Fifth stage
MedicineLec-3
د.محمد
6/11/2016
Megaloblastic AnaemiaDefinition : Megaloblastic anaemia are group of disorder characterized by the presence of distinctive morphological appearance of developing RBC in the BM leading to macrocytic anaemia and pancytopenia;
this abnormality affect all cells that have a rapid turnover : GIT mucosal cells,gonads and epidermal cells ,hence changes are evident; in the buccal mucosa, tongue, small intestine, cervix,vagina and uterus.,
Ineffective erythropoiesis; Bone marrow.
Megaloblastic anaemia is the result of abnormal DNA synthesis because of a single or combined deficiency of Folate, vitamin B12.Folate is an important substrate of, and vitamin B12 a co-factor for, the generation of the essential amino acid methionine from homocysteine.
Effect of Vit B12 on folate:
demethylation of folate that has been taken by the cells, allowing it to be conjugated (supplied with polyglutamates )vit. B12 deficiency prevents the cells from retaining folate, with following consequences :
elevated levels of 5-methyl tetra hydro folate (5-mTHF).
decrease level of intracellular polyglutamate folate caused by increased leakage of solute from the cells.
Deficiency of either vitamin B12 or folate will therefore produce high plasma levels of homocysteine and impaired DNA synthesis
Vitamin B12 :
A cobalt containing vitamin.
Found primarily in foods containing animal protein such as meat, fish eggs , milk.
The normal daily requirements is 1 μg daily
About 2-5 mg are stored in the liver, means that vitamin B12 deficiency takes years to develop.
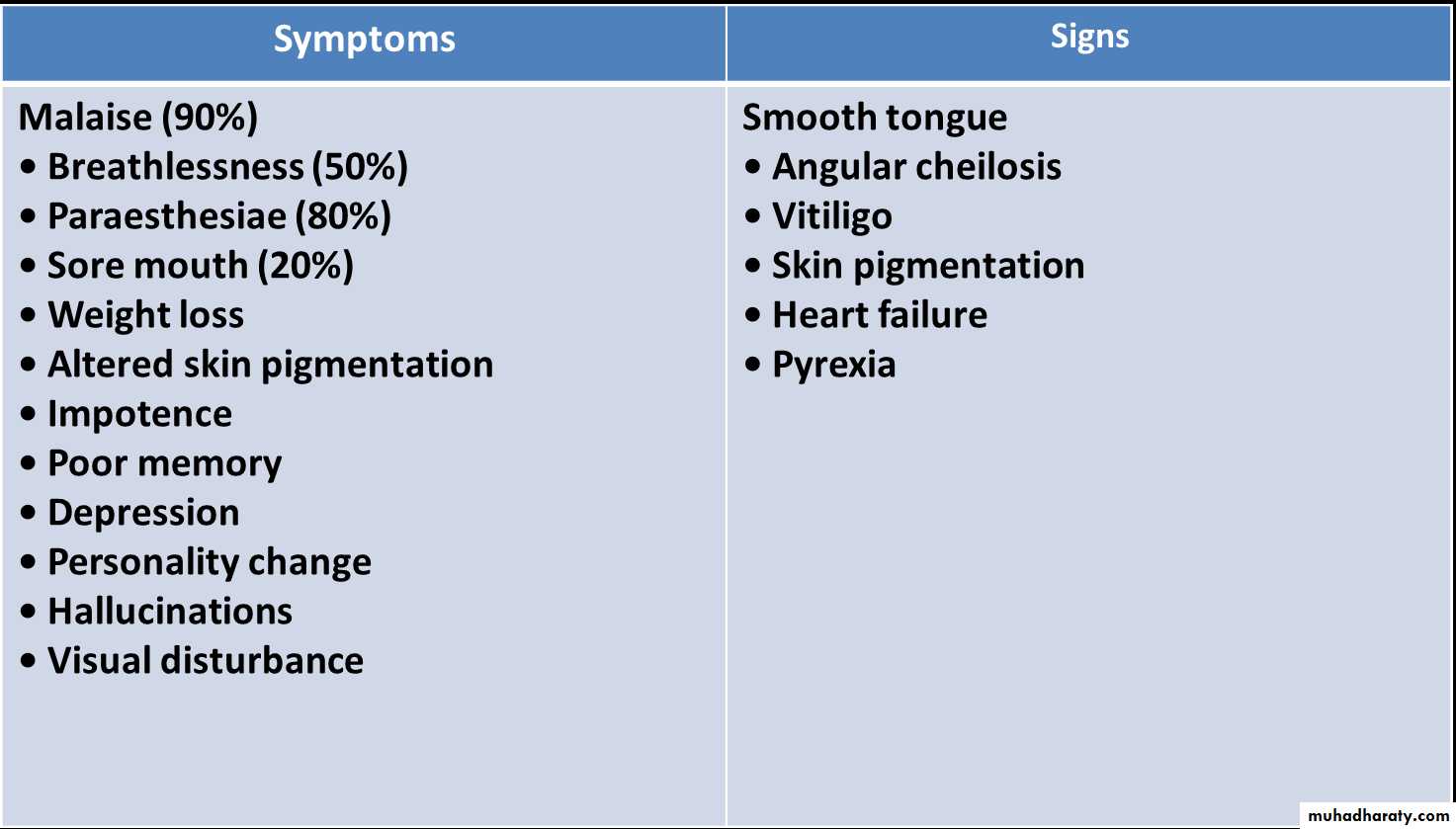
Clinical features of megaloblastic anaemia:
Neurological findings in B12 deficiency
Peripheral nerves• Glove and stocking paraesthesiae
• Loss of ankle reflexes
Spinal cord
• Subacute combined degeneration of the cord
Posterior columns – diminished vibration sensation and
proprioception
Corticospinal tracts – upper motor neuron signs
Cerebrum
• Dementia
• Optic atrophy
Autonomic neuropathy
Causes of vit. B12:
Depletion by decreased diet intake (vegans & vegetarians)
Poor absorption :absence of IF as in pernicions anaemia, gastrectomy and infiltration of stomach (lymphoma , Ca).
increased bacterial utilization of vit. B12.
gastrointestinal bypass surgery.
