
Dr.Amina Zakaria Al-tutunji
M.B.Ch.B, MD.
Obstetrics and Gynecology
College of medicine/ University of Mosul
2016-2017
LEC3
Abnormal sexual development
Sexual differentiation
Genetic sex.
The normal sex chromosome.
46xy will develop as a male.
46xx will develop as a female.
Gonadal sex
The resulting development of the gonad will create either a testis or an ovary
.
Phenotypic sex
development of the internal and external genitalia.
Brain sex ,
cerebral differentiation to a male or a female orientation.
Genetic sex
In the developing embryo with 46xy , the presence of the Y chromosome that determines that the undifferentiated gonad will
become a testis. Absence of Y chromosome will result in the developement of an ovary.
On the short arm of the Y chromosome is a region known as SRY gene, which is responsible for testicular development as it
produces a protein known as testicular determining factor (TDF) which directly influnces the undifferentiated gonad to become a
testis. When this occurs, the testis also produces Mullerian inhibitor that regress the Mullerian ducts.
The testis differentiated into two cell types, Lydig and Sertoli cells.
The Sertoli cells are responsible for the production of Mullerian inhibitor. The Leydig cells produce testosterone, which promotes
the development of Wolffian duct leading to the development of vas deferens, epididymis and seminal vesicles. The testosrterone
converted to dihydro-testosterone by the effect of 5a reductase, that lead to development of penis and scrotum.
The absence of Y chromosome means absence of testosterone and Mullerian inhibitor is not created that lead to regression of
Wolffian ducts but Mullerian ducts persist in the female lead to external female phenotype. See fig 1& 2.
Abnormal development
Anomalies due to genetic factors ( intersex )
Anomalies of external genital organs (ambiguous genitalia )
Anomalies of internal genital organs ( Mullerian Anomalies )
Intersex
is a general term used for a variety of conditions in which a person is born with a reproductive or sexual anatomy that
doesn't seem to fit the typical definitions of female or male.
Ambiguous genitalia
term used when intersex present.
Transsexualism
occur when a person strongly believes that he or she belong to the opposite sex.
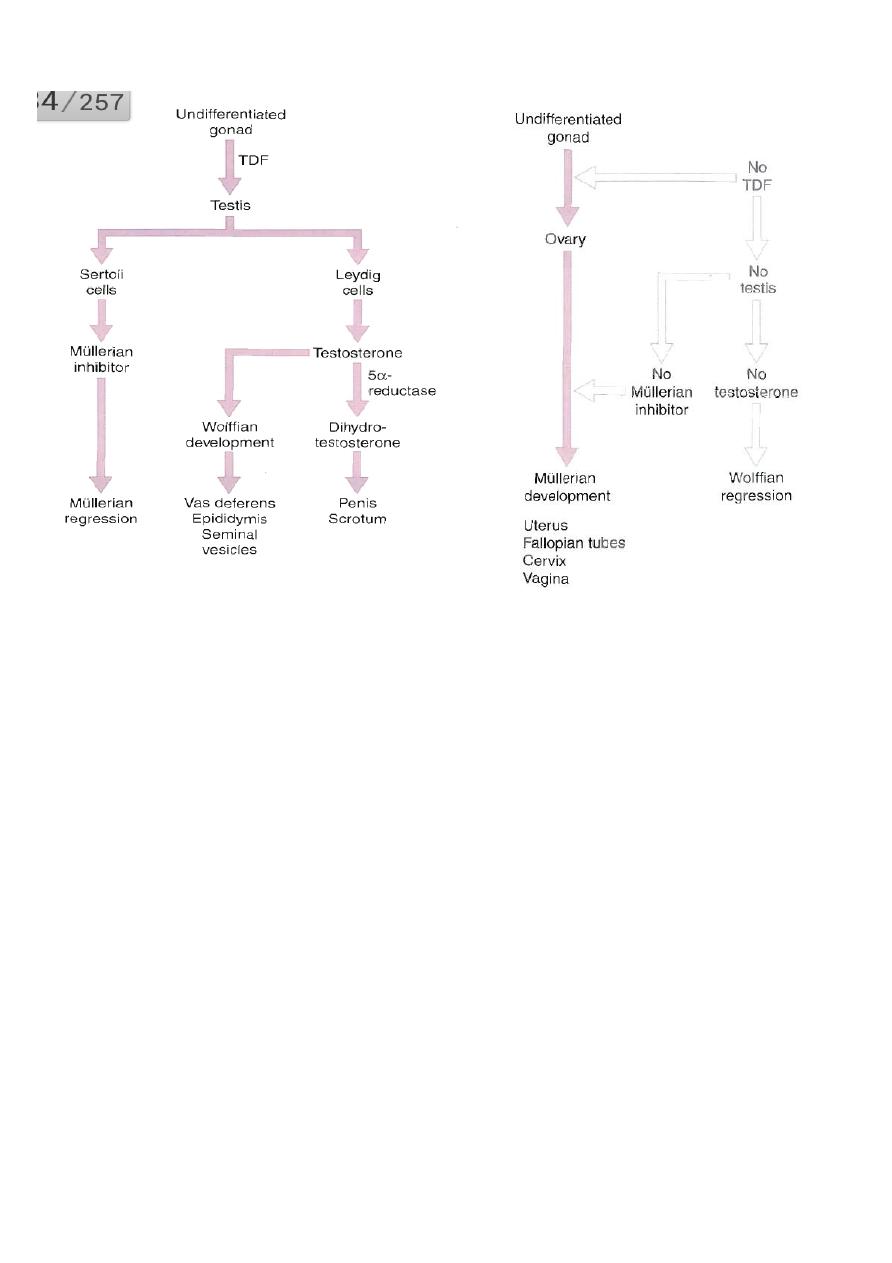
Fig.1 Male differentiation Fig.2 Female differentiation
Classification of intersexuality/ Clinical presentation.
1–virilization of genitically female fetus........female pseudo hermaphroditism.(CAH)
2–Incomplete musculinization of genitically male fetus.......male pseudo hermaphroditism (XY_female).
3–The presence of both ovarian and testicular tissue in the same individual.......true hermaphroditism.
4–Chromosomal abnormality.......mixed gonadal dysgenesis (45XO, 46 XY).
Aetiology
Most intersex conditions occur due to a genetic or enviromental disruption to the pathway of fetal sexual development. This
disruption can be due to
* Gonadal differentiation or development.
* Sex steroid production.
* Sex steroid conversion.
* Tissue utilization of sex steroid.
Incidence
A conservative estimate is that 1in 2000 children born will be affected by an intersex condition.
