This sinus occupies the body of the sphenoid bone and drains into the
sphenoethmoidal recess. The pituitary gland is located on its roof whereas the lateral
wall is in contact with the cavernous sinus. The Vidian nerve passes below this sinus.
Function of paranasal sinuses:
The physiological role of paranasal sinuses is uncertain. They are a continuation of
the respiratory cavity and covered by respiratory mucosa. They may have the
following functions;
(1) Decrease the weight of the skull.
(2) Warming and moistening of the air.
(3) Add resonance to the laryngeal voice.
(4) Temperature buffer.
Symptoms of Nasal Diseases
I.
Nasal obstruction:
1. Anatomical abnormality: Congenital choanal atresia or deviated nasal septum.
2. Abnormality of the mucous membrane: Nasal polyposis or turbinate
hypertrophy.
6
3. Abnormalities of autonomic control of the mucosa: Vasomotor rhinitis.
II. Nasal Discharge:
1. Watery clear discharge: Onset of common cold, allergic rhinitis or CSF
rhinorrhea.
2. Mucopurulent:
-Yellow pus: Sinusitis.
-Unilateral foul discharge in a child: FB in the nose.
-Crusts in adults: Atrophic rhinitis.
3. Thick blood stained discharge: Tumour.
4. Postnasal mucopurulent discharge: Disease of the posterior group of sinuses.
III. Sneezing: Allergic rhinitis or common cold.
IV. Pain:
1. Severe local pain: Folliculitis.
2. Early morning headache: Sinusitis.
V. Epistaxis.
VI. Disturbance of smell
--------------------------------------------------
Inflammatory conditions of the nose
(1) Inflammations confined mainly to the external nose ;
(A) Common skin disease ; e.g. Impetigo , Acne and Lupus Erythematosus.
(B) Others which are particularly important in the nasal area ;e.g. nasal eczema
vestibulitis, furunculosis, Herpes simplex and Herpes zoster, rhinophyma
…etc.
(2) Inflammations mainly confined to the nasal cavity :
(A)Allergic rhinitis.
(B) Viral rhinitis (coryza).
(C) Non-Allergic rhinitis (intrinsic or vasomotor rhinitis).
(D) Atrophic rhinitis.
FURUNCULOSIS:
(Furuncle =boil) It is an acute infection of a hair follicle with staphylococcus
aureus. The hair bearing area of the nasal vestibule is a vulnerable site due to the
strong hairs and mechanical trauma to this area. It starts as a hard tender red nodule
which enlarges and becomes more painful and fluctuant. The majority discharge into
the nasal vestibule and resolves. A serious (although rare) complication is the spread
of the infection through the valveless superior ophthalmic veins to the cavernous sinus
leading to cavernous sinus thrombosis which characterized by severe illness with
fever, prostration and convulsion. Local changes include oedema with cyanosis of the
eyelids and base of the nose and chemosis due to obstruction of the ophthalmic vein.
7
Ophthalmoplegia and papillary changes (dilated or small immobile) are common.
Retinal haemorrhage and papilloedema are late events.
TREATMENT:
a. Avoid squeezing the nose.
b. Systemic antibiotic (against staphylococcus aureus like ampiclox or
lincomycin).
c. Analgesic.
d. Soothing ointment.
VESTIBULITIS:
Is inflammation of the vestibule with recurrent crusting and pain, usually due to
infection with staphylococcus aureus .It may also be caused by an irritant dermatitis-
like reaction due to watery rhinorrhoea (e.g. in acute coryza and allergic rhinitis).
Unilateral vestibulitis in a child or mentally impaired person should raise suspicion of
a foreign body. Offensive discharge is a further strong evidence.
TREATMENT:
1) Management of underlying predisposing factors (e.g. by giving antihistamine in
rhinorrhoea caused by allergy or viral infection and by removal of foreign body )
2) Mild topical (corticosteroid + antibiotic) ointment.
__________________________________________________________________