Congenital Anomalies
of
The Upper Urinary Tract
Dr. Ali Wafaa Al-Wefy M.D.
Urology Specialist

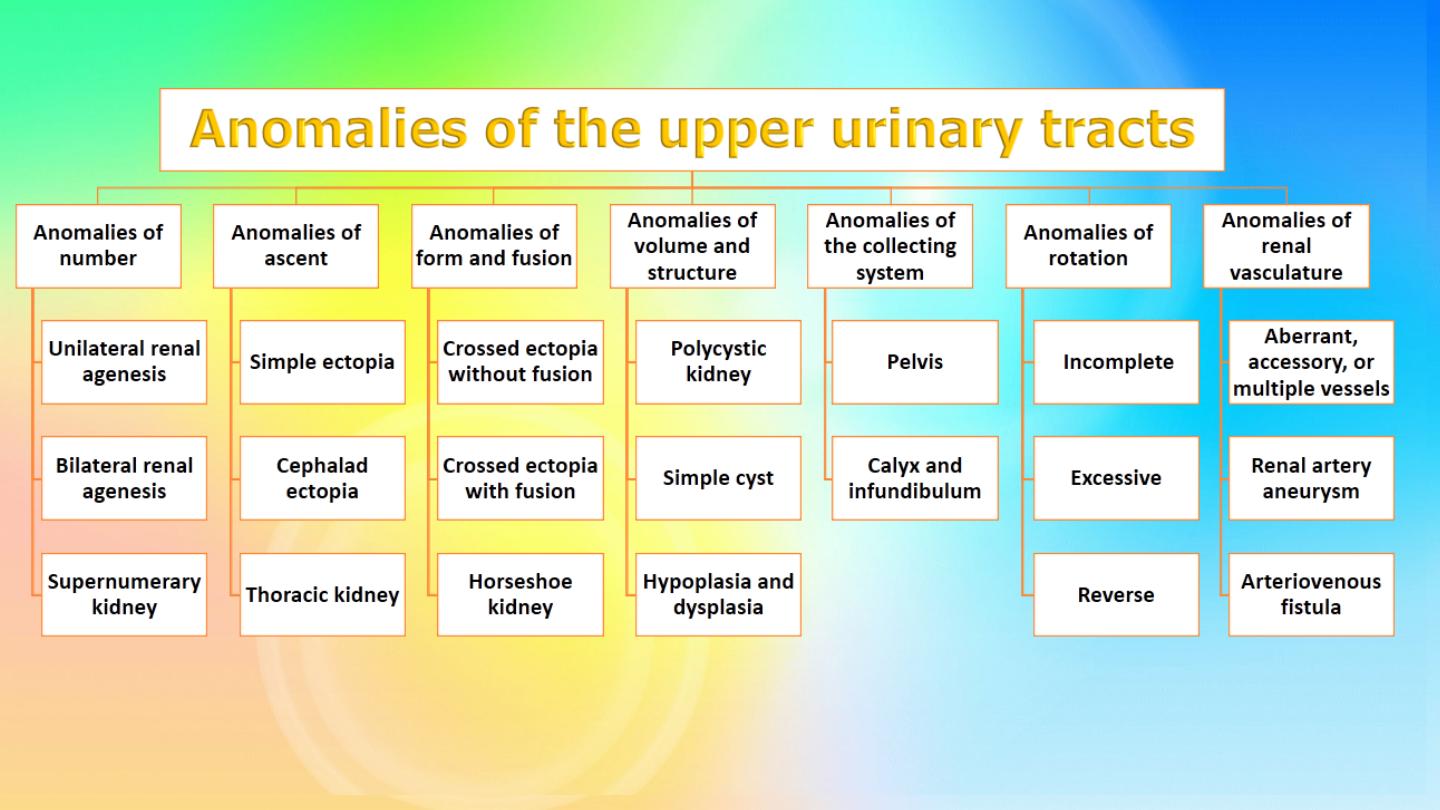
Congenital anomalies of the upper
urinary tract comprise a group of
abnormalities, ranging from complete
a b s e n c e t o a b e r r a n t l o c a t i o n ,
orientation, and shape of the kidney as
well as aberrations of the collecting
system and blood supply.

Surgical anatomy
The parenchyma of each kidney usually drains into
seven calyces, three upper, two middle and two lower
calyces. Each of the three segments represents an
anatomically distinct unit with its own blood supply.
The kidney and renal pelvis normally rotate 90 degrees
ventromedially ( toward midline) as they leave the
true pelvis during beginning of ascent at 6
th
week of
gestation so that the calyces point laterally and the
pelvis faces medially. When this alignment is not
exact, the condition is known as malrotation
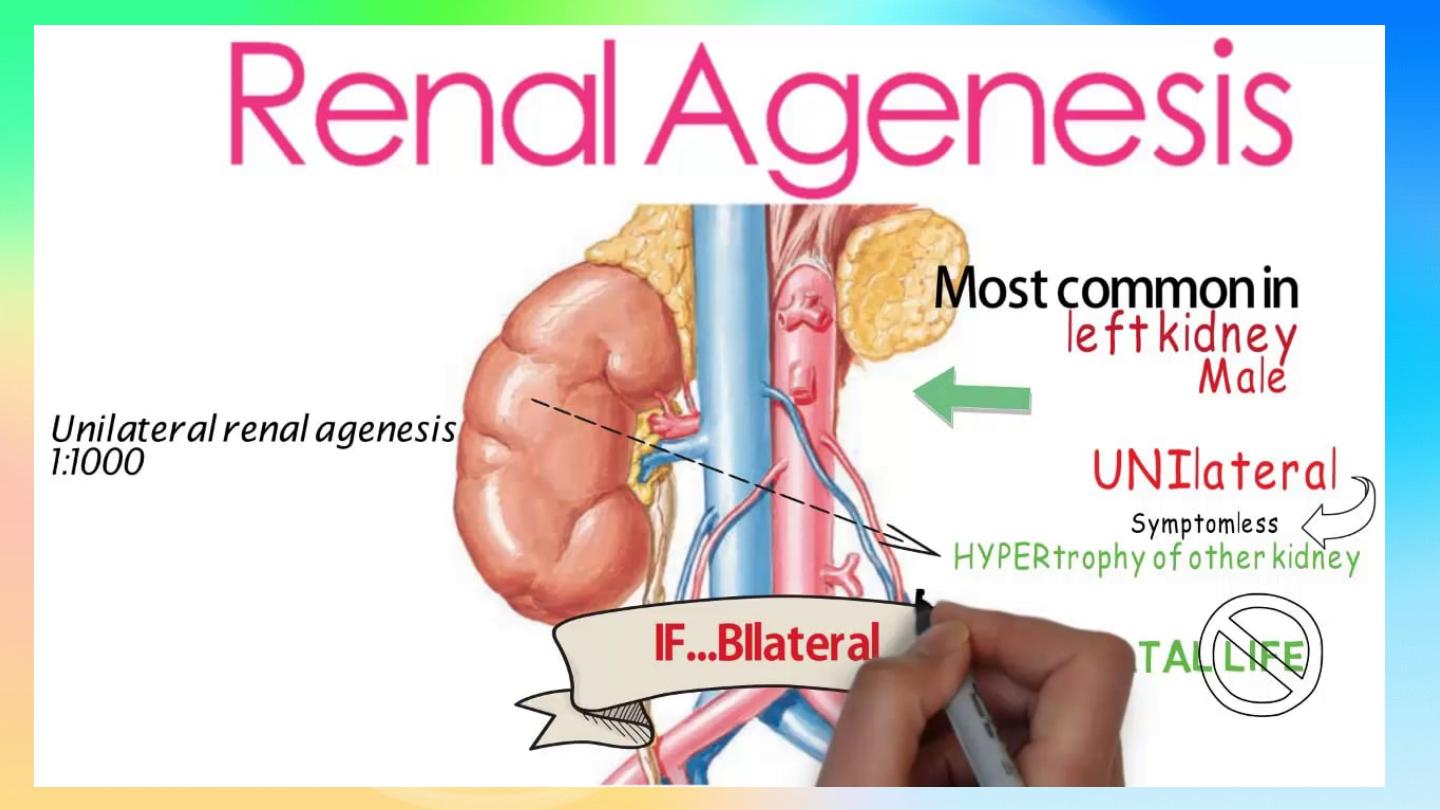
Unilateral Renal Agenesis (URA)
Bilateral agenesis:
rare, incompatible with life
Found accidentally, more frequently on the left side.
Ipsilateral adrenal agenesis is rarely encountered with URA
Symptoms:
Asymptomatic
Diagnosis:
U/S or IVU,CT scan: absent kidney on that side +
compensatory hypertrophy of the contralateral kidney
Treatment:
no specific treatment
Supernumerary Kidney
The supernumerary kidney is a distinct mass of
renal parenchyma that may be either completely
separate or only loosely attached to the major
kidney on the ipsilateral side.