98% of affected babies are due to congenital adrenal hyperplasia (CAH).
Female
pseudo hermaphroditism
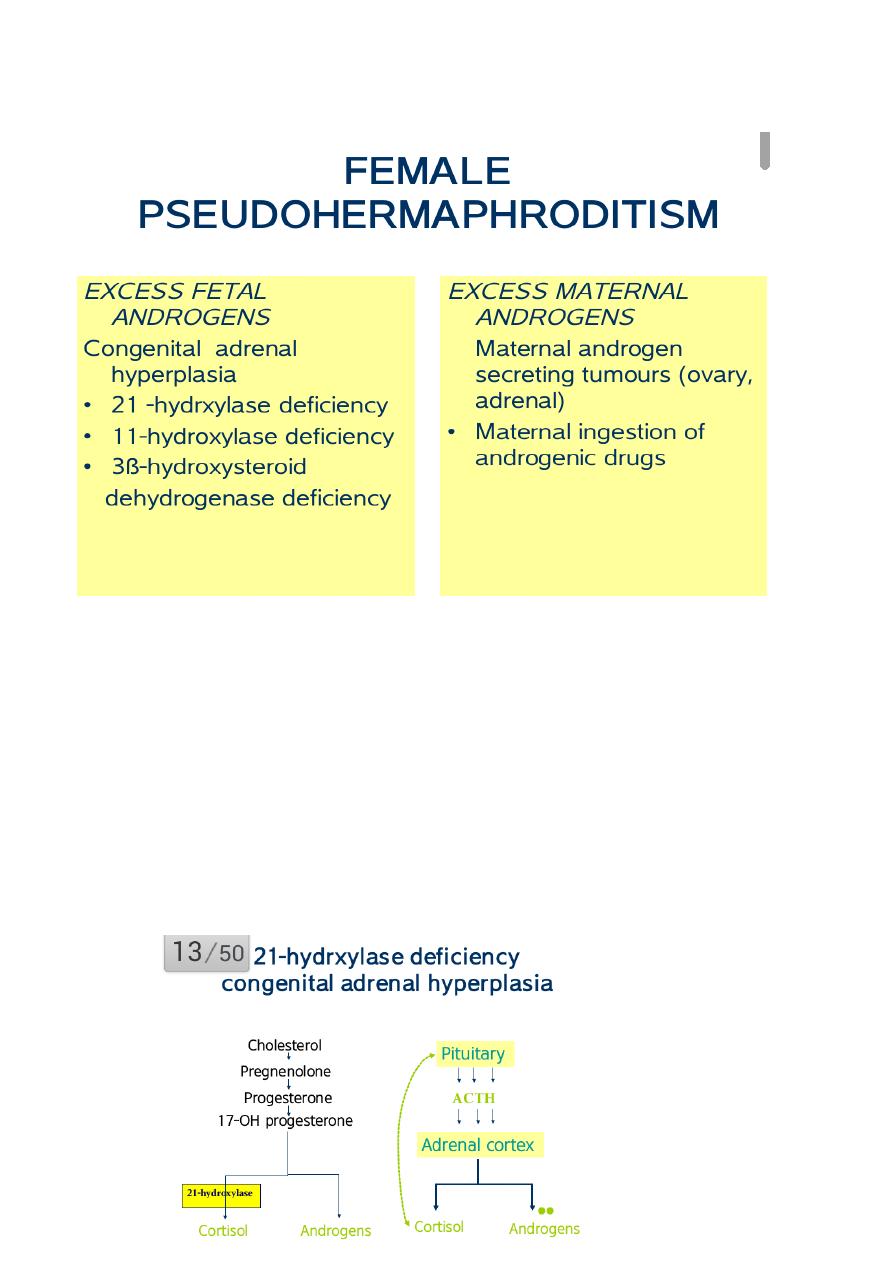
Congenital adrenal hyperplasia (CAH)
*Autosomal recessive.
*The commonest cause of genital ambiguity at birth.See fig.4
*21-hydroxylase deficincy is most common form.
*Salt wasting form may be lethal in neonate.
*Serum 17-hydroxyprogesterone (steroid precursors) increase.
In this condition, an enzyme defect in adrenl gland-usually 21-hydroxylase deficincy-prevent fetal adrenal gland from
pdoducing cortisol, means that the feedback mechanism on the hypothalamus lead to an elevation of ACTH which lead to
hyperplasia of adrenal gl......excessive production of steroid precursors......excessive amount of androgen. So the clinical
phenotype of CAH depend on the nature & severity of the enzyme deficiency.Fig.3
Epidemiology
Classic adrenal hyperplasia has a prevalence of 1 case/ 16,000 population.
CAH caused by 11-b hydroxylase deficiency account for 5-8% of all CAH cases.
Age
Classic CAH is recognized at birth or in early childhood.
Non classic adrenal hyperplasia is recognized at or after puberty because of oligomenorrhoea or virilizing signs in females.
