Clinical considerations in Fixed partial denture
Dr. Ahmed Jawadمعالجة اسنان \ المرحلة الخامسةالمحاضرة (2)
HISTORY
1. Personal detailsPatient's name
Address
Phone number
Gender
Occupation
Work scheduleMarital and financial status
Include all relevant information concerning the reasons for seeking treatment, along with any personal information, including relevant previous medical and dental experiences.
2. Chief complaint:
Chief complaints usually fall into one of the following four categories:Comfort (pain, sensitivity, swelling)
Function (difficulty in mastication or speech)
Social (bad taste or odor)
Appearance (fractured or unattractive teeth or restorations, discoloration)
• Medical history
• Conditions affecting the treatment methodology (e.G., Any disorders that necessitate the use of antibiotic premedication, any use of steroids or anticoagulants, and any previous allergic responses to medication or dental materials).
• Conditions affecting the treatment plan (e.G., Previous radiation therapy, hemorrhagic disorders, extremes of age, and terminal illness).
3. Systemic conditions with oral manifestations for example, periodontitis may be modified by diabetes, menopause, pregnancy, or the use of anticonvulsant drugs , in cases of hiatal hernia, bulimia, or anorexia nervosa, teeth may be eroded by regurgitated stomach acid..
4. Possible risk factors to the dentist and auxiliary personnel (e.G., Patients who are suspected or confirmed carriers of hepatitis B, acquired immunodeficiency syndrome, or syphilis).
4. Dental history