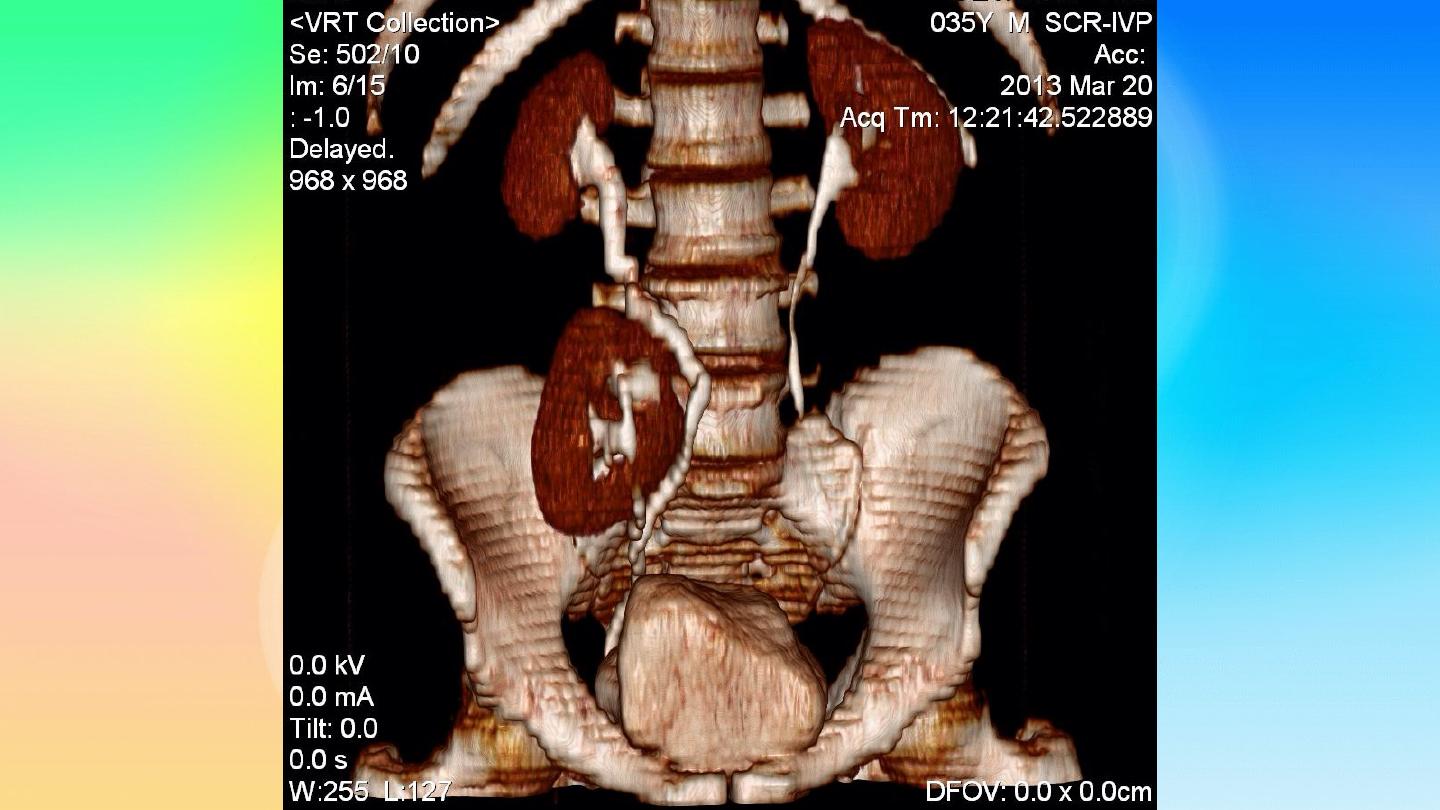
ANOMALIES OF ASCENT
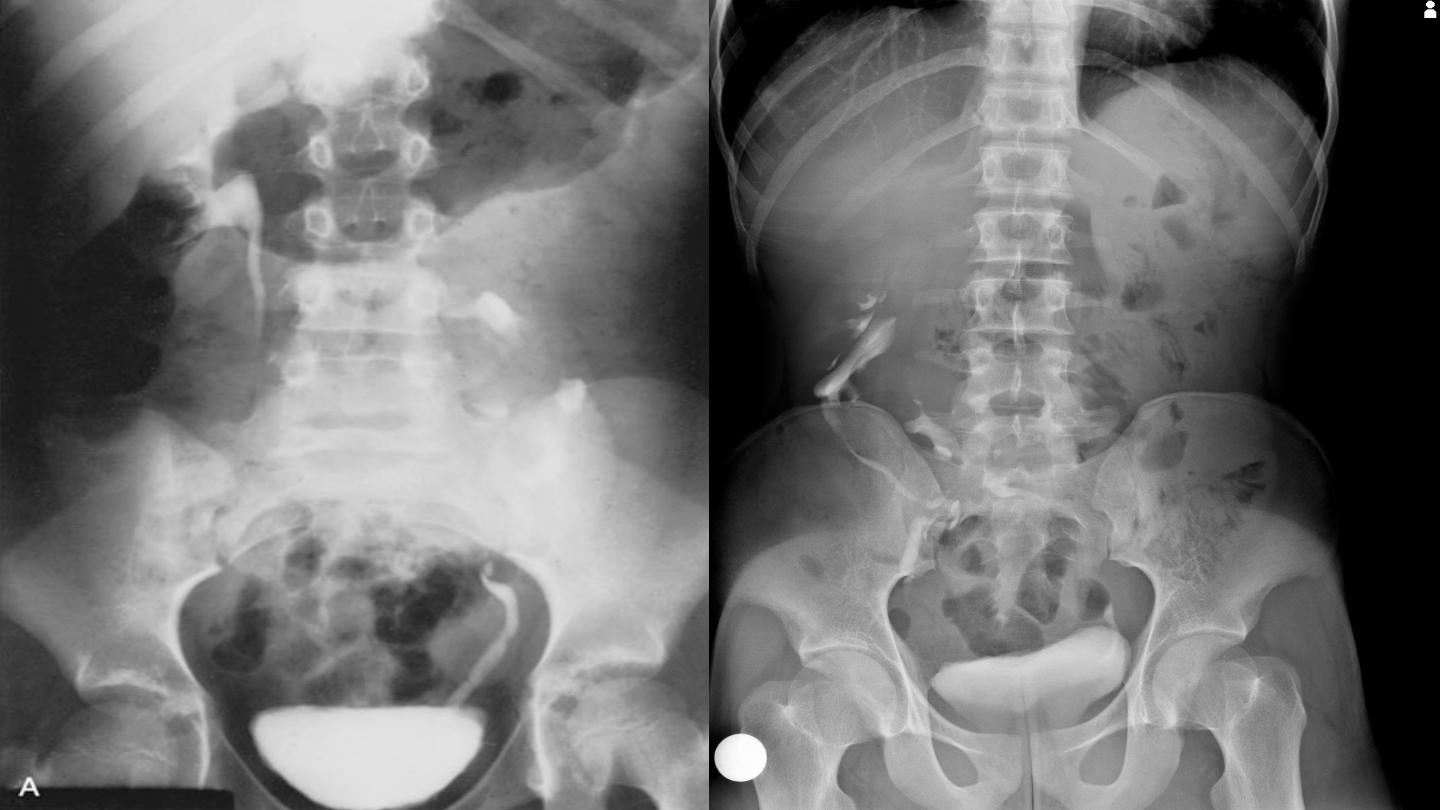
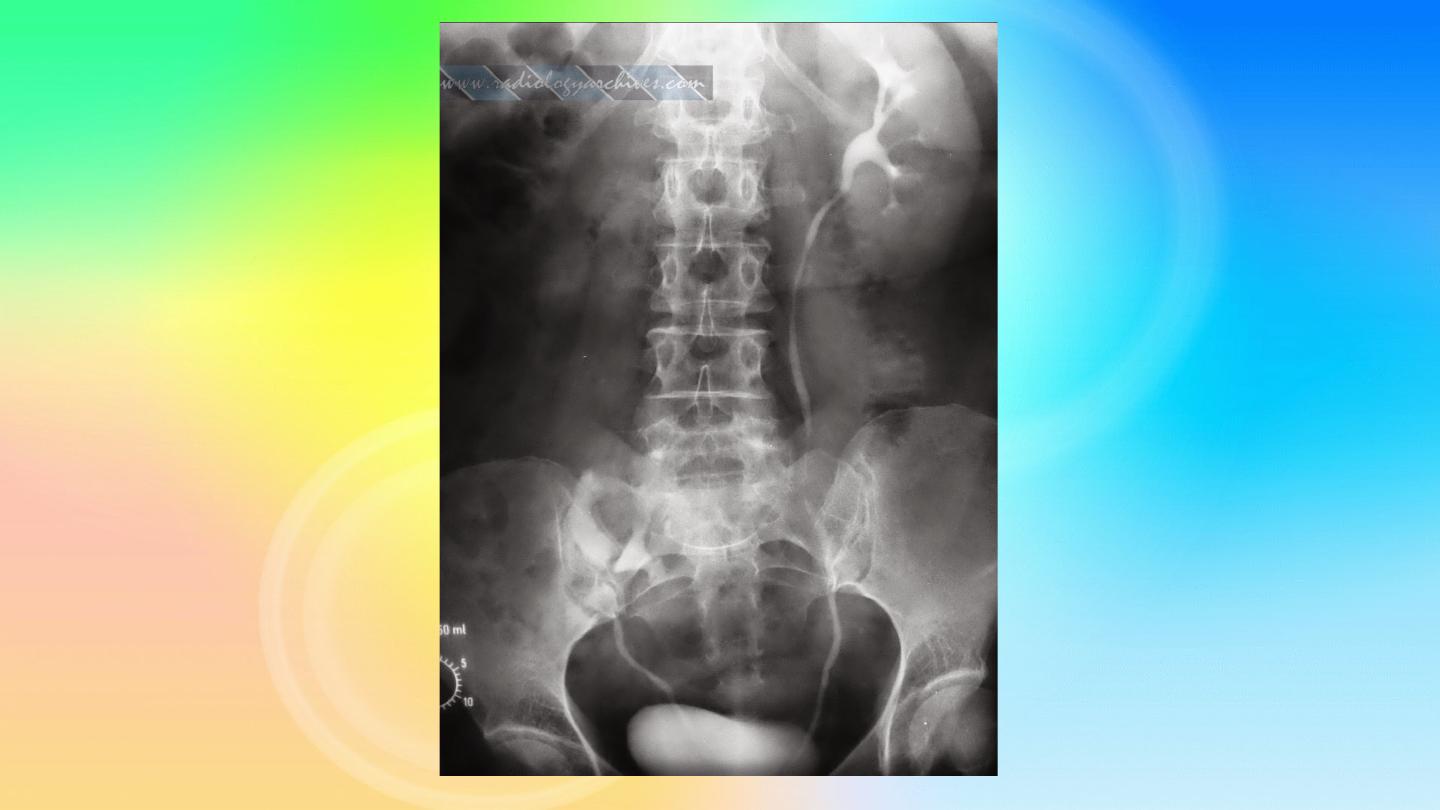
1. Simple Renal Ectopia
When the mature kidney fails to reach its normal
location in the “renal” fossa, the condition is
known as renal ectopia. The term is derived
from the Greek words ek (“out”) and topos
(“place”) and literally means “
out of place
.”

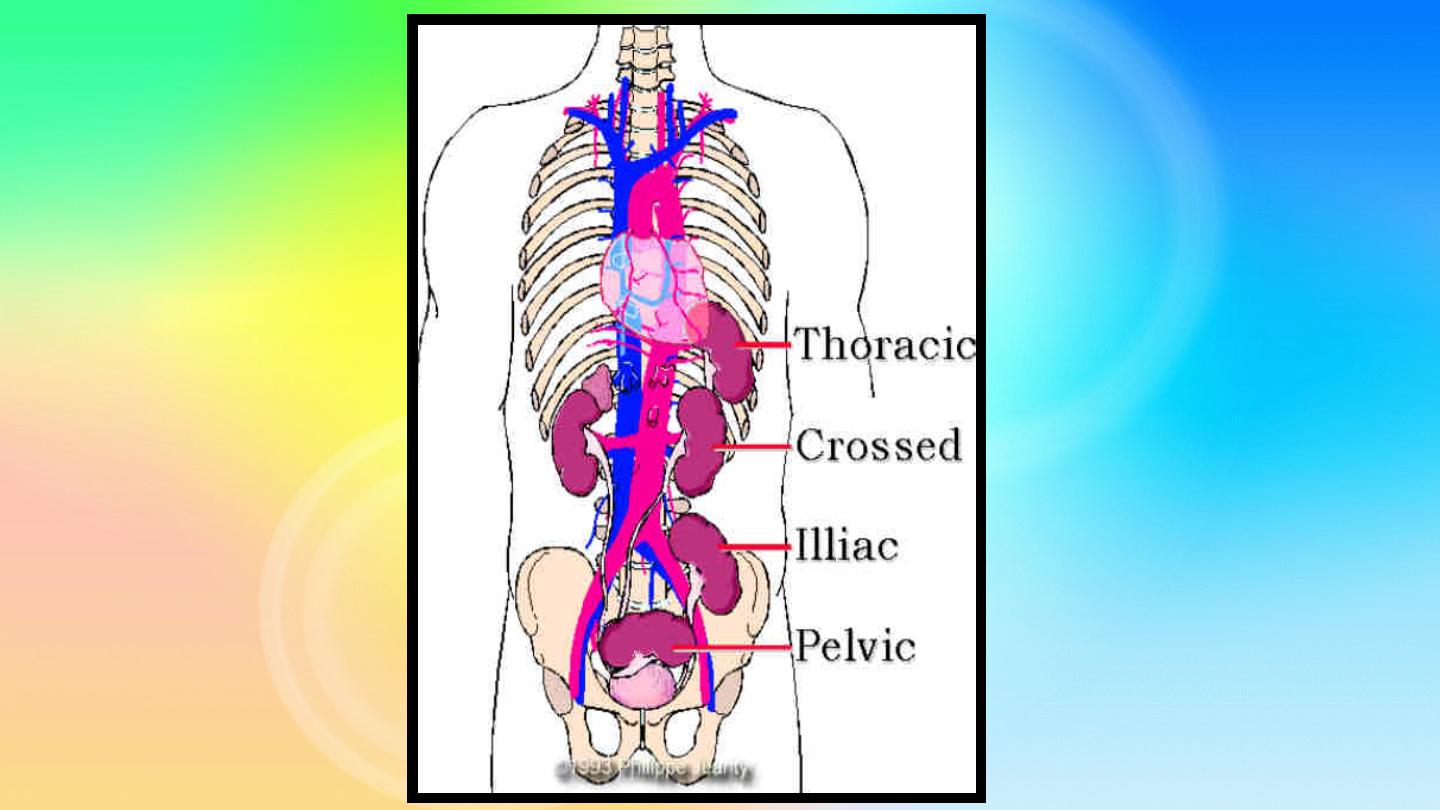
An
ectopic kidney
can be found in one of the following
positions:
pelvic, iliac, abdominal, thoracic, and crossed.