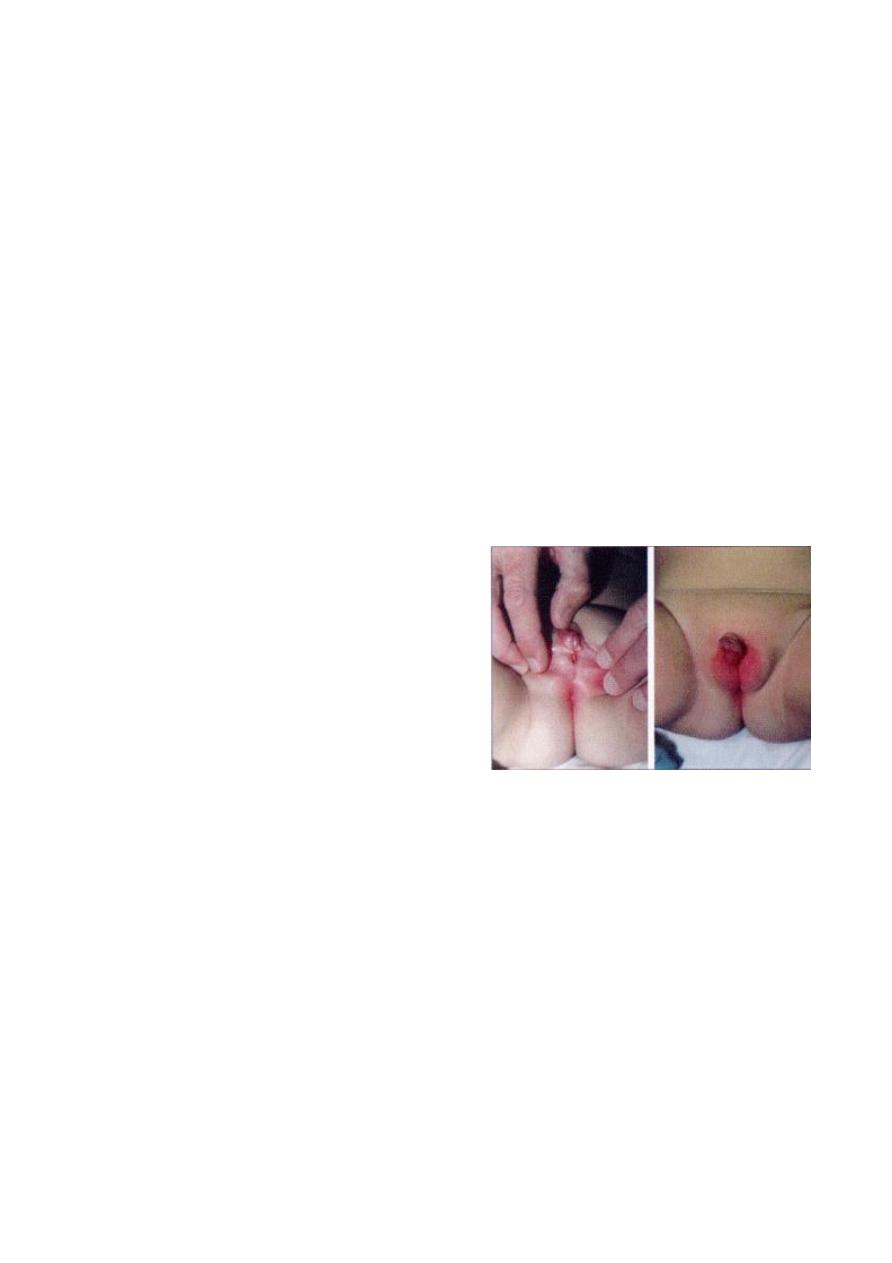
Affected female born with
-Enlargement of clitoris
-Excessive fusion of the genital fold obscure the vagina and urethra.
-thickdning and rugosity of the labia majora.
-Internal genital organs are present.
-Dangerous salt losing syndrome that may lead to death if not treated because the sever cortisol and aldosterone deficiencies
that result in salt wasting, hyponatremia, hyperkalemia, dehydration and hypotension.
Fig.4
ambiguous genitalia
Affected male
21-
hydroxylase deficincy is generally not identified in the neonatal period because the genitalia are normal. If the defect is
sever & result in salt wasting, these male neonates present at age of 1-4 weeks with failure to thrive, recurrent vomiting,
dehydration, hypotension and shock. This condition may be misdiagnosed as gastroenteritis or pyloric stenosis.
Investigation for suspected CAH
*Karyotype.
*17 alpha hydroxyprogesterone measurement.
*Electrolyte abnormality : Na, Cl, K.
*Pelvic ultrasound (internal genital organs).
Treatment of CAH
Medical control of the underlying disorder
.......Cortisol administration.
.......Correction of electrolyte disorder.
Surgical correction of the underlying anatomical abnormality
.....Reduction of the clitoris; amputation or reduction.
.....Clitoroplasty (best in the neonatal period).
.....Division of the fused labial fold (if thick better done well after puberty).
Prognosis for CAH
*Delayed puberty up to 2 years.
*Menstrual abnormality...oligo or amenorrhoea.
*Reduced fertility.
Drugs with Androgenic side effects ingested during pregnancy
Testosterone........Synthetic progestins.......Diazoxide......Minoxidil
Phenetoin sodium.....Streptomycin....Pencillamine.
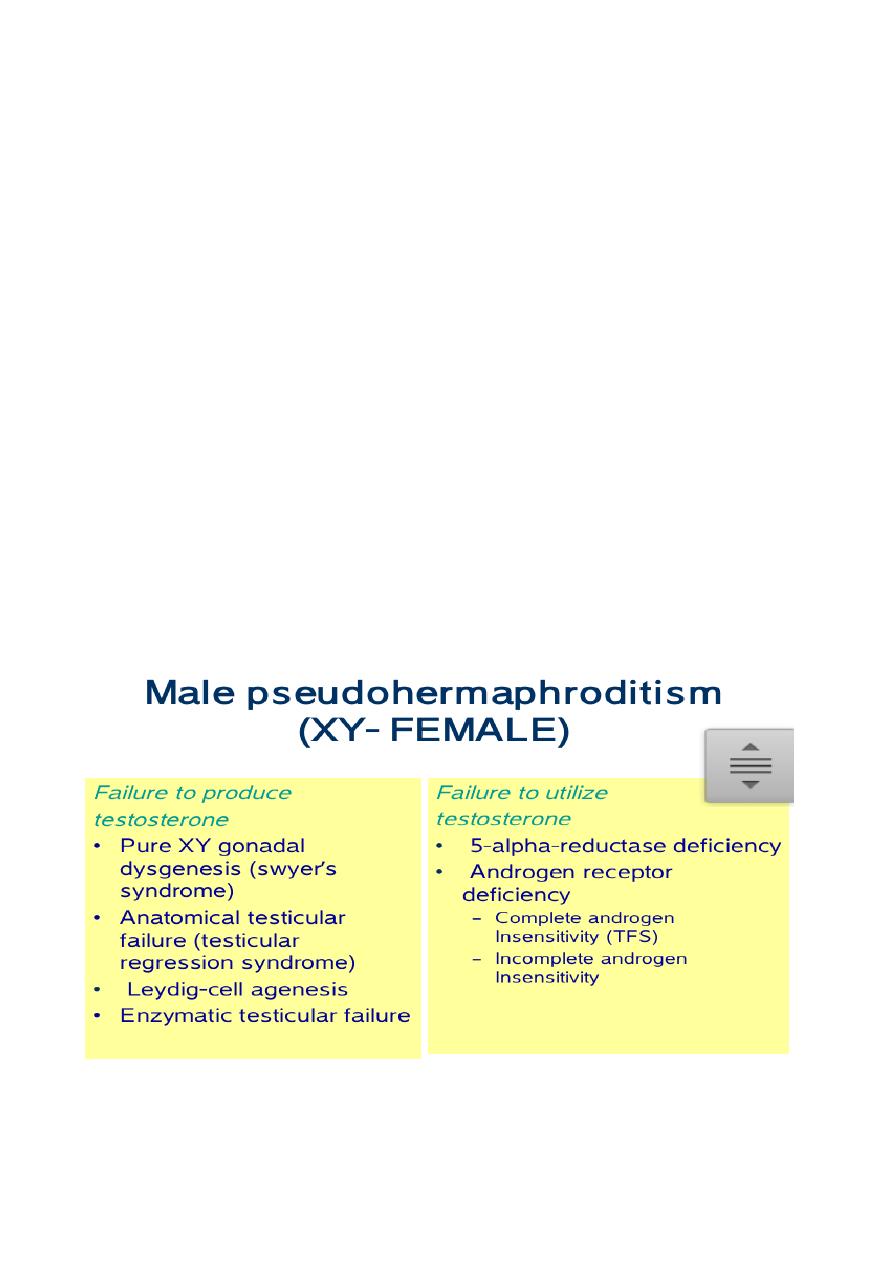
male pseudo hermaphroditism
XY female (46XY)
*Female phenotype.