Periodontal history, restorative history, endodontic history, orthodontic history, removable prosthodontic history, oral surgery history, radiographic history, TMJ dysfunction historyEXAMINATION
DIAGNOSISA typical diagnosis will condense the information obtained during the clinical history taking and examination.
• General and local factors, varies from patient to patient.
PROGNOSIS
Factors Influencing Fixed Bridge Design
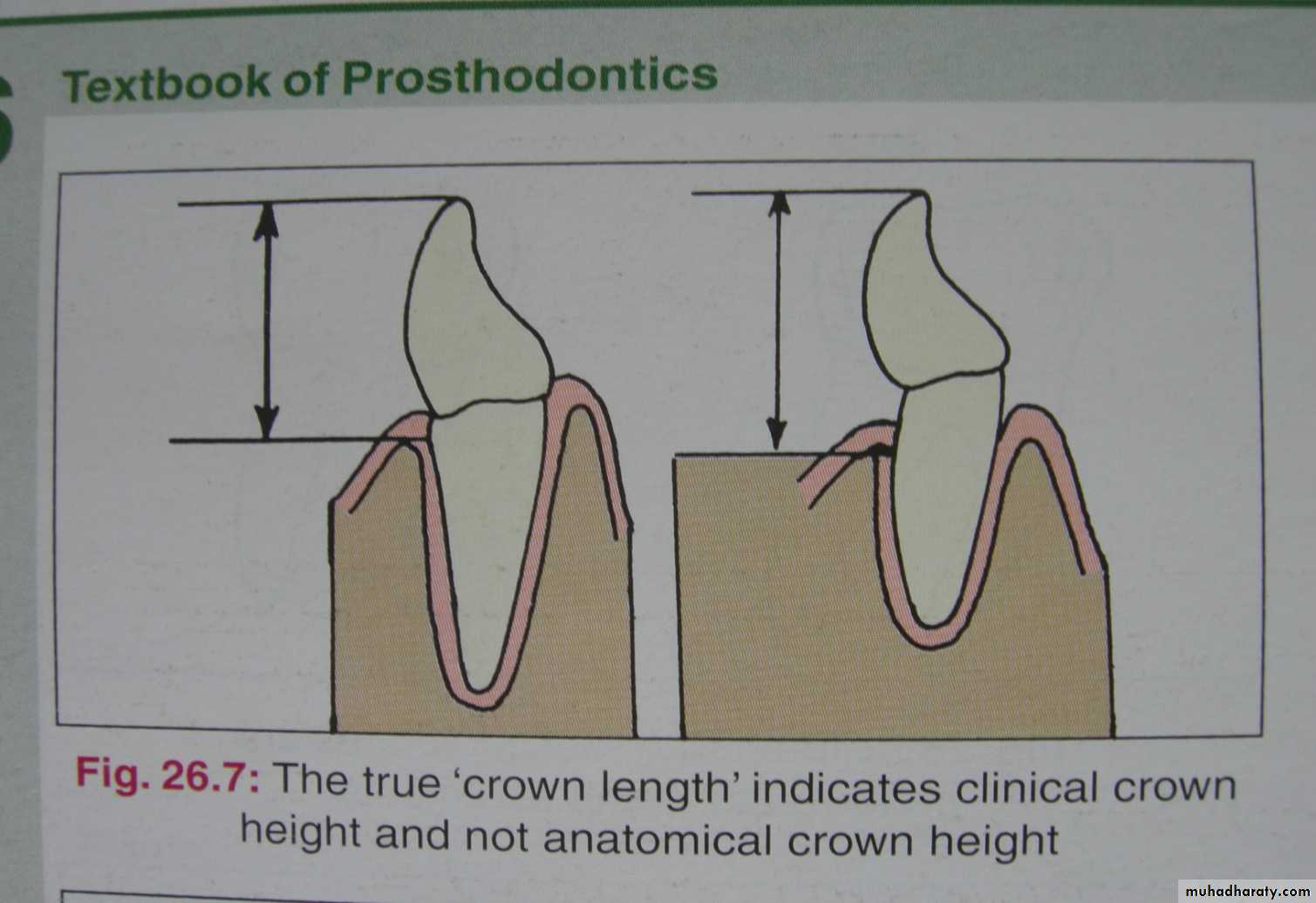
1. Crown LengthTeeth must have adequate occlusocervical crown length to achieve sufficient retention
2. Crown Form
Some teeth have tapered crown form which interferes with parallelismIncisors possessing very thin highly translucent incisal edges