The renal pelvis is usually
anterior
(instead of medial) to
the parenchyma, because the kidney has
incompletely
rotated
. As a result, some of ectopic kidneys have a
hydronephrotic collecting system due to
obstruction
of the
ureteropelvic or the ureterovesical junction.
Associated Anomalies:
The incidence of contralateral
agenesis appears to be rather high.
Hydronephrosis
secondary to
obstruction or reflux
may be seen in the
contralateral kidney
Clinical features:
Most ectopic kidneys are
asymptomatic
Diagnosis:
U/S, IVU, CT scan
Prognosis:
The ectopic kidney is no more susceptible
to disease than the normally positioned kidney
except for the development of
hydronephrosis or
urinary calculus
formation or the presence of
ectopic ureter.
2. Cephalad Renal Ectopia
The kidney may be positioned more cranial than
normal.
3. Thoracic Kidney
Intrathoracic ectopia denotes either partial or a
complete protrusion of the kidney above the level
of the diaphragm into the posterior mediastinum
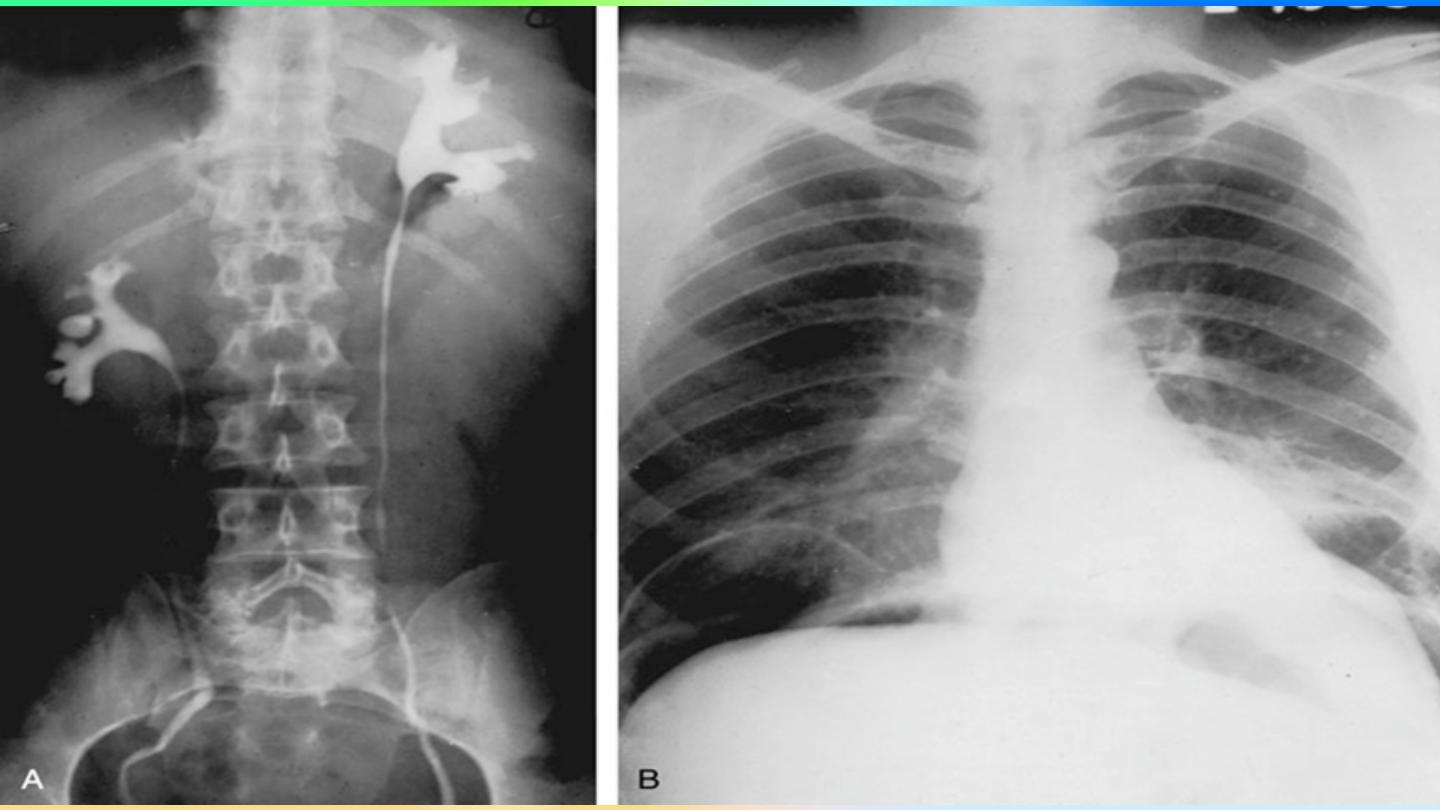
ANOMALIES OF FORM AND FUSION
Crossed Renal Ectopia With and Without Fusion
When a kidney is located on the side opposite from that in
which its ureter inserts into the bladder, the condition is known
as crossed ectopia.
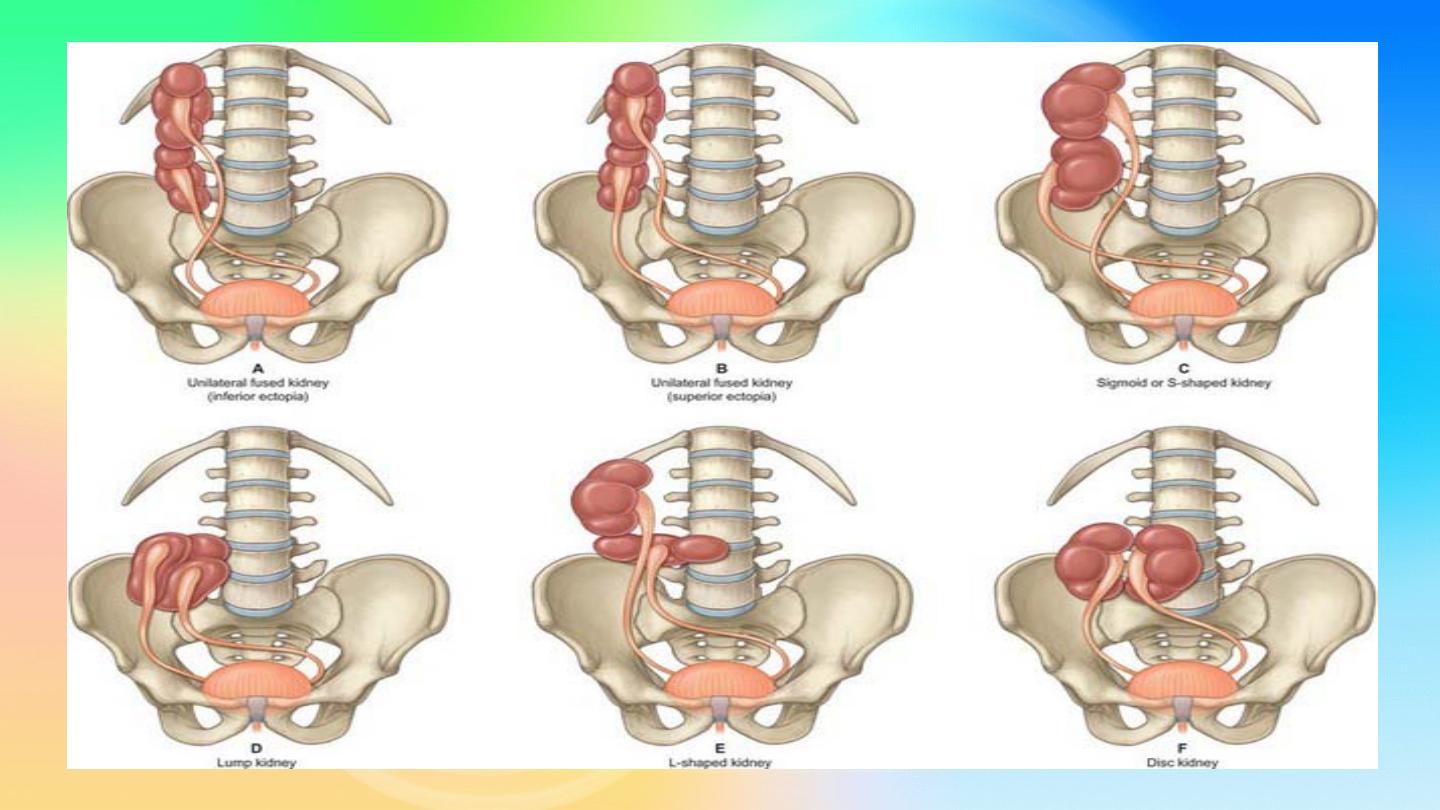
Types of fused ectopia
A. Inferior Ectopic Kidney:
The upper pole of the crossed
kidney is attached to the inferior aspect of the normally
positioned mate.
B. Superior Ectopic Kidney:
crossed ectopic kidney that lies
superior to the normal kidney.
C. Sigmoid, or S-Shaped, Kidney:
they face in opposite
directions from one another
D. Cake or Lump Kidney:
fusion has taken place over a wide
margin
E. L-Shaped Kidney:
crossed kidney assumes a transverse
position.
F. Disc Kidney:
joined at the medial borders of each pole
Horseshoe Kidney
•
probably the most common of all renal fusion anomalies.
•
The anomaly consists of two distinct renal masses lying
vertically on either side of the midline and connected at
their respective lower poles by a parenchymatous or
fibrous
isthmus
that crosses the midplane of the body.
•
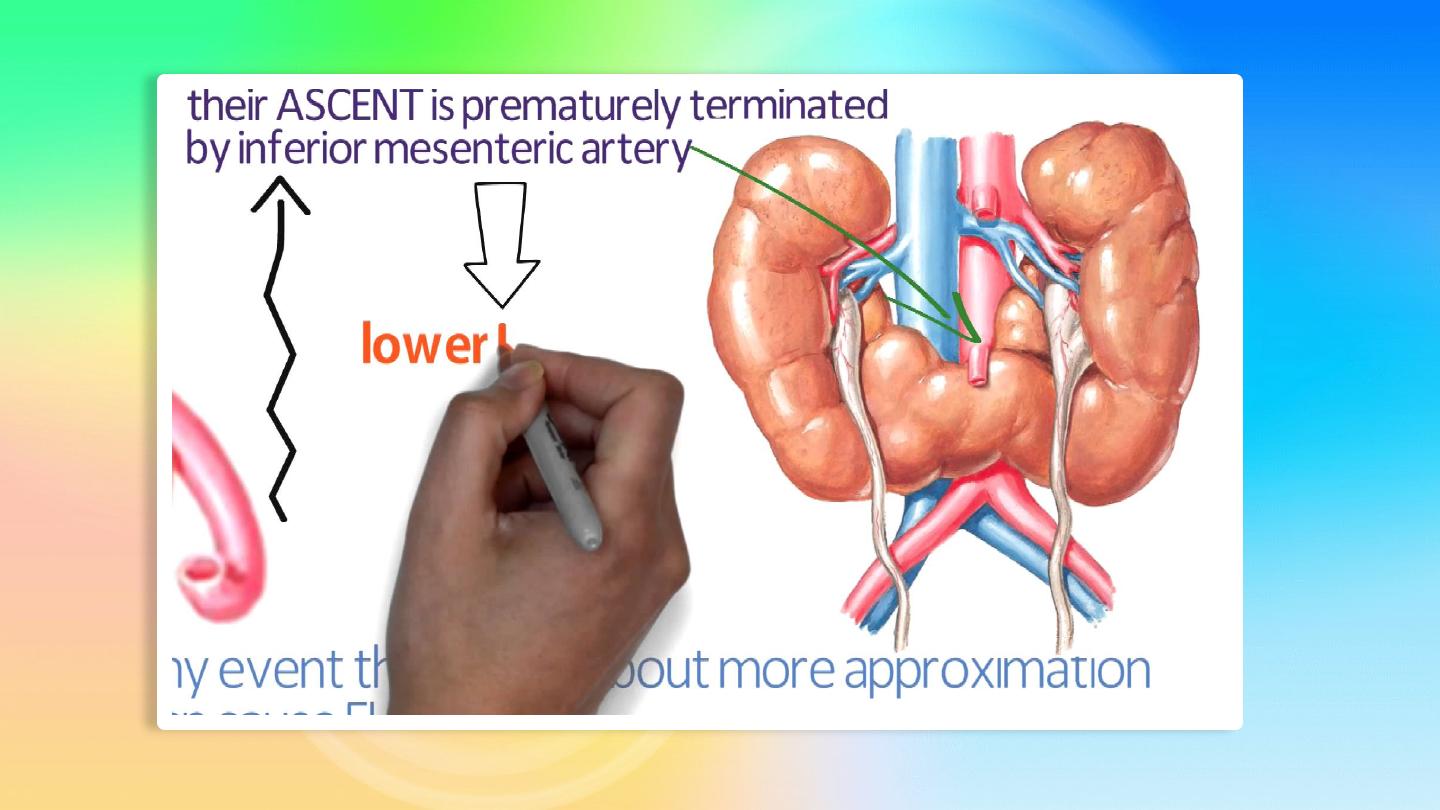
Fusion of the renal masses early in embryonic life, so its
ascent will be impeded by
inferior mesenteric artery
.