*Primary amenorrhoea.
*breast development.
*Scanty or absent pubic and axillary hair.
*Absent uterus and tubes with short vagina.
*Un-descended testes (found in the abdomen, groin or labia majora).
*Diagnosis: female appearance with 46XY karyotype.
*5% risk of malignancy require gonadectomy.
*HRT(estrogen) treatment may be required.
*Surgery to elongate the vagina is seldom required.
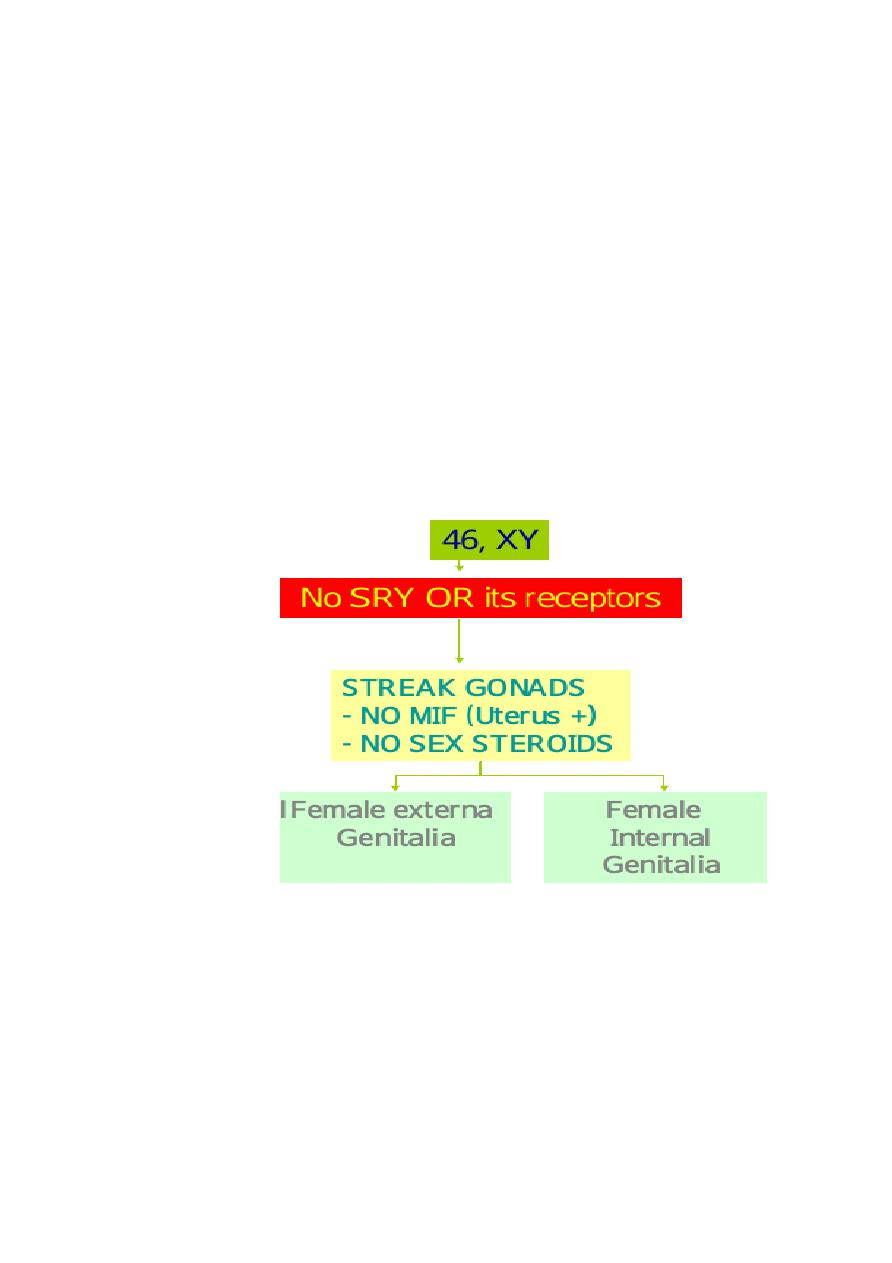
Pure XY gonadal dysgenesis (
Swyer's syndrome
)
Failure of testicular differentiation and development (no SRY or its receptors). Such patient has poor musculinization or none,
uterus (in contrast to other XY female), tubes and vagina are present.
Testicular feminization syndrome,
Now more appropiately called complete androgen insensitivity syndrome. This genetic disorder that makes XY fetus
insensitive ( unresponsive )to androgen. Instead, they are born looking externally like normal girl. Internally, there is a short
blind pouch of vagina & no uterus, fallopian tubes or ovaries. There are testes in the abdomen or the inquinal canal.