3. Degree of MutilationSize, number and location of carious lesions or restorations affect whether full or partial coverage retainers are indicated
Fractured or carious teeth not restorable should be removed thereby altering design and creating the need for a prosthesis
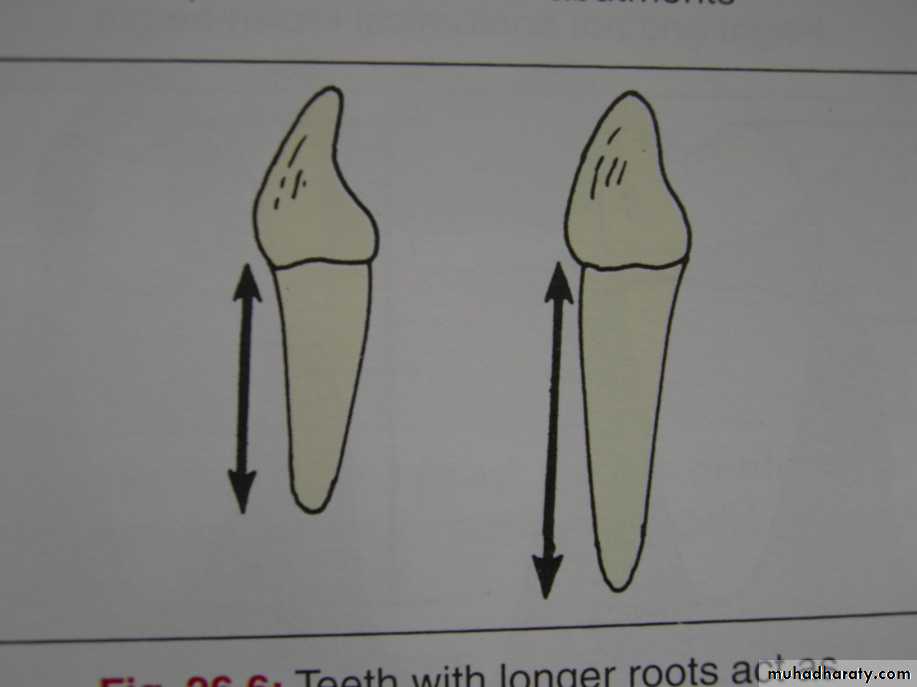
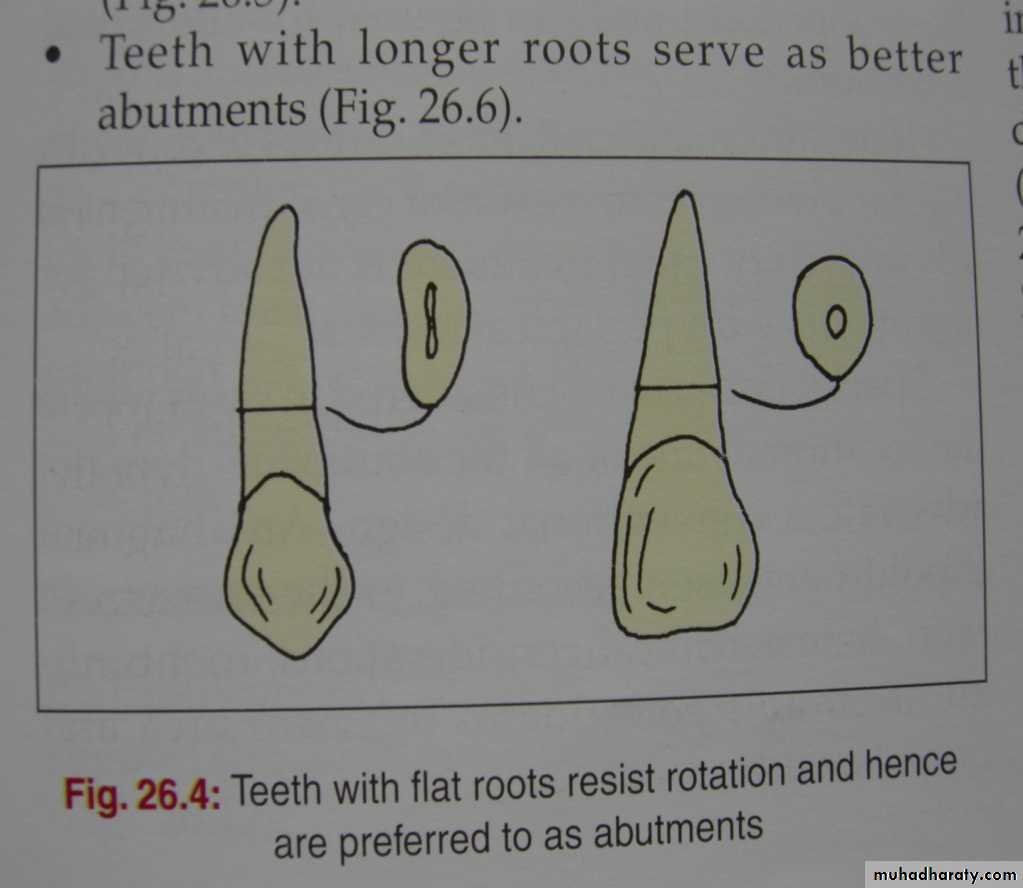
4. Root Length and Form
Roots with parallel sides and developmental depressions are better able to resist additional occlusal forces than are smooth-sided conical rootsMultirooted teeth generally provide greater stability than single-rooted teeth
Longer root has better retention than short root
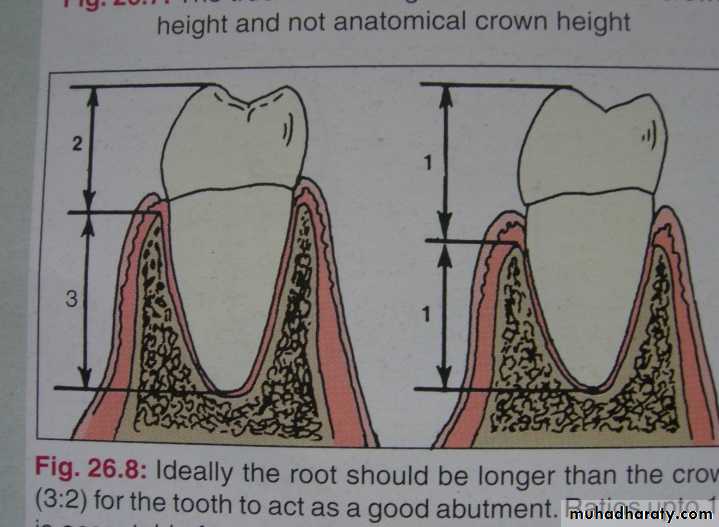
5. Crown-Root Ratio
1:1.5 ratio has been generally acceptable whereas 1:1 ratio is considered minimal and requires consideration of other factors (ex. # Of tooth being replaced, tooth mobility, periodontal health) before it can be used as an abutment