•
The kidneys are
low located at the level of the 4
th
lumbar
vertebrae, malrotated and pelves lie anteriorly
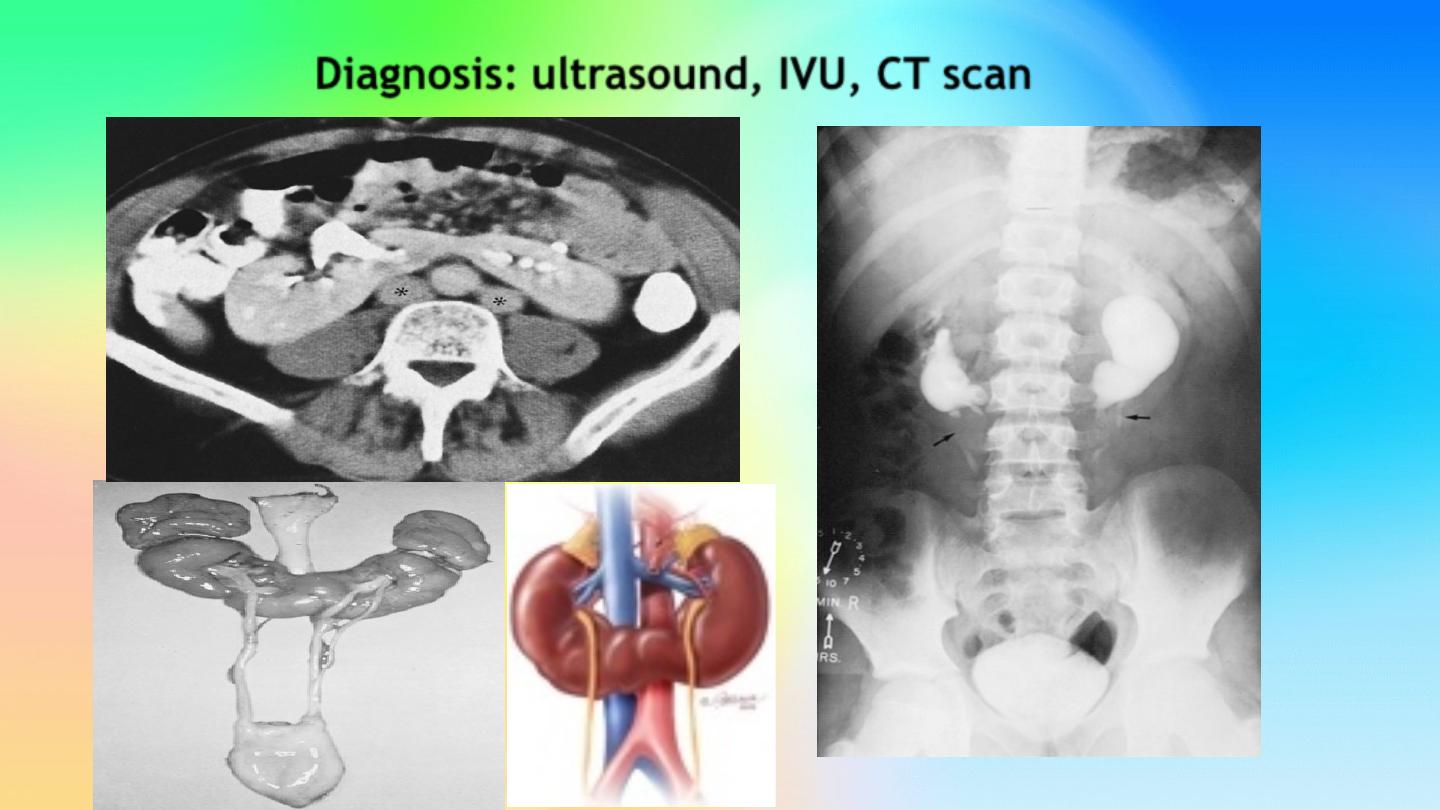
Diagnosis:
ultrasound, IVU, CT scan
Symptoms:
When present, they are related to
complications like
hydronephrosis, infection, or
calculus
formation due to ureteric angulation or
obstruction with impaired urine drainage
Treatment:
Medical:
pain relief and antibiotics to control infection
Surgical:
if present, stone removal, Pelviureteric
junction obstruction correction.
Cystic disease of the kidneys
Polycystic kidney disease :
The kidney is one of the most common sites in the body
for cysts
Two types:
•
AUTOSOMAL RECESSIVE ("INFANTILE") POLYCYSTIC
KIDNEY DISEASE
•
AUTOSOMAL DOMINANT ("ADULT") POLYCYSTIC KIDNEY
DISEASE
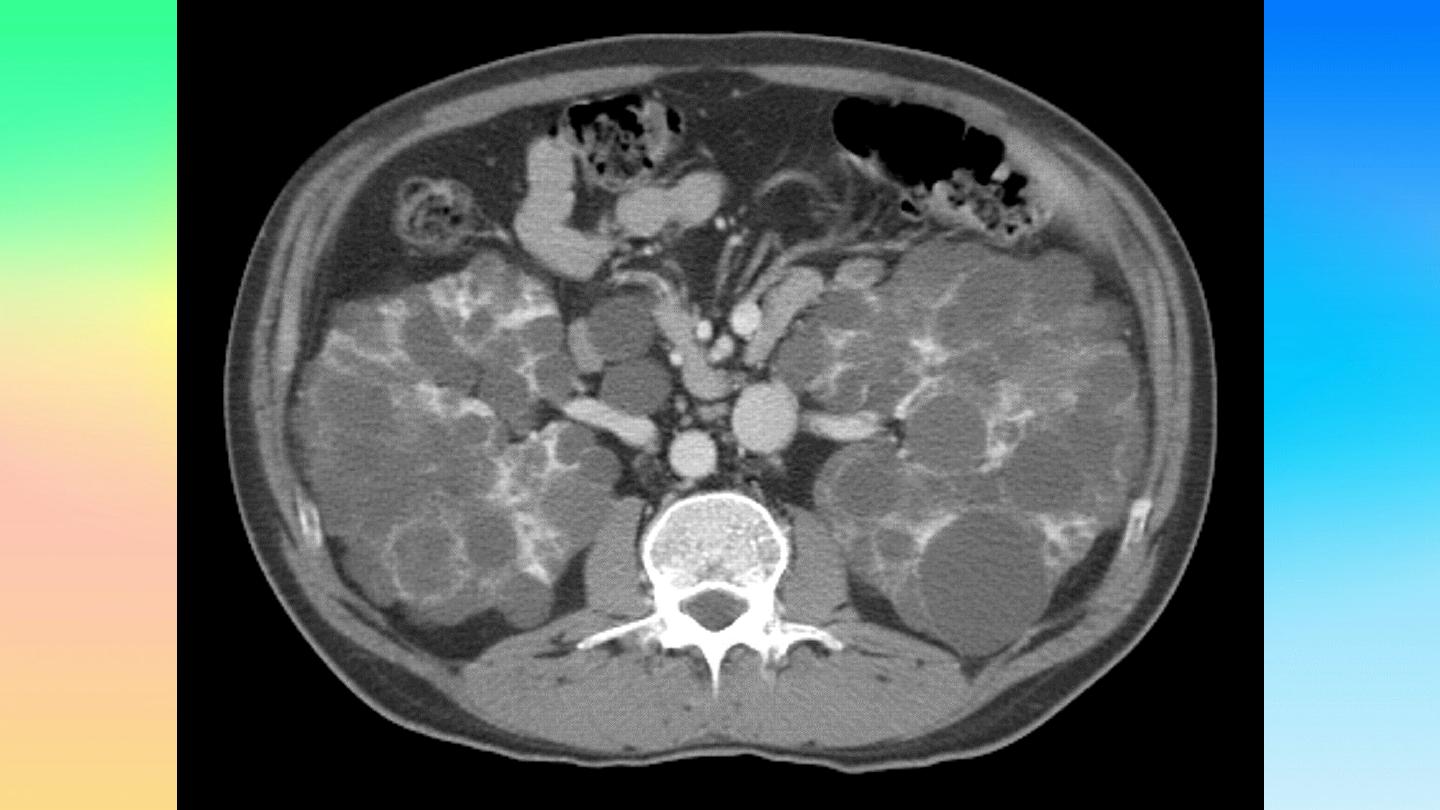
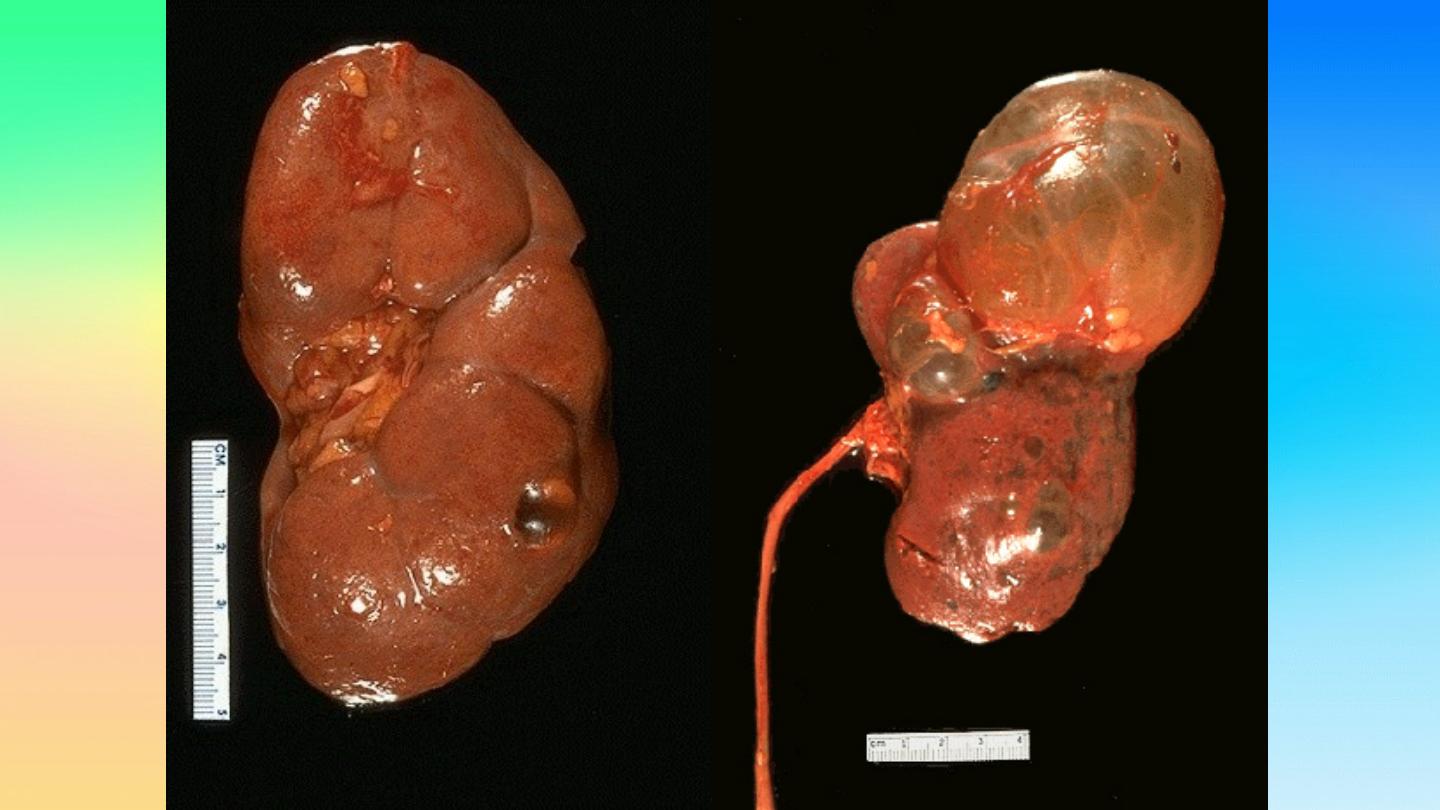
Autosomal dominant polycystic kidney
disease
•
Autosomal dominant, transmitted by either parents,
50%
of offspring affected.