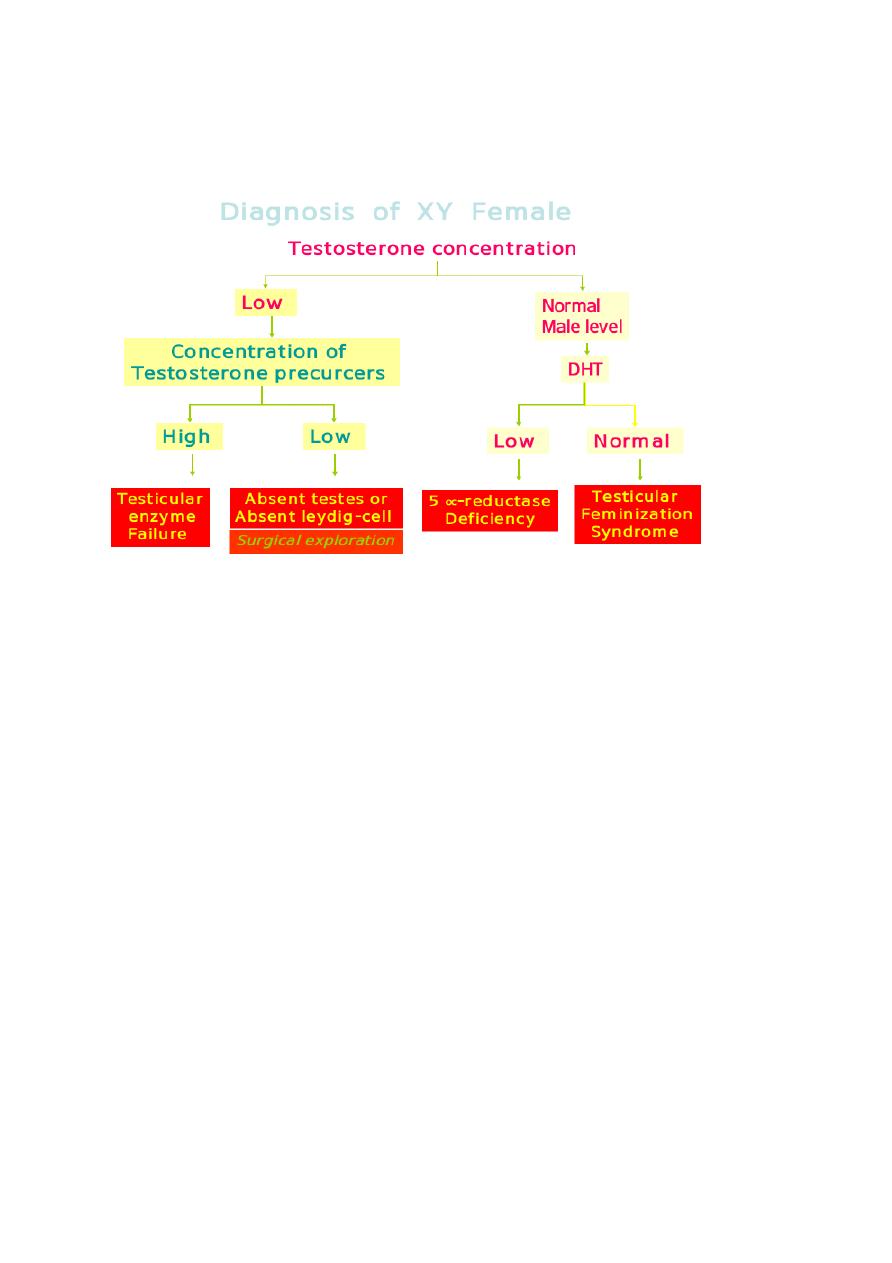
Diagnosis of XY female
Treatment
Removal of streak gonads during childhood (risk of malignancy in 5%).
Puberty replasement therapy (E. & P.) to produce secondary sexual development & mensis.
True hermaphroditism
The presence of both ovarian tissue & testicular tissue in one person so the patient present with various degree of sexual
ambiguity.
In the majority, uterus and vagina are present.
karyotype of 46 XX (57%), XY(13%) and XX/XY (30%).
Regarding gonadal distribution, ovotestis present on one side & ovary on the other or ovary in one side & testis
on the other.
Diagnosis by biopsy.
The sex chosen depend on functional capability of external genitalia.
Inappropriate organ should be removed.
mixed gonadal dysgenesis
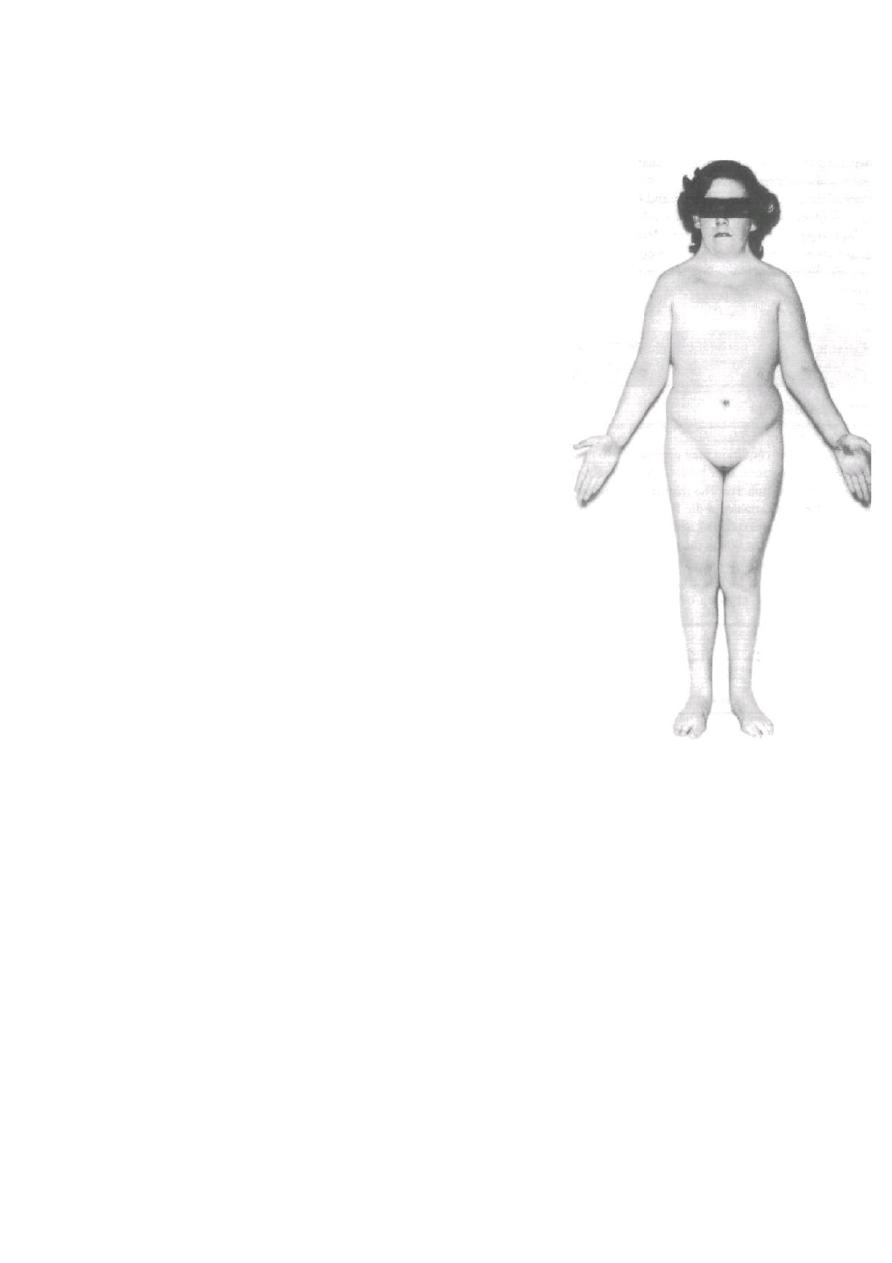
Turner's syndrome
Karyotype 45 XO
Phenotype female
Oedema of hand & feet.