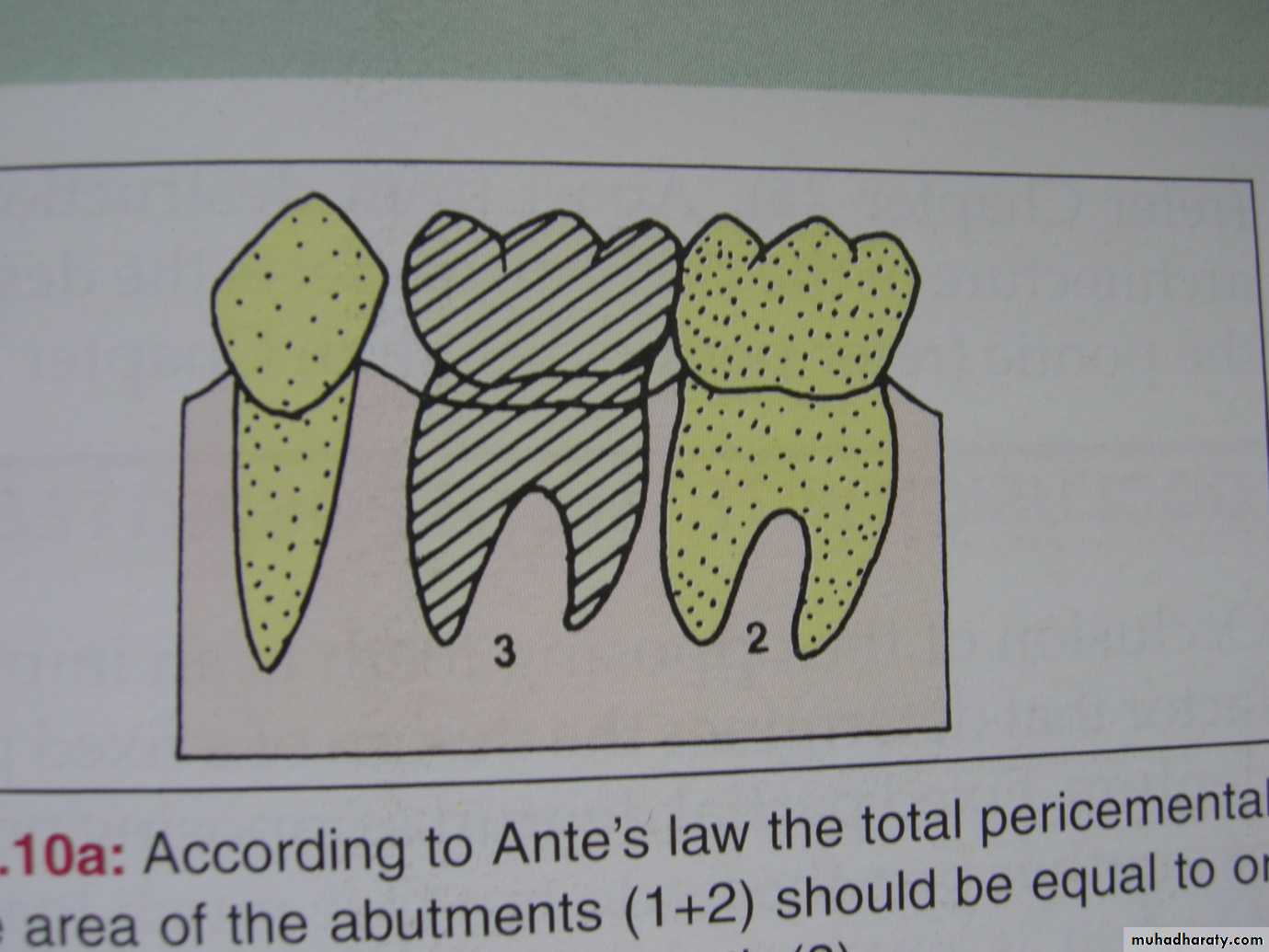
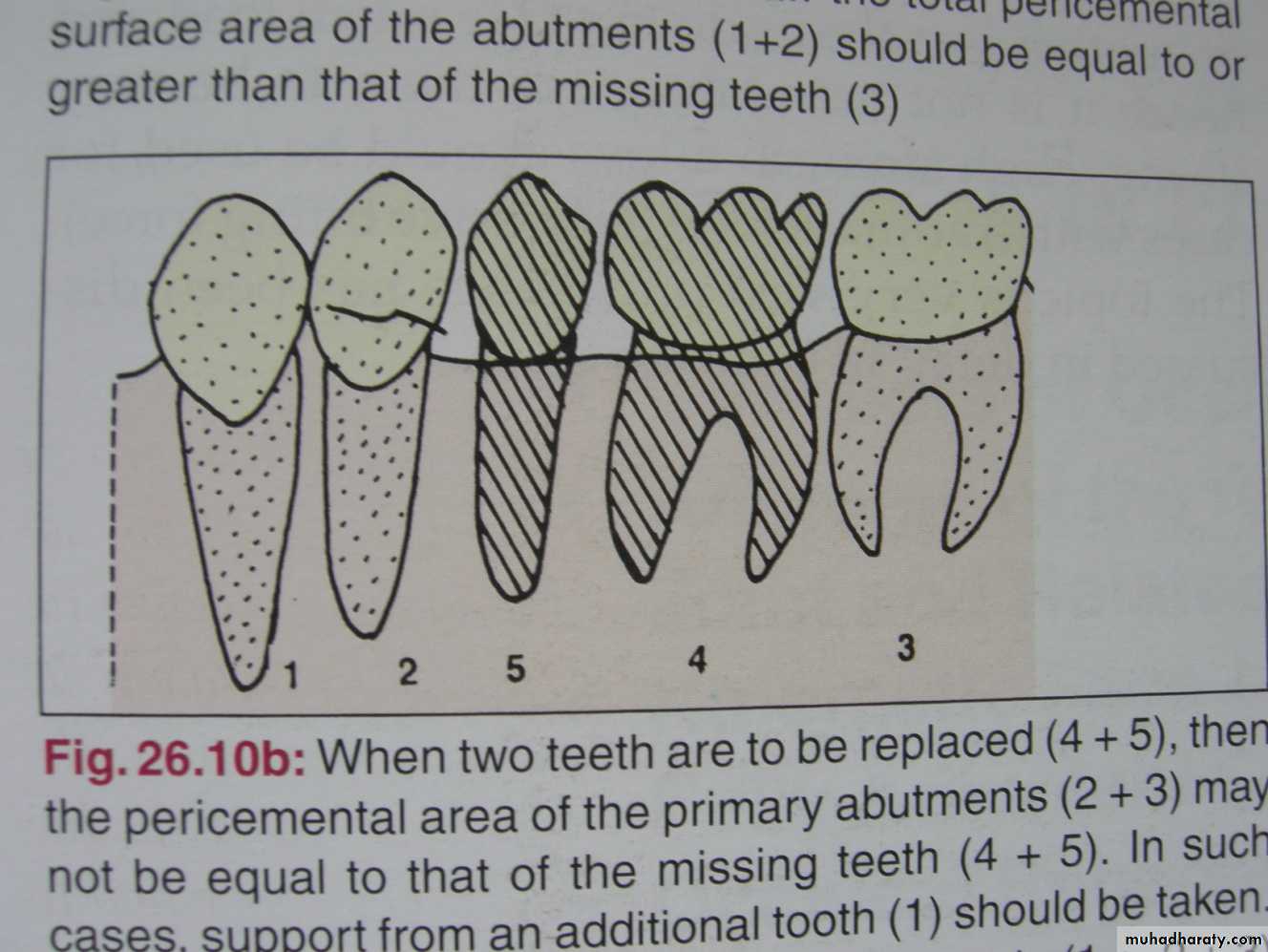
6. Ante’s Law
Periodontal ligament area/pericemental area of the abutment teeth should be equal or greater than the periodontal ligament area/pericemental area of the missing tooth/teeth1
7. Periodontal Health
Absence of any form of periodontal disease such as bone resorption and gingival recession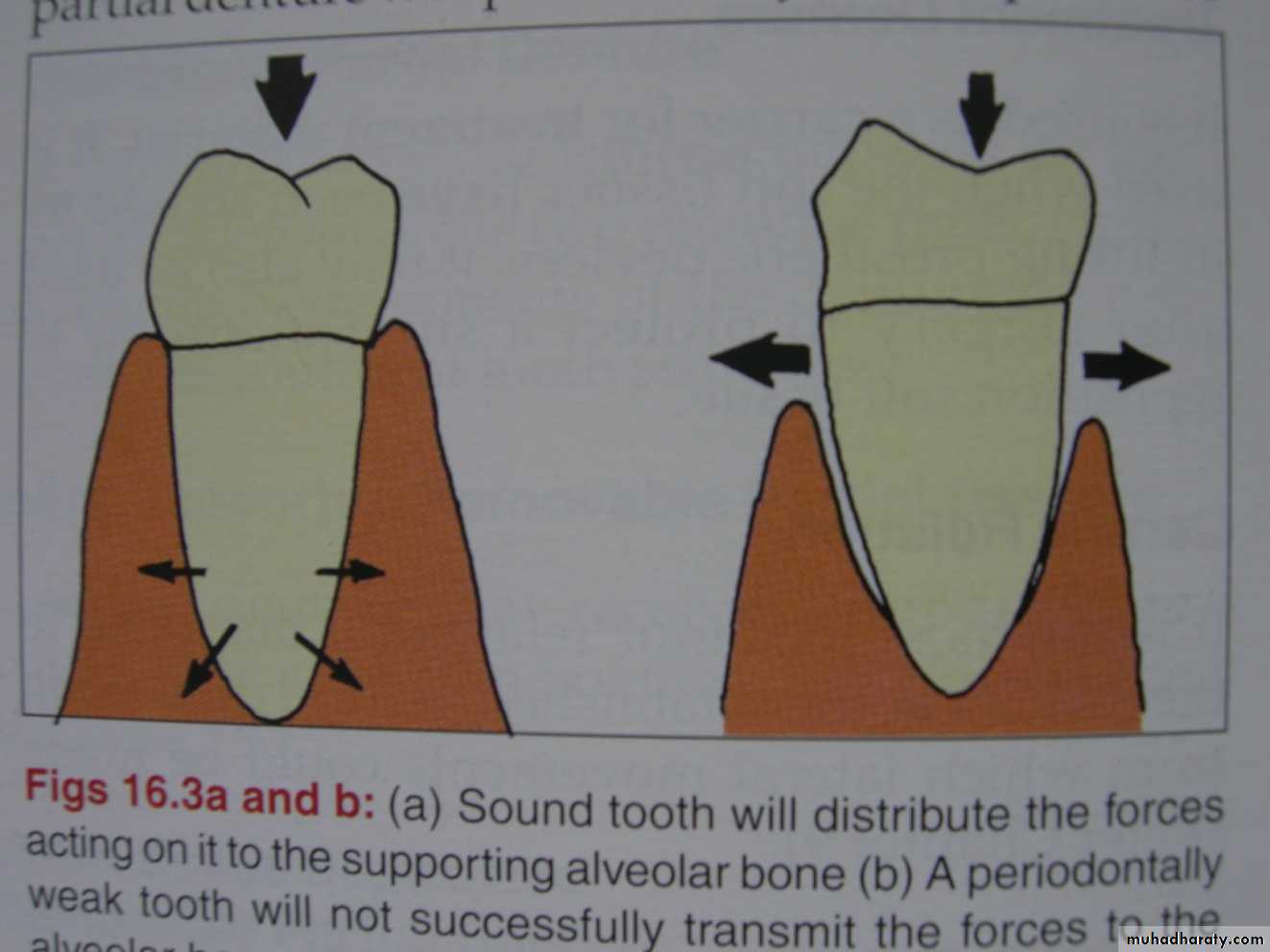
8. Mobility
Miller mobility value
• 1o mobility – normal• 2o mobility – still acceptable provided that you must know the factor that cause the mobility (patient age, presence of calcular deposit) and consider the # of tooth being replaced