•
Both kidneys replaced by large no. of cysts of
variable size which make the kidney of large size.
•
15% associated with
cystic disease of liver, lung,
pancreas or spleen.
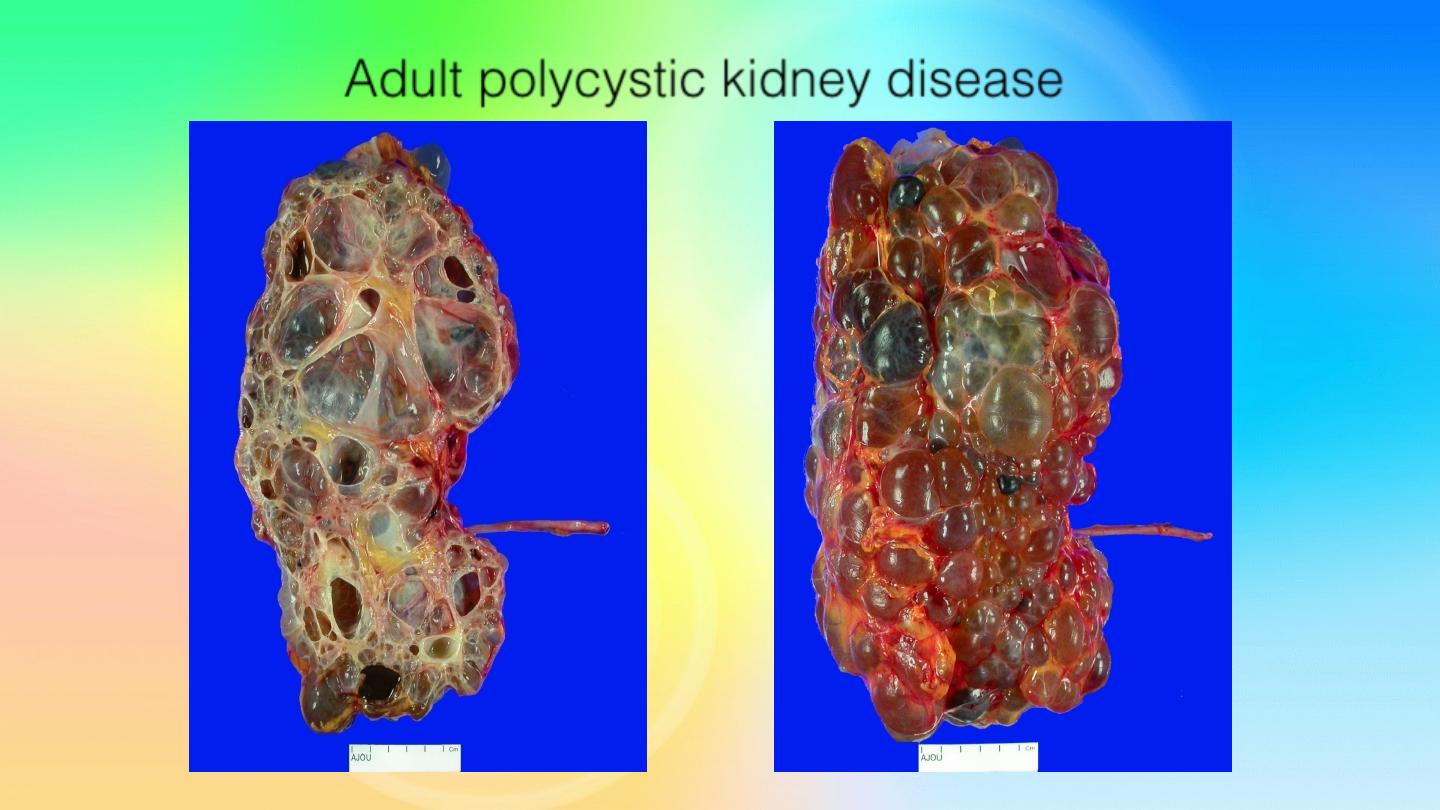
Adult polycystic kidney disease
Clinical presentation:
Rarely gives clinical manifestation before 4o years
Asymptomatic
Pain
Hematuria
Infection
Hypertension
Renal impairment
Renal enlargement
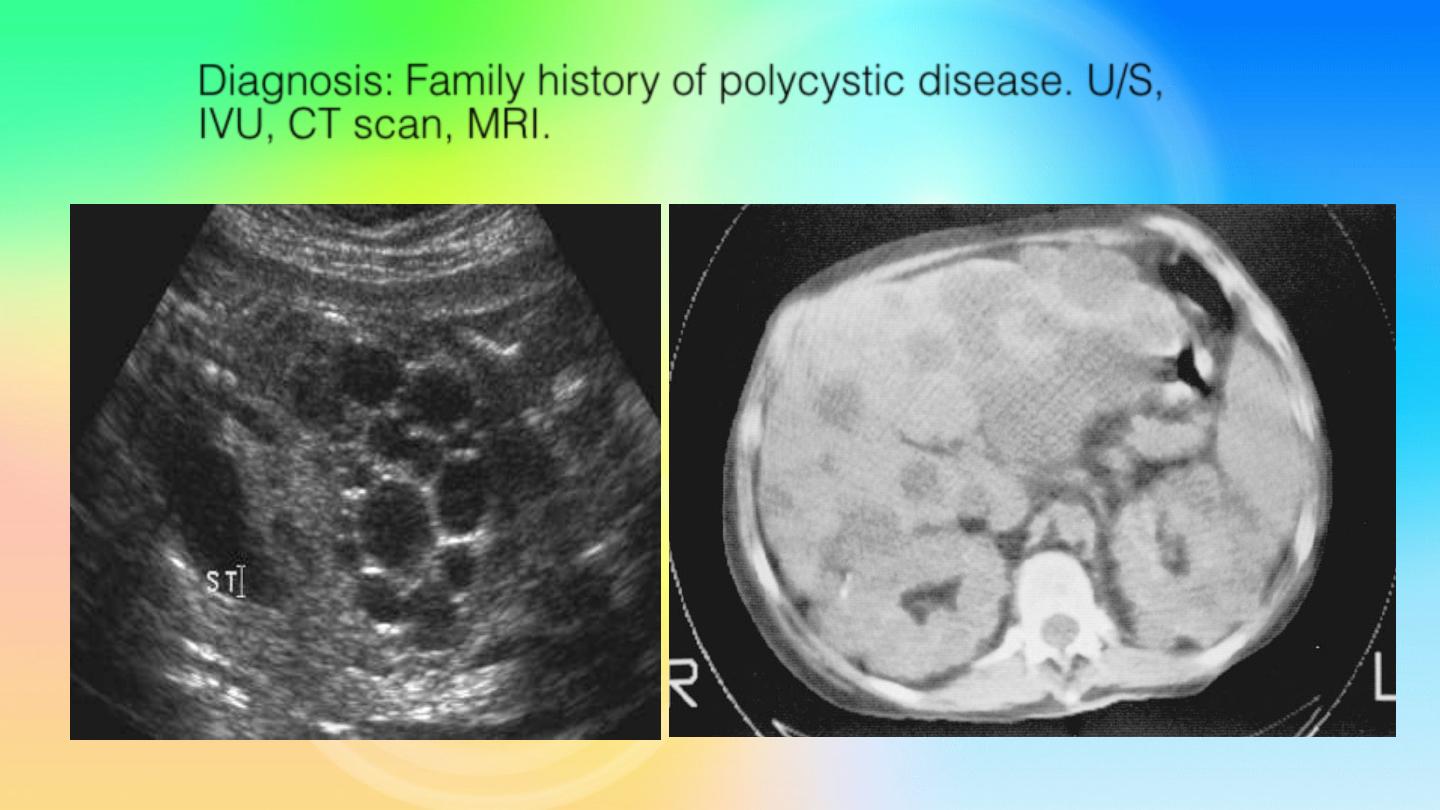
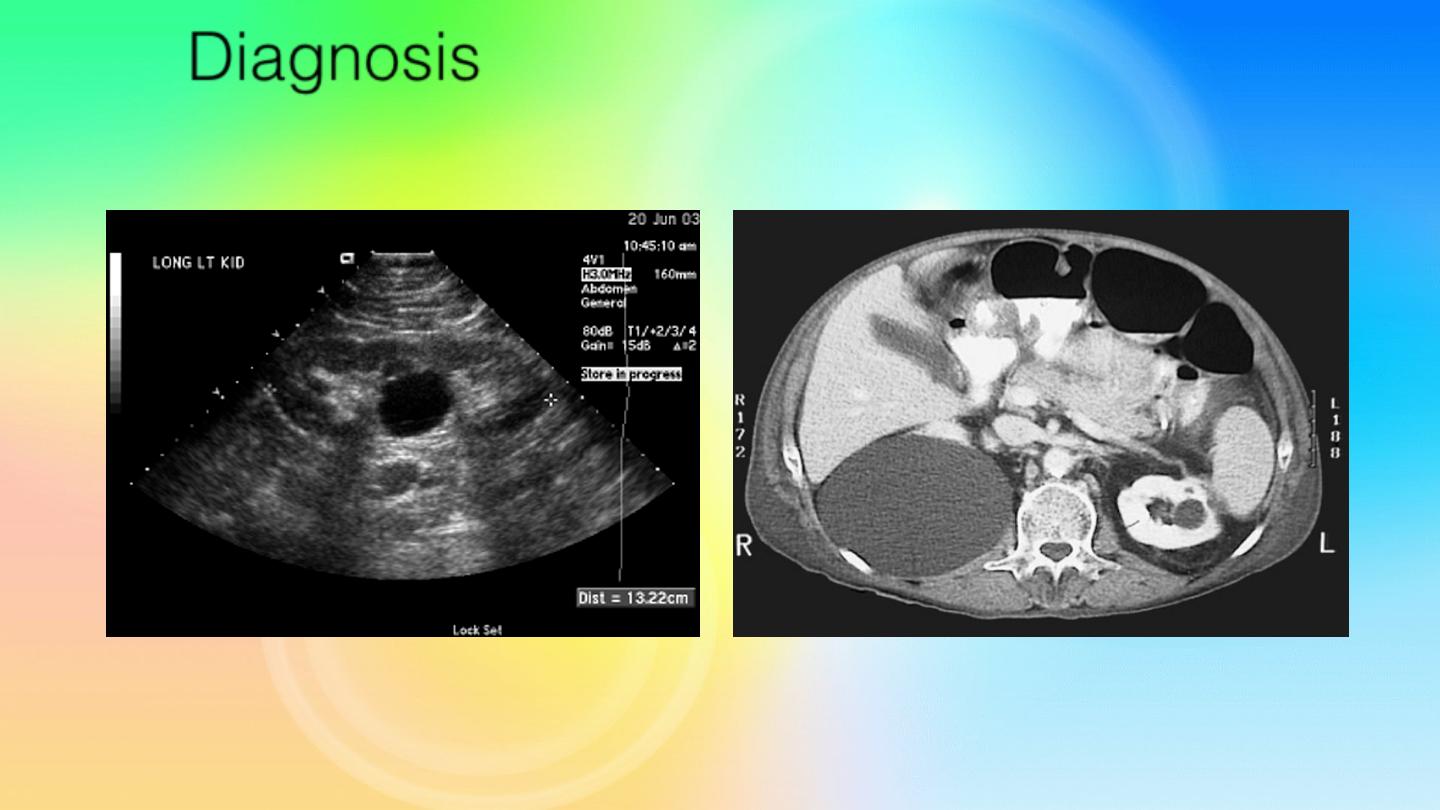
Diagnosis:
Family history of polycystic disease. U/S,
IVU, CT scan, MRI.