Short stature.
Absent secondary sexual characteristics.
Wide carrying angle of the arms.
Webbed neck.
Broad chest with widely spaced nipples.
Associated medical problems as colour blindness, coarectation of aorta.
Streak ovaries (non functioning).
Normal internal genital organs.
Markedly elevated gonadotrophin (LH, FSH) &reduced estrogen.
The only anomaly commonly seen on ultrasound is cystic hygroma.
Fig.5
Treatment
–Induction of puberty by long treatment of estrogen
–Induction of menstruation by adding progesteron to estrogen after 2 years
of estrogen treatment.
-Growth hormone will increase growth & final adult height.
-Up to one third may have functioning ovaries, so pregnancy is possible.
Fig.5 Turner's syndrome
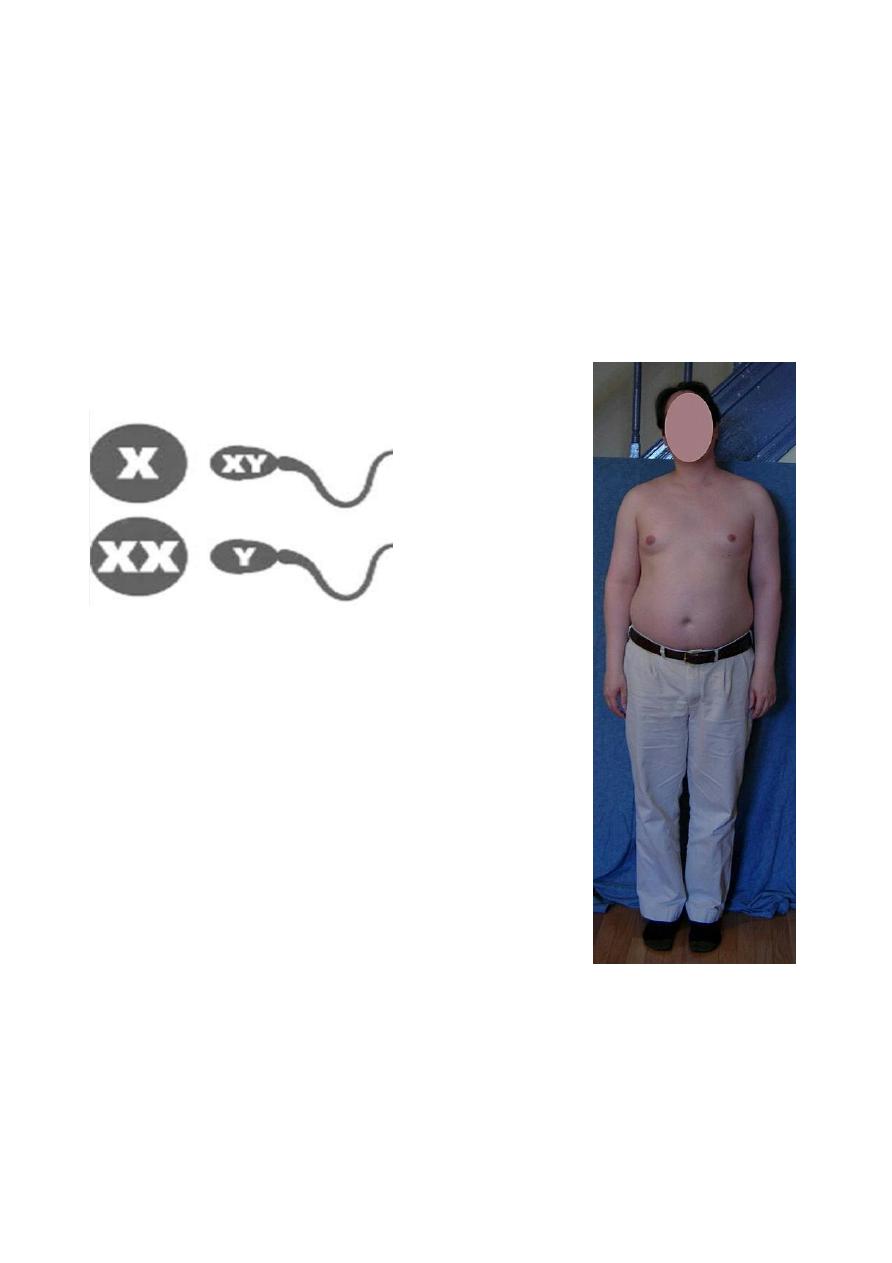
Klinefelter syndrome
(Seminiferous Tubule Dysgenesis).
*Karyotype of 47XXY.
*Appearance essentially is male.
*Scrotal testis, small, azoospermatic (infertile).
*Abnormal secondary sexual characteristics (tall, no facial hair)
*Affected male often infertile or reduced fertility.
*Leydig cells are present but testosterone is low normal, raised FSH, LH & estrogen cause gynaecomastia.
*Treat with androgens/ reduction mammoplasty/ cancer surveillance.See fig.6
Super female
*Karyotype is XXX.
*Mental subnormality.
*hypoplastic genitalia.
*Scanty menstruation or amenorrhoea. Fig.6
Klinefelter syndrome
Clinical presentation of intersexuality
# At birth............Ambiguous genitalia.
#During childhood......Heterosexual features.
#At adolesscence........Delayed or heterosexual puberty.

Ambiguous genitalia at birth
Genral guidelines
.........medical & social emergency
.........avoid immediate declaration of sex
.........proper counselling of the parents.
.........team management.
History: pregnancy & family history
Examination: general, abdominal, pelvic, external genitalia.
Investigation involve
.........rule out CAH
.........karyotype ( buccal smear, blood)
.........pelvic US & some time MRI.
........skin biobsy; fibroblast culture to measure 5 a reductase activity.
........laproscopy.
........gonadal biobsy ( laprotomy).
Treatment ..surgical considerations..