• 3o mobility – can not be used as an abutment.
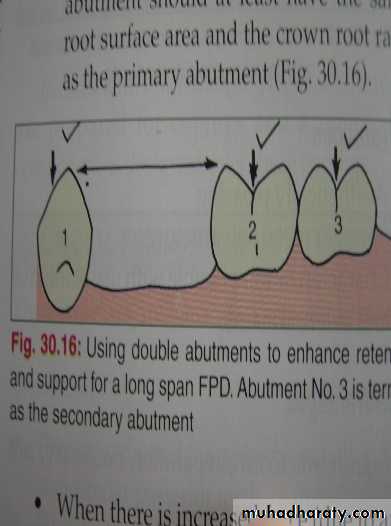
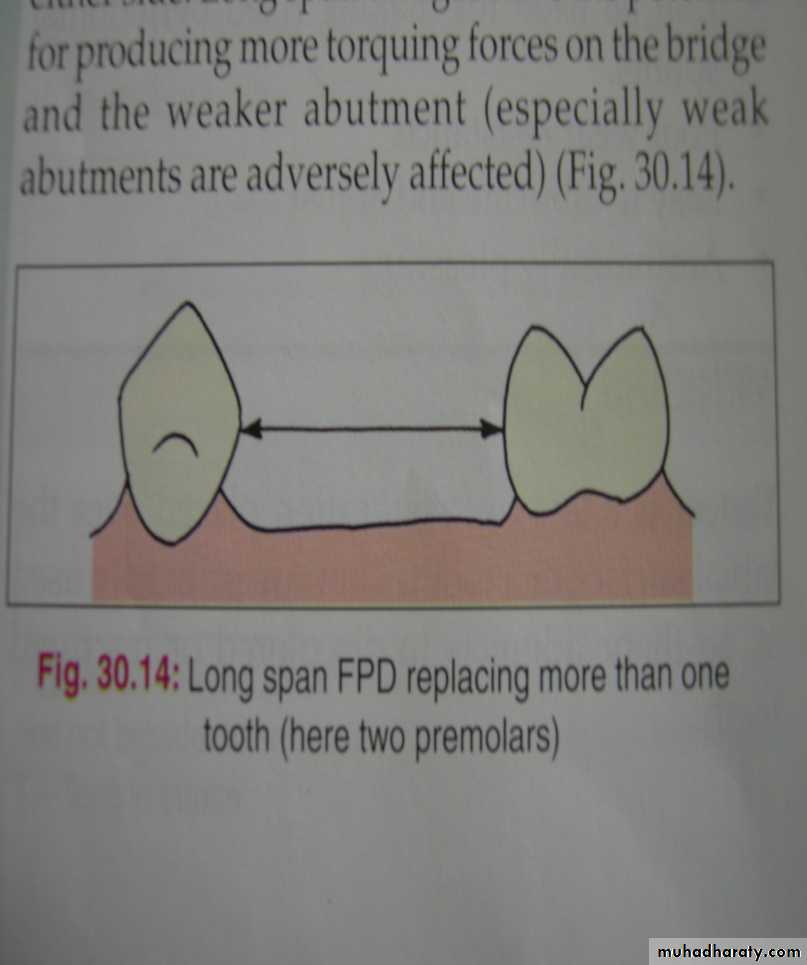
9. Span Length
Distance between abutments affects the feasibility of placing fixed prosthesisIdeal for 1-2 missing tooth
Loss of 3 adjacent tooth requires careful evaluation of other factors (crown-root ratio, root length and form, periodontal health, mobility)
Primary abutment
Secondaryabutment
10. Axial Alignment
Crowns of proposed abutments must be well aligned
Minor alterations in axial alignment (tipped/rotated) often necessitate the use of full coverage crowns to achieve retention or acceptable esthetics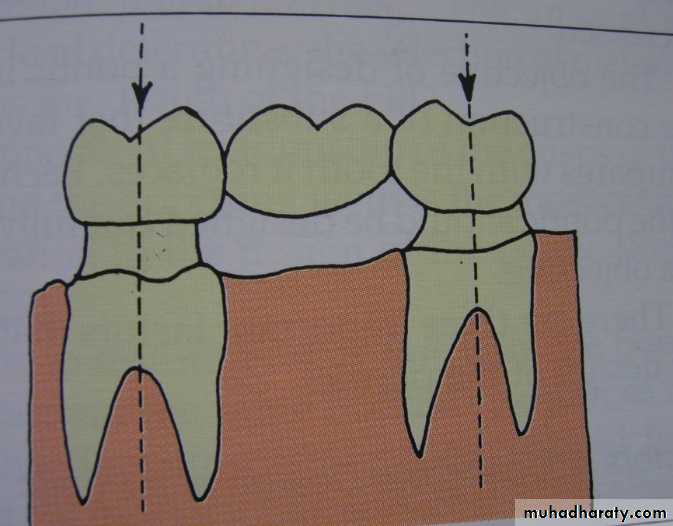
11. Arch Form
fulcrum linefulcrum line
lever
lever
counter-balancing