Treatment:
Medical:
To control infection, hypertension, pain and anemia.
Renal impairment: by
low protein diet and dialysis.
Surgical:
Rovsing’s operation (deroofing) for large cysts causing
symptoms or obstruction.
Stone removal.
Renal failure: Renal transplantation.
Autosomal recessive polycystic kidney disease
Rare autosomal recessive, incompatible with life.
50% die at
birth
.
Both kidneys are large in size and replaced by large number of
cysts which may obstruct labor. Associated with
hepatic fibrosis
Clinical features:
oligohydramnios, respiratory distress,
uremia, hypertension,
Treatment:
according to presentation. treat hypertension,
treat hepatic failure, transplant.

Simple (solitary) renal cyst
Common condition.
Single or multiple.
uni or bilateral.
Congenital or acquired.
Usually asymptomatic. In 10% symptomatic:
pain,
heaviness, infection, bleeding inside the cyst or
pressure effect
on the ureter causing
hydronephrosis.
Diagnosis
U/S, KUB, IVU, CT scan &MRI

Treatment:
usually no treatment needed
Symptomatic patients:
•
Aspiration and injection of sclerosing agent.
•
Rovsing’s operation (deroofing).
•
Partial or total nephrectomy in destructed kidney.
Congenital Anomalies of Renal pelvis & Ureter
Duplication of Renal Pelvis:
More common on left side.
Renorenal reflux
may occur from one pelvis to the other.
Duplication of the ureter:
Usually the ureters fuse & have
common orifice in the bladder although they may open
independently in the bladder.
Clinical features :
usually asymptomatic
More prone to infections, calculus disease & hydronephrosis
Treatment:
expectant
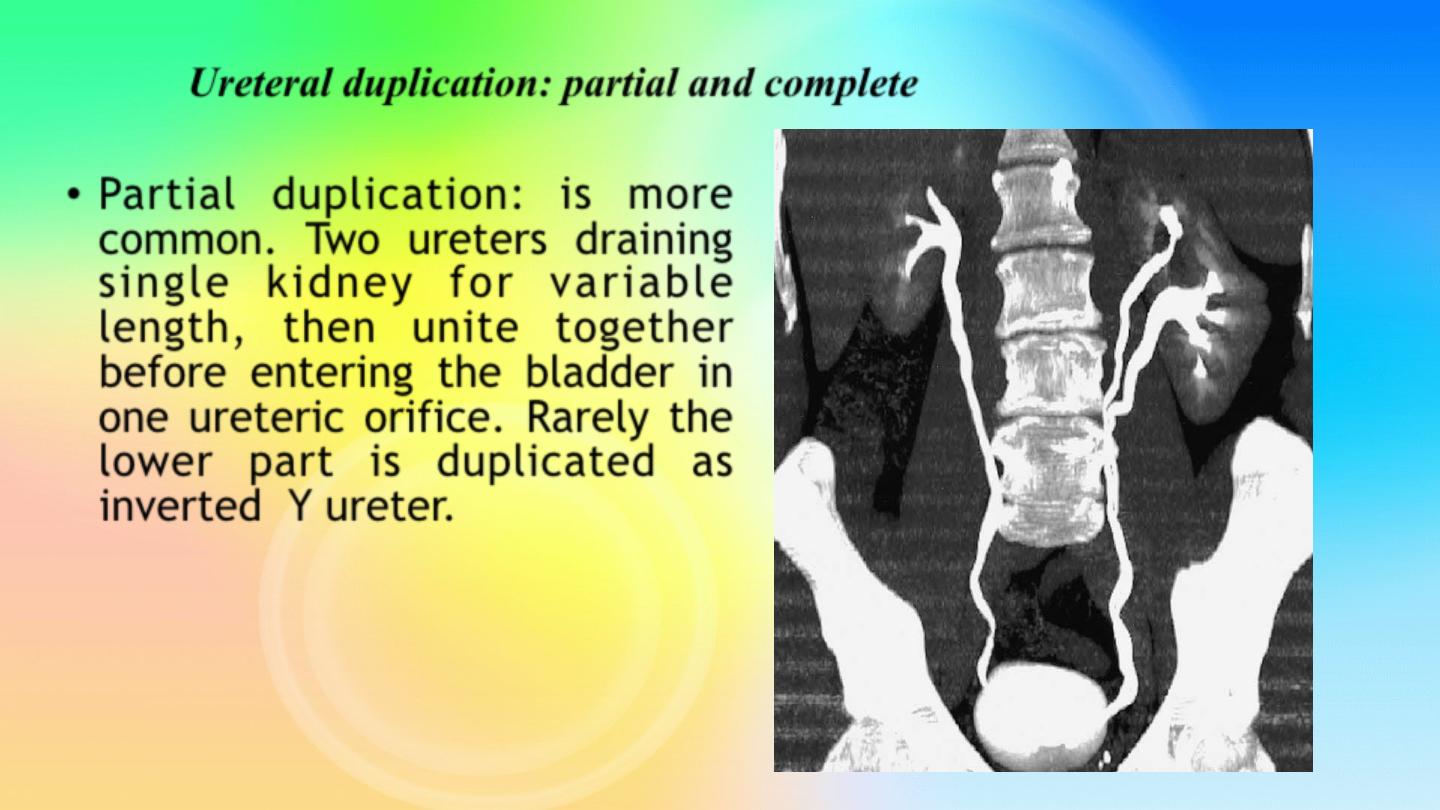
Ureteral duplication: partial and complete
•
Partial duplication:
is more
common. Two ureters draining
single kidney for variable
length, then unite together
before entering the bladder in
one ureteric orifice. Rarely the
lower part is duplicated as
inverted Y ureter.
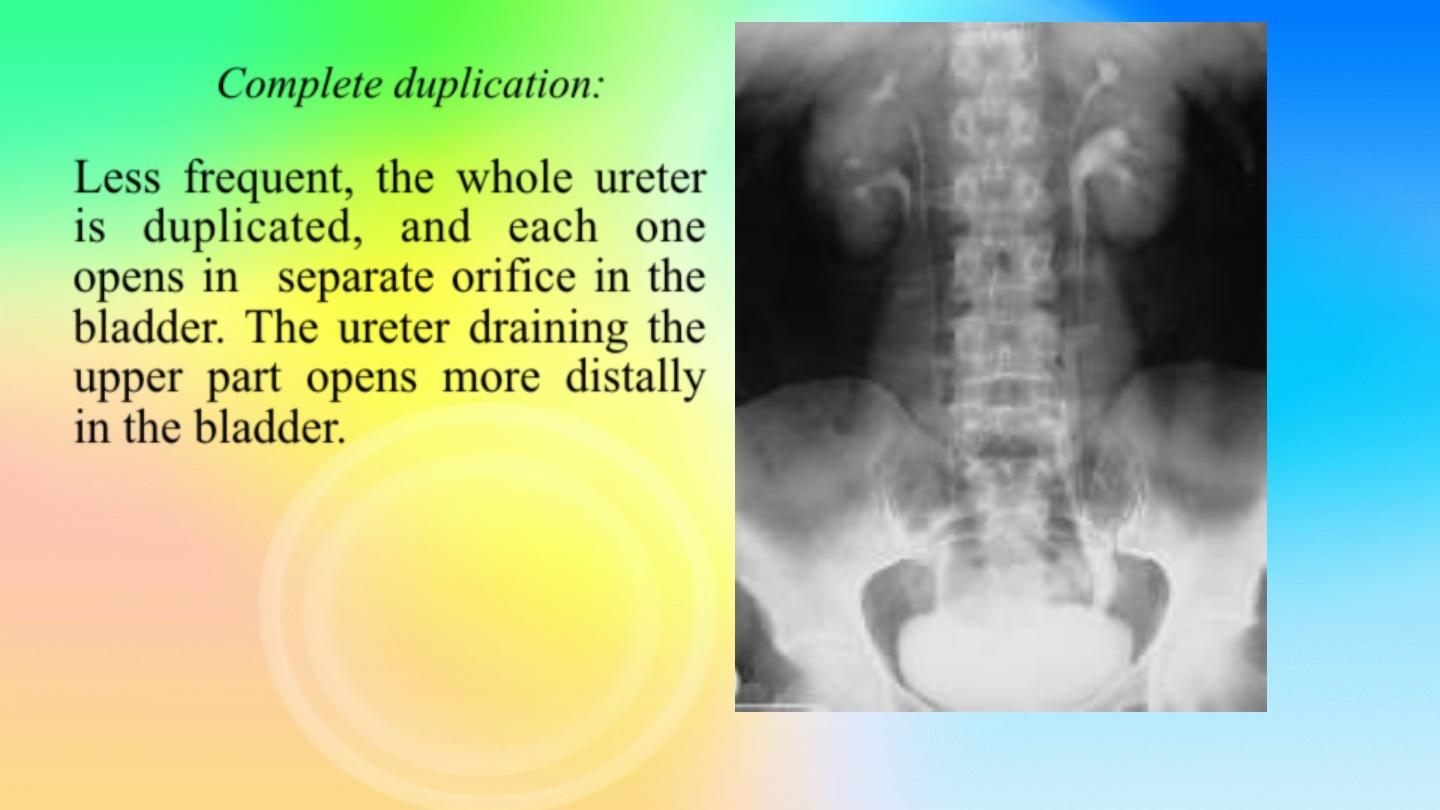
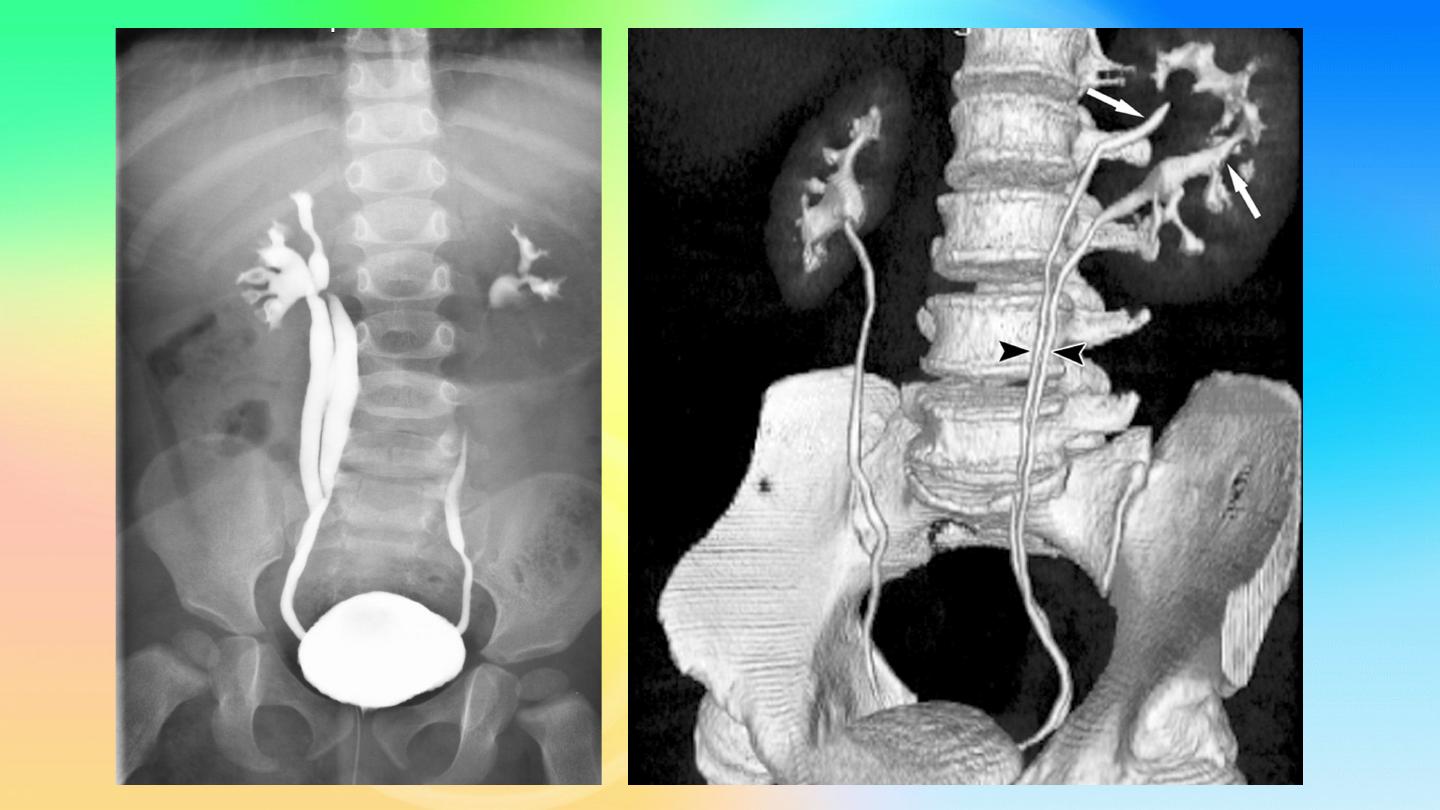
Complete duplication
:
Less frequent, the whole ureter
is duplicated, and each one
opens in separate orifice in the
bladder. The ureter draining the
upper part opens more distally
in the bladder.