........phallic/ clitoral reduction if the assigned sex is female, before 3years of age.
........removal of intra abdominal gonads /streaks in new borns carrying Y chromosome.
.......vaginal construction / repair is better performed around puberty.
At adolescence
History
........primary amenorrhoea
.........ambiguous genitalia as in neglected CAH.
Examination
Investigation
Treatment
........cortisol replacement therapy & corrective surgery in CAH .
........corrective surgery in drug induced cliteromegally.
........in almost all other instances ( XY_female), whatever the diagnosis is to maintain the gender role as female.
........in some cases of enzymatic testicular defects or 5a reductase deficincy; some may seek to change the gender role.
.......gynecologists, endocrinologists, plastic surgeons, urologists &psychiatrists should be actively involved in the
management.

Dr.Amina Zakaria Al-tutunji
M.B.Ch.B, MD.
Obstetrics and Gynecology
College of medicine/ University of Mosul.
2016-2017
LEC4
Anomalies of internal genital organs ( Mullerian Anomalies )
Congenital Mullerian Anomalies
Epidemiology
Anatomic anomalies of the uterus are rare 0.5%
The exact aetiology is unknown, the mostly accepted 3 theories are: teratogenesis like diethylstilbestrol (DES.)
exposure, genetic inheritance & multifactorial expression.
Pathogenesis
All reproductive structures arise from the Mullerian system except the ovary ( which arise from genital ridge ) & the lower
one third of vagina ( which arise from urogenital diaphragm ). The anomalies can be
-lack of development (agenesis)
-incomplete develolment (hypoplasia )
-incomplete canalization (atrasia )
-complete seperate development.
**Uterine anomalies
1---
Absence of the uterus;
uterus is absent or rudimentary & non functioning.there are 2 conditions present with absent
uterus.
1.Rokitansky syndrome
.....46XX
.....absent uterus & vagina.
.....normal ovarian function.
.....primary amenorrhoea
2.Androgen insensitivity syndrome
.....XY
.....absent uterus
.....blind end of lower vagina
.....absent axillary &pubic hair.
.....gonads are testis found in abdomen or groin & require removal.
*** No treatment is available for such uterine anomalies only uterine transplant.
2---
Uterine fusion anomalies
Uterine didelphys (complete failure of fusion of Mullerian ducts) (8%.)
Bicornuate uterus ( 26% ).
...complete to the internal os
...partial
...arcuate

Unicornuate uterus (10% )
With a rudimentary horn....with a communicating endometrial cavity
....with a non communicating cavity
....with no cavity
Without any rudimentary horn.
Septate uterus ( 35% )
....with a complete septum
....with an incomplete septum.
Fig.1 uterine anomalies
Clinical Manifestations
* Asymptomatic
*Dysmenorrhoea (rudmentary horn)
*Dyspareunia
*Cyclic & non cyclic pelvic pain
*Infertility
*Recurrent miscarriage
*Malpresentation
*Preterm labour