12. OcclusionOcclusal forces brought to bear on a prostheses are related to the following factors:
A. Degree of muscular activityB. Patients habit
C. # Of tooth being replaced
D. Leverage on the bridge
E. Adequacy of bone support
13. Pulpal Health
Abutment/s should not be sensitive to percussion or vitality testing (normal response)
Abutments with poor pulpal health should undergo endodontic treatment prior to tooth preparation14. Alveolar Ridge Form
Not indicated for FPD if there is considerable bone loss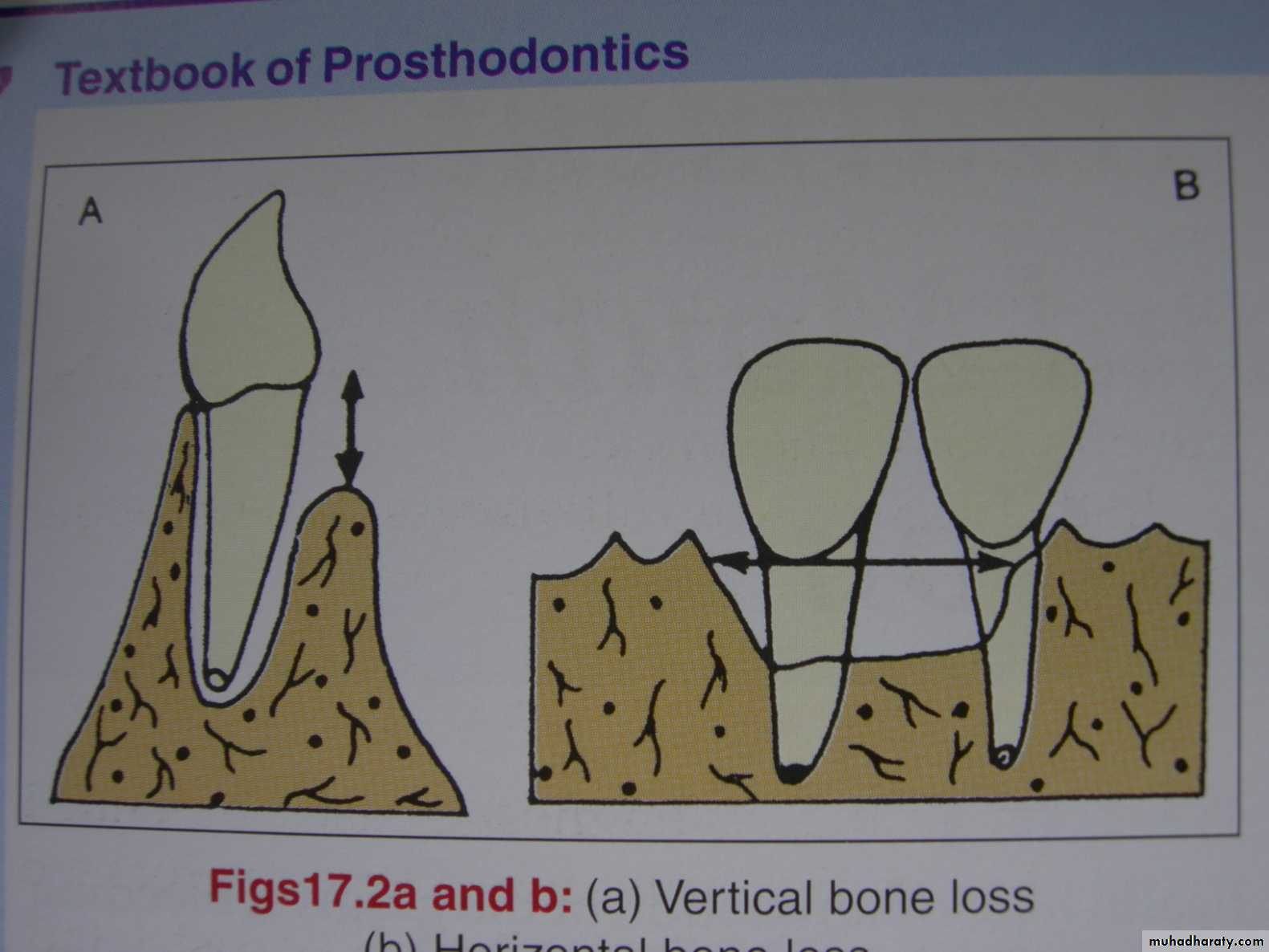
Vertical bone loss
Horizontal bone loss15. Age of Patien
Not indicated in older patient as well as adolescents when teeth are not fully erupted or with large pulps16. Phonetics
Patients prefer FPD for good phonation (provides sufficient resistance to the flow of air to allow normal speech sounds to be produced) rather than RPD17. Long-Term Abutment Prognosis
Take note of the oral hygiene
If there is question on the ability of the remaining supporting structure to accept additional occlusal forces, RPD is indicated
Tooth with sufficient loss of periodontal support and questionable prognosis may be best treated with an RPD rather than an FPD
18. Esthetics
Prefer FPD because it resembles natural toothBut RPD may be indicated when the use of a pontic produces large and unsightly proximal embrasures in a fixed prostheses.
19. Psychological Factors
To most patients an FPD feels more normal than an RPD and more quickly becomes an accepted part of the oral environmentPatients feels more confident and looks good wearing FPD than RPD