Bifid renal pelvis
i
Ectopic Ureters
Ectopic ureter is the ureter that does not enter the trigonal area of the
bladder.
In the male, the posterior urethra is the most common site of termination,
also to semenal vesicle
In the female, the urethra and vestibule are the most common sites
Clinical features:
According to the site of orifice
In females: continuous dribbling
In males: urinary tract infection
Diagnosis:
IVU, U/S, CT scan, cystoscopy
Treatment:
Ureteric reimplantation
Ectopic ureters may drain renal moieties (either an upper pole or a single-
system kidney) that have minimal function. Therefore, upper pole
partial
nephrectomy
(or nephrectomy of single system) is sometimes
recommended
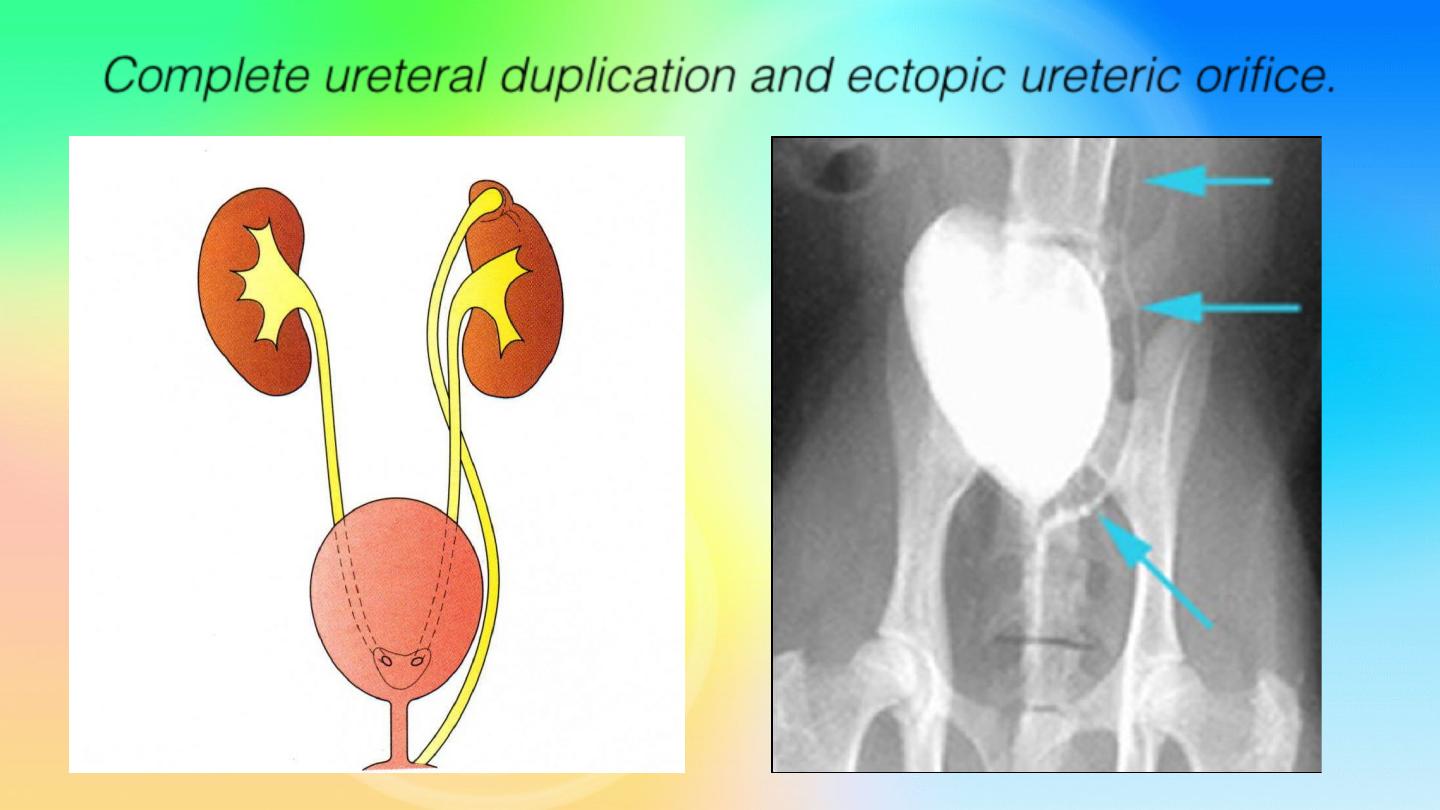
Complete ureteral duplication and ectopic ureteric orifice.
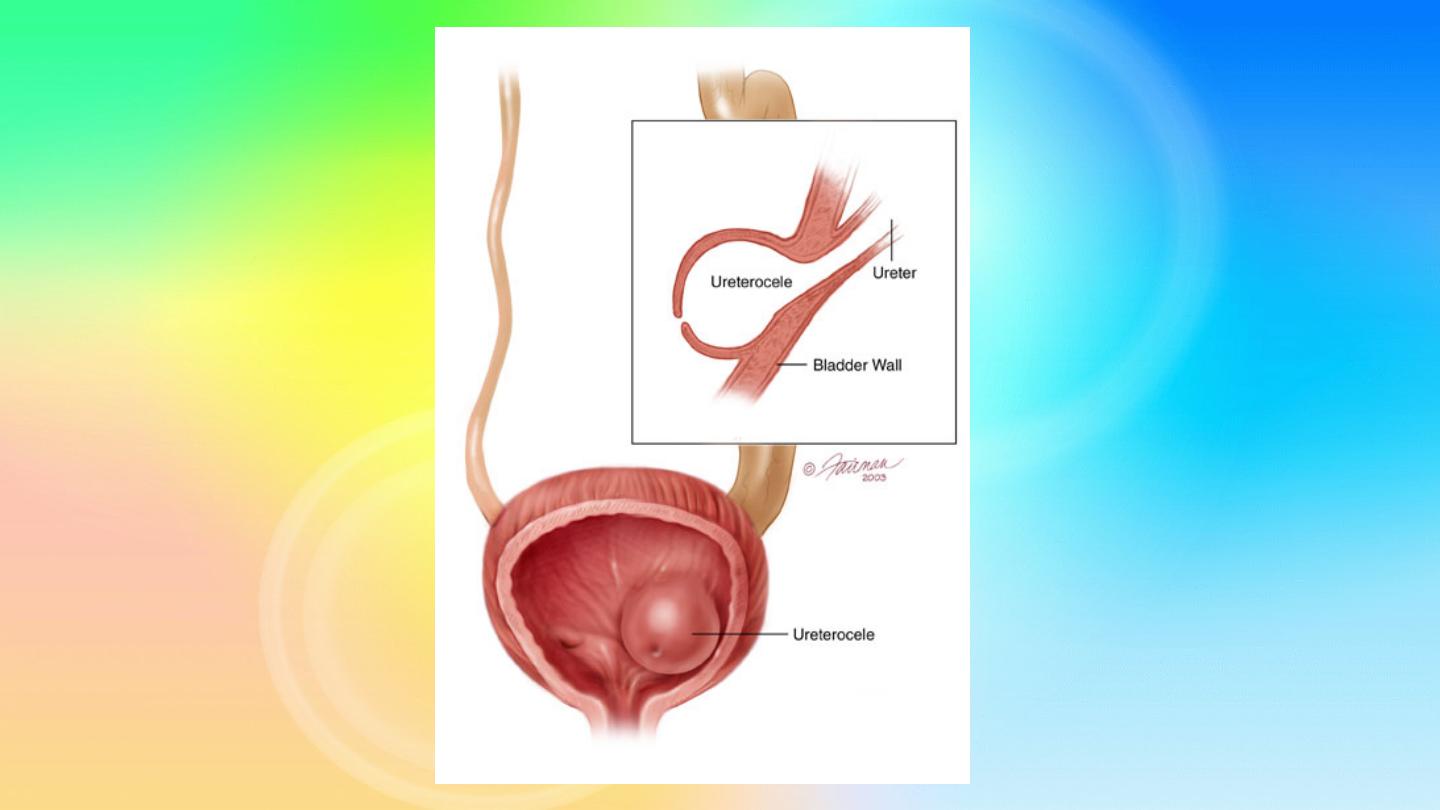
Ureteroceles
Is due to congenital atresia of the ureteric orifice which causes a
cystic dilatation of the intramural portion of the ureter
Women > men
Sometimes involves with ectopic ureter
More prone to stone disease & UTIs
Clinical Features
:
asymptomatic,
Repeated UTIs, Hematuria
Diagnosis
IVU, cystoscopy, cystogram
The ‘cobra head sign’ on excretory urography is typical.
Treatment
Asymptomatic : no treatment
Cystoscopy with diathermy incision of the ureterocele or Nephrectomy
in non functioning kidney
In complicated cases, ureteral reimplantation.