*Rarely, ectopic pregnancy in rudimentary horn, may presented later than other type with rupture & sever haemorrhage.
Diagnostic evaluation
Pelvic US, CT,MRI, sonohistogram, HSG, hysteroscopy & laproscopy.
There is an increased incidence of renal anomalies (unilateral renal agenesis, horseshoe kidneys or irrigularities in the
collecting system ).
Treatment
Many require no treatment.
Uterine septa can be excised with hysteroscopy.
If pregnancy occur in case of bicornuate uterus, the patient will require delivary via CS to decrease risk of rupture.
**Vaginal anomalies
1--Absent vagina
Usually occur with absent uterus in Rokitansky syndrome (rarely occur with the presence of uterus). Present as primary
amenorrhoea . US required for diagnosis. If patient abnormality discovered after marriage, an operation to create a new vagina
(William operation). More extensive one is McIndoe operation (a space is dissected between the rectum & bladder & urethra,
this cavity is lined with a skin graft from the thigh.
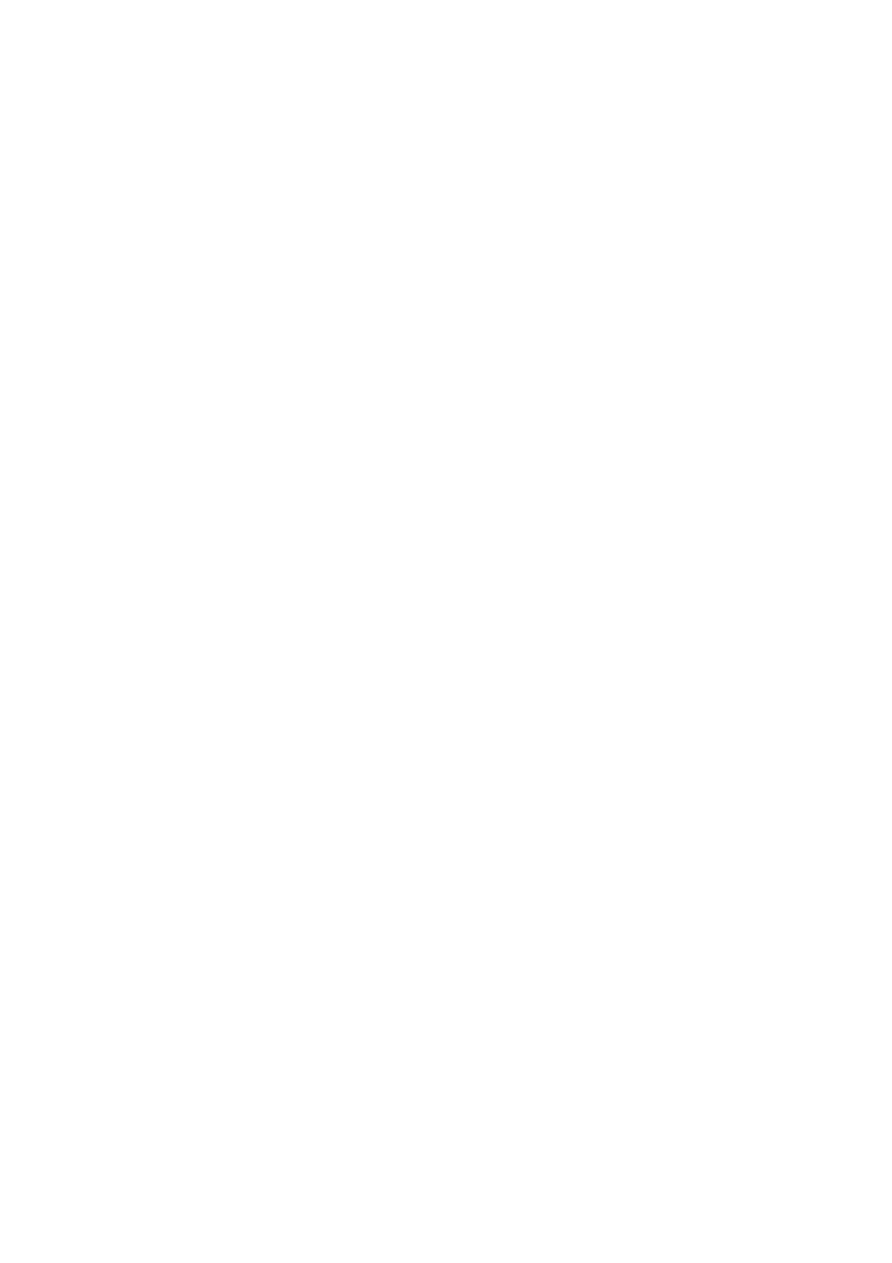
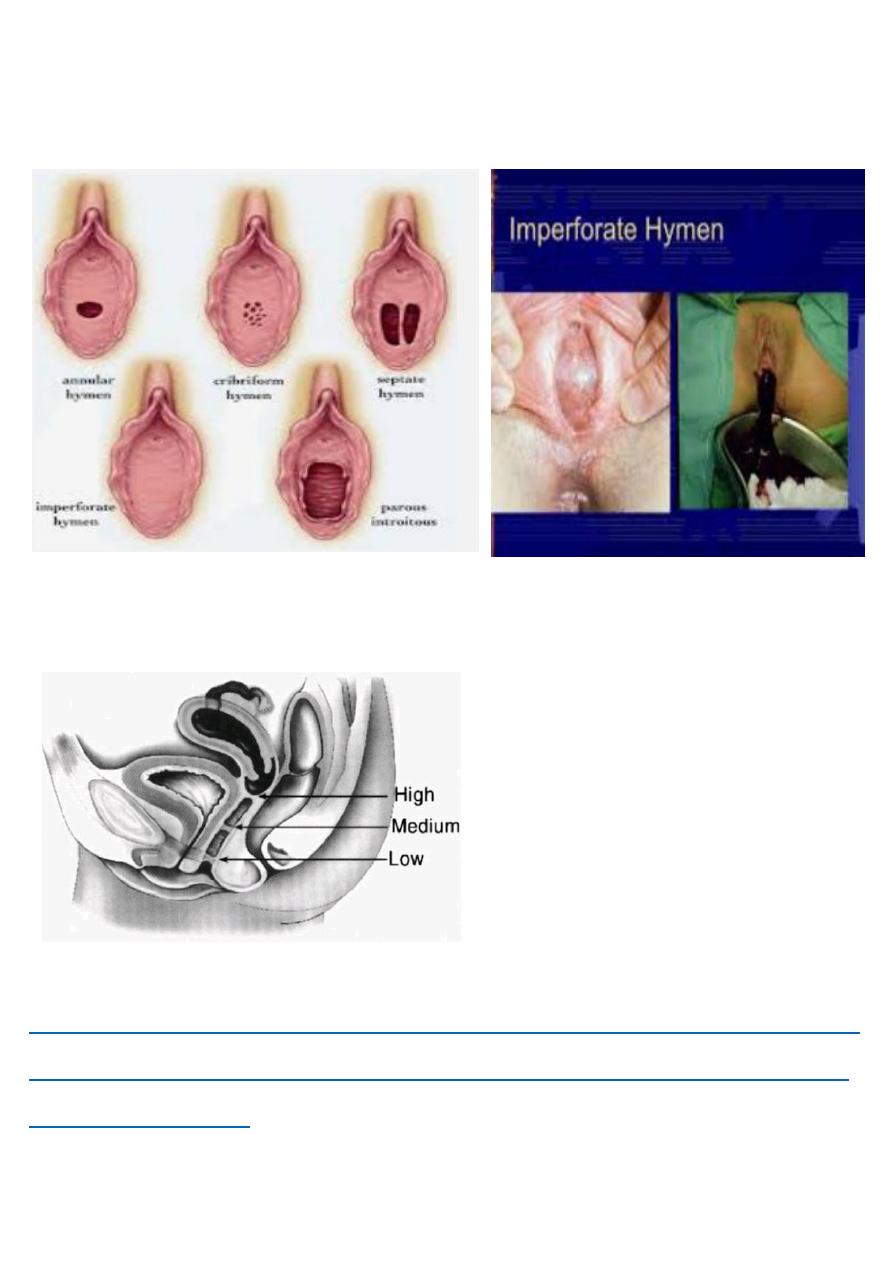
2--Vaginal atresia
Is a condition in which the vagina is abnormally closed. The main cause can either be complete vaginal hypoplasia or vaginal
obstruction, often caused by an imperforate hymen (fig.2,3) or less commonly a transverse vaginal septum (fig.4).. As the
uterus is often present, the menstrual blood after puberty will be retaied inside, a condition called cryptomenorrhoea. The
vagina become distended with blood (haematocolpos) the blood become thick & chocolate after slow absorption of fluid. Any
leaking into the peritoneal cavity may cause endometeriosis.
It present in a female between 14-16y as
*primary amenorrhoea.
*cyclical discomfort & abdominal pain.
*retention of urine may occur.
Examination
*an abdominal mass may be felt above pubic symphysis due to collection of blood within the uterus (hematometra)
*vulval inspection; a bulging membrane may be seen & appear purple or red.
*rectal examination; reveal a mass at the vagina.
Diagnosis
*US
*Laproscopy
*Laprotomy
Treatment
Drinage best by excision of membrane but there is a high risk of infection that need antibiotic cover before & after drinage.
Prognosis
Is good if the distention only involve the vagina, not the uterus nor the tubes.
There is a risk of obstruction of fimbria, endometriosis & infertility.
There may be vaginal stenosis & dyspareunia later on.
3--Vaginal septum
There is a longitudinal anteroposterior septum.
**Fallopian tube anomalies
Absent tubes or malformed.
**Gonadal anomalies
(gonadal dysgenesis)
Cervical anomalies (congenital elongation of the cervix that may require excision.
Fig.2 types of hymen Fig.3
imperforate hymen
Fig.4
vaginal septum
https://www.muhadharaty.com/lecture/13269/Abnormal-sexual-development/%D
8%AF--%D8%A7%D9%85%D9%86%D8%A9-%D8%B2%D9%83%D8%B1