Acute Renal Failure
Professor Dr. Issam Al-Azzawi
Head of Urology department

The maintenance of urine production
( Renal function )
is dependant on :
1 – satisfactory renal perfusion
2 – proper glomerular function
3 – proper tubular function

Acute Renal Failure could be
presented as :
• Anuria
• complete absence of
urine production
• Oliguria
• The excretion of less
than 300 ml / 24 h

Causes of renal failure
• Pre renal :
poor renal perfusion
• Hypovolemia, Blood loss, sepsis , shock, cardiogenic shock,
anaesthesia
• Renal :
Renal pathology ,
•
eg , glomerulonephritis , nephrotoxic drugs , poisons, Eclampsia,
contrast media, myoglobinuria , hemoglobinuria
• Post renal :
Obstructive
• Stones, pelvic malignancy, Bilharizia, retroperitoneal fibrosis,
Iatrogenic ureteral injuries, crystaluria, BPH, Urethral stricture

Clinical features of acute R. failure
• History
• Physical examination :
vital signs, checking the
urine output, signs of dehydration, signs of trauma /
bleeding, Anemia .
• Investigations :
RFT, HB, PCV, Urinalysis ( crystals,
casts etc… ), S. electrolytes, Ultrasound ( hydronephrosis ,
dilated ureters , stones , size of kidneys , cortical thickness )

Clinical progress of ARF
• 3 Phases
• 1 – Oliguria / Anuria
• 2 – Diuretic phase
• 3 – Recovery phase
• OR
• Death / progression to Chr. Renal failure

Managment of ARF
( according to the cause )
• * For Pre Renal & Renal causes :
•
1 – correction of hypovolemia
•
2 – good oxygenation
•
3 – inotropic agents ( Dopamin )
•
4 – diuretics ( mannitol )
•
5 – high calori intake
•
6 – Antibiotics
•
• Be aware of 2 dangerous complications :
•
acidosis & hyperkalemia
Management of ARF
•
Good response
Resumption of urine output
•
( between 8
th
& 10
th
day / up to 6 wk )
• ↓
• Diuretic phase ( heavy loss of Na & K )
• Poor response
vomiting, M. twitching, altered
consciousness, acidosis, hyperkalemia
• ↓
• Dialysis
( peritoneal / haemodialysis )

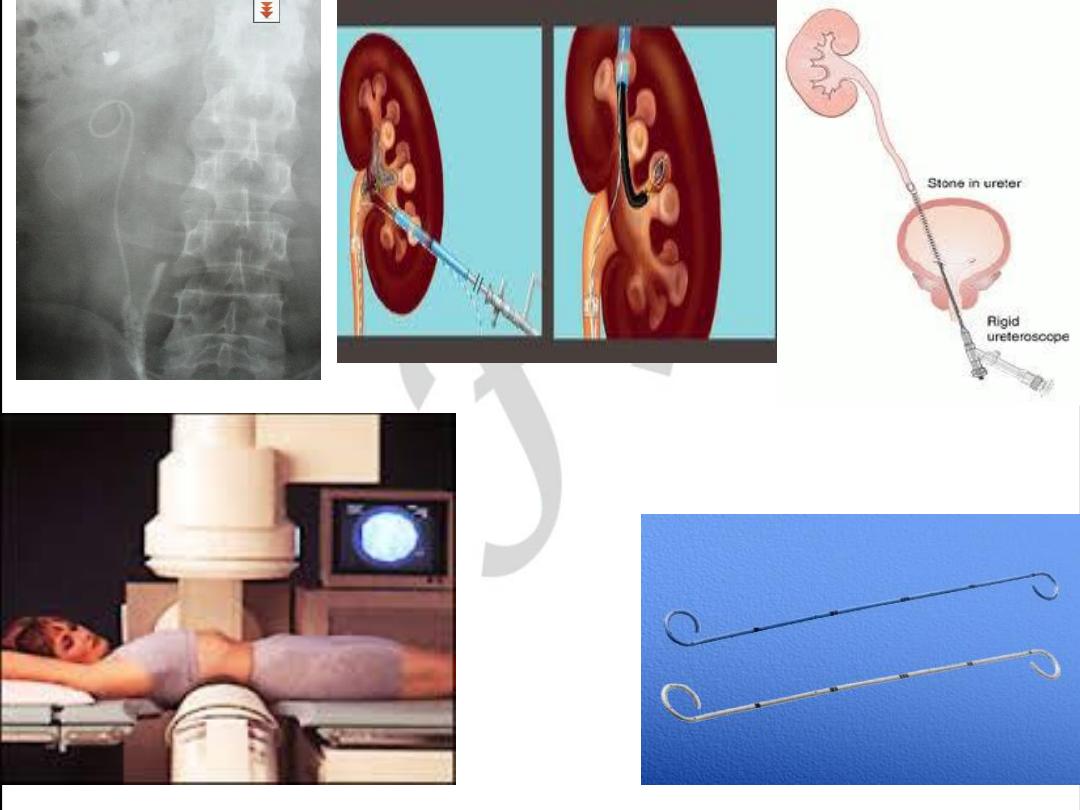
Post Renal ARF ( Obstructive )
• Emergency :
Drainage procedure :
PCN, JJ Stent
• Supportive :
fluid & electrolyte balance, diet, AB
• Treatment of individual causes :
•
stones
: MET, ESWL, Ureteroscopy
•
malignancy
: DXT, Hormonal, permanent nephrostomy
•
iatrogenic
: surgical correction
• bilharizial strictures & contractures
: surgical correction
•
retroperitoneal fibrosis
: JJ stent + steroids / ureterolysis
•
crystalluria
: increase fluid intake, Allopurinol , citrus fruits