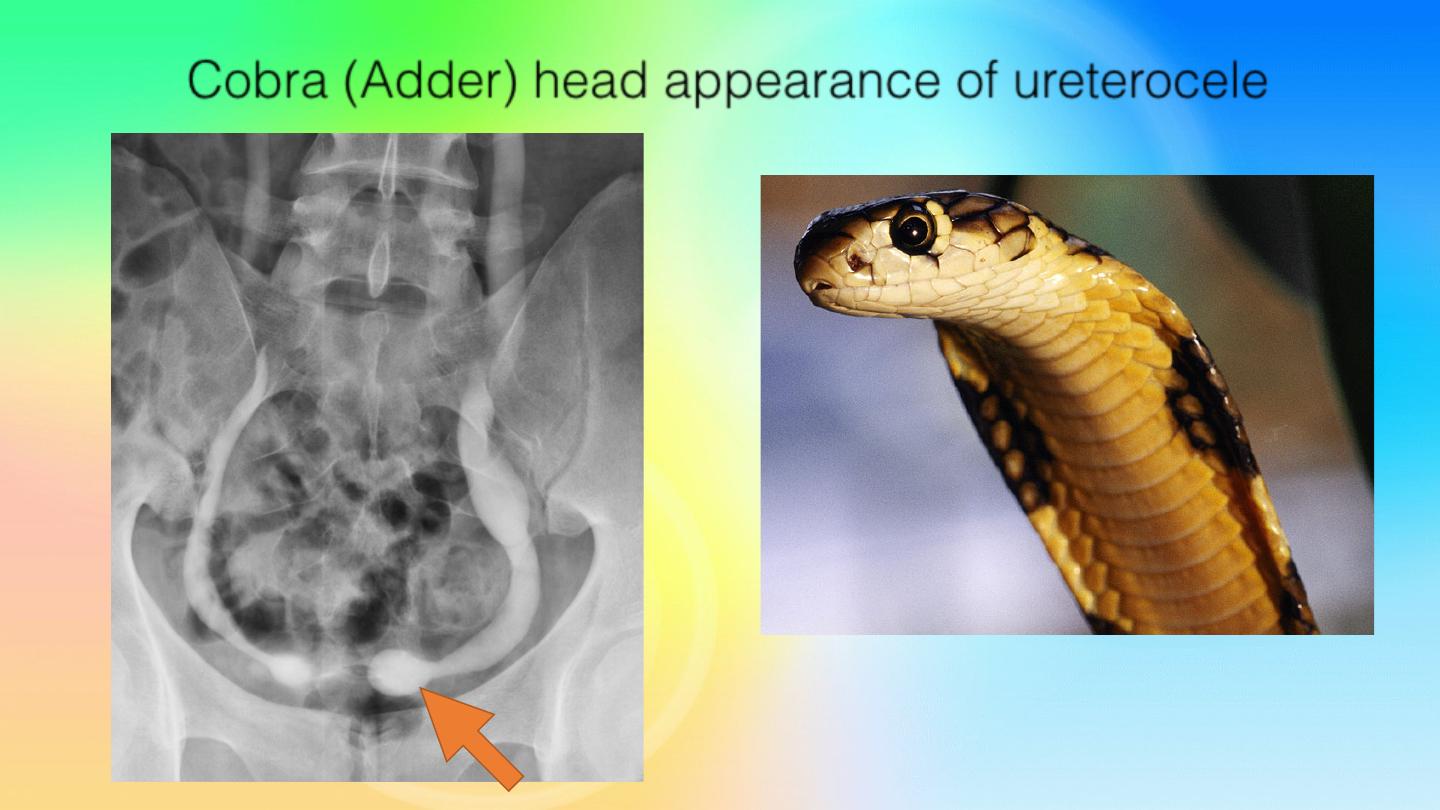
Cobra (Adder) head appearance of ureterocele
Ureteropelvic Junction (UPJ) (PUJ) Obstruction (stenosis)
The most common cause of significant dilation of the collecting
system in the fetal kidney
Boys > Girls
Left-sided lesions predominate
Could be bilateral
ETIOLOGY
Intrinsic (intramural):
interruption in the development of the
circular musculature of the UPJ or mucosal fold that causes valve
like effect.
Extrinsic:
An aberrant, accessory, or early-branching lower-pole
renal artery
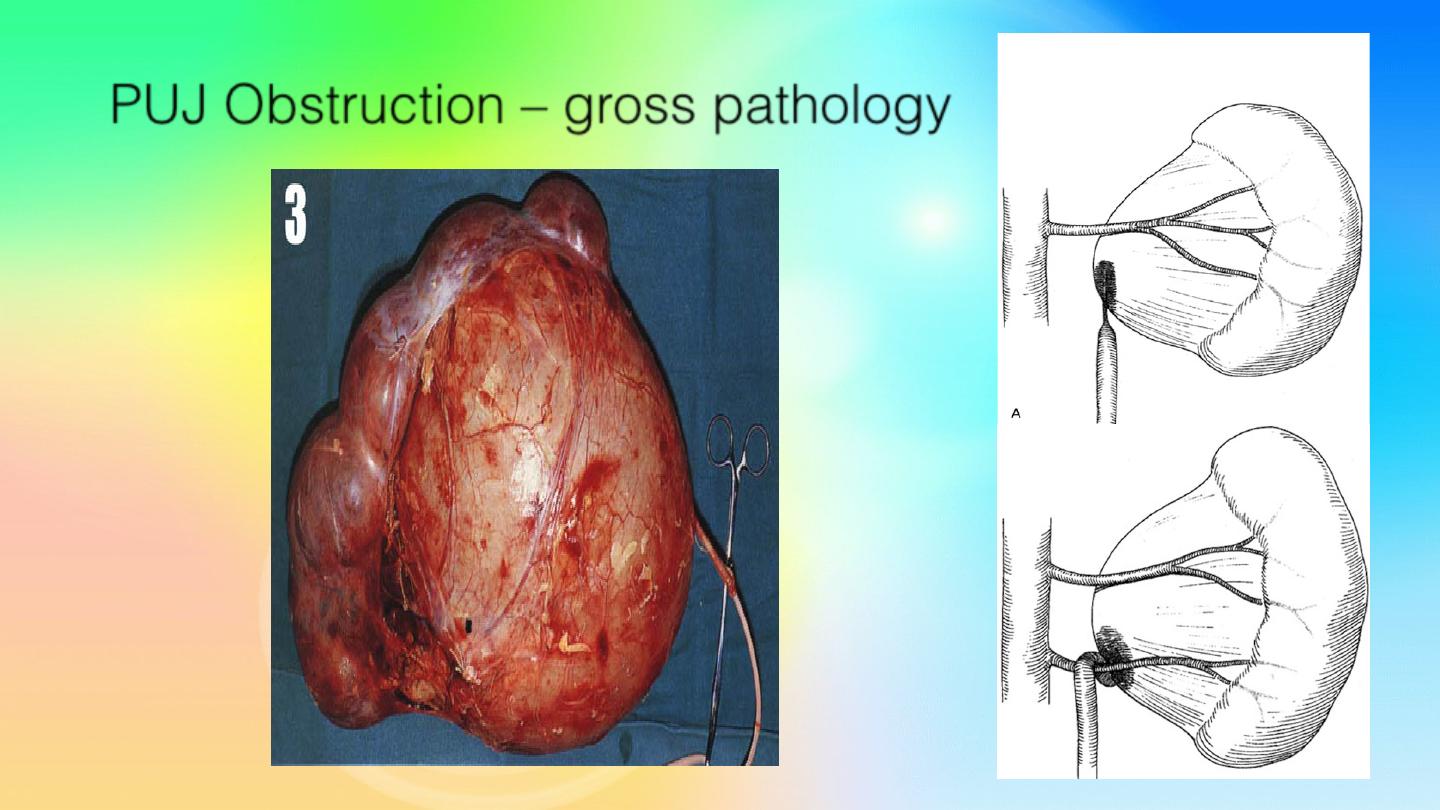
PUJ Obstruction – gross pathology
SYMPTOMS / PRESENTATION
Most infants are
asymptomatic
and most children are
discovered because of their symptoms
Episodic flank or upper abdominal
pain with recurrent
infections,
sometimes associated with
nausea and vomiting,
failure to thrive, diarrhea, and loin mass.
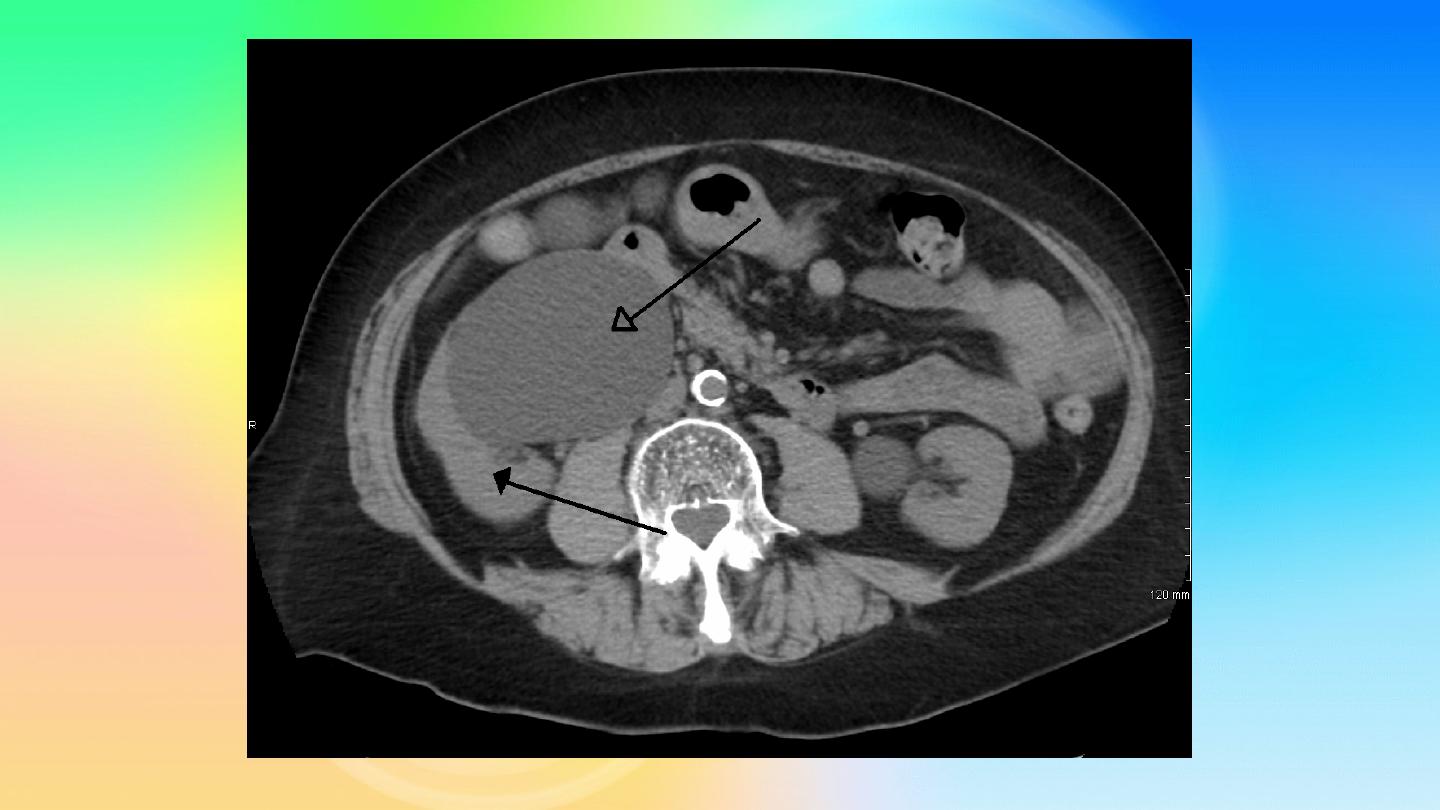
DIAGNOSIS
U/S, IVU, CT scan, Magnetic Resonance Imaging, Radionuclide
Renography: to see the split function of each kidney, Pressure-
Flow Studies and Whitaker test

Treatment:
Medical:
control infection and pain.
Suppressive antibiotics
Surgical:
Indications for surgery:
1-progressive hydronephrosis.
2- UTI despite antibiotic cover, and symptomatic
patients.
3- Severe hydronephrotic non functioning kidney.
4- deterioration of renal function

SURGICAL REPAIR:
including open surgical techniques, laparoscopic,
& endoscopic approaches
Open & laparoscopic surgical techniques
Anderson-Hynes dismembered pyeloplasty: excision
of the pathologic
UPJ & appropriate reanastamosis.
Flap technique or flap operation
Endoscopic Approaches:
•
Balloon dilatation
•
Antegrade endopyelotomy
•
Nephrectomy for non functioning kidney
Thank U 4 listening