Small bowel diverticula.
Intestinal stasis & obstruction.
Parasitic infestation .
Fish tape worm (diphyllobotherium latum)
Pathology in absorption sites :
TB of the ileum.
Lymphoma of the small intestine.
Tropical sprue.
Regional enteritis.
Pernicious Anaemia (PA)
Etiology : PA a consequence of long standing gastritis lead to atrophy of all the cells of the stomach (secretory).Auto-immue mechanism :
Anti-intrinsic factor( IF) antibody( Ab.) found in 75% of pt. With PA. IgG or IgM found in saliva ,gastric juice, serum.
Other antibodies
Anti-parietal cell Abs.
Lymphocytic infiltration of gastric mucosa.
In the absence of intrinsic factor, less than 1% of dietary vitamin B12 is absorbed.
Pernicious anaemia has an incidence of 25/100 000 population over the age of 40 years in developed countries, but an average age of onset of 60 years.
It is more common in individuals with other autoimmune disease (Hashimoto’s thyroiditis, Graves’disease, vitiligo, hypoparathyroidism or Addison’s Disease)
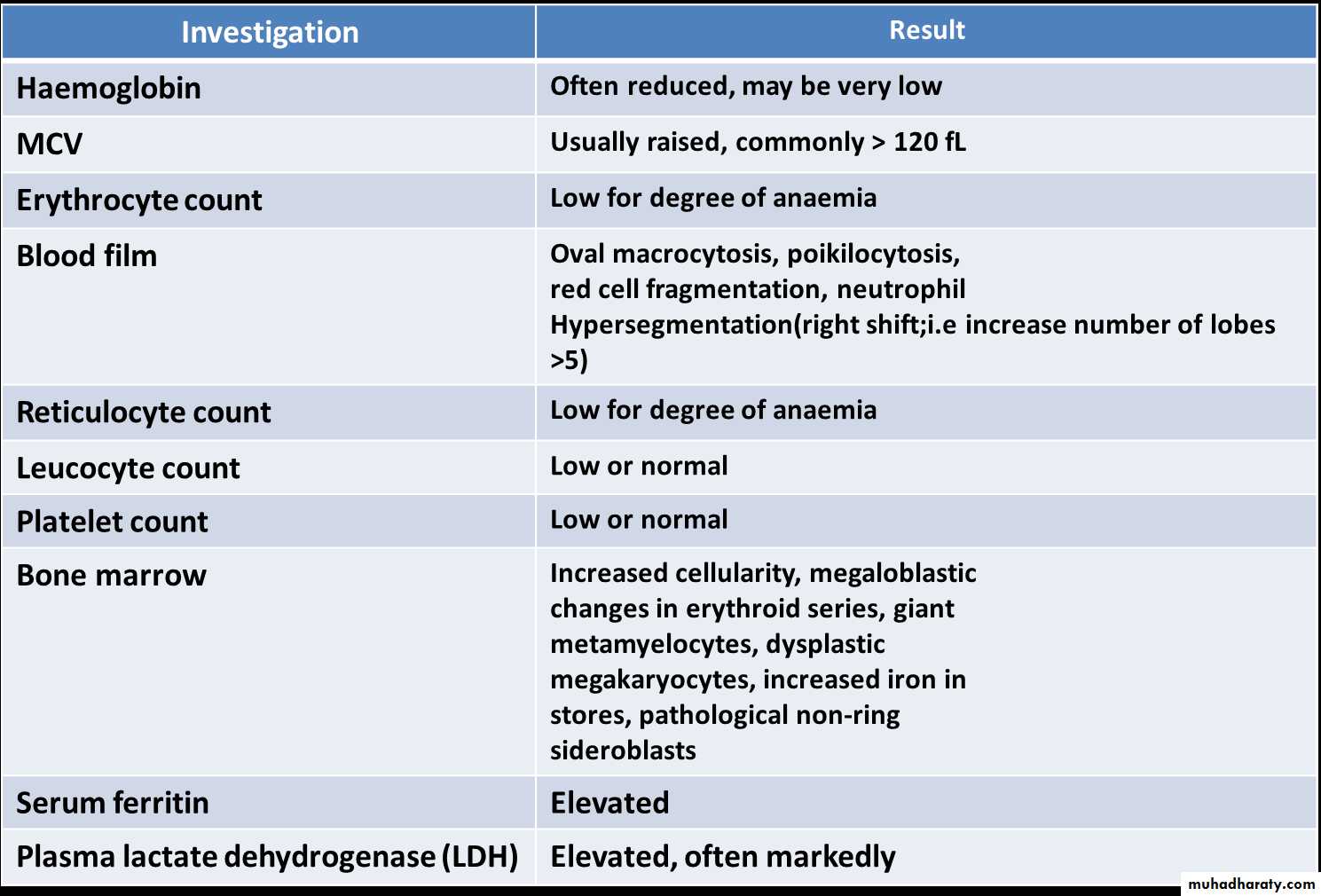
Investigations in megaloblastic anaemia:



Folate:
Folates are produced by plants and bacteria; hence dietary leafy vegetables (spinach, broccoli, lettuce), (kidney, fruits (bananas, melons) and animal protein ( liver (pteroyl-glutamate) folic acidtotal body folate is 10 mg in liver, daily requirement 100 µg.
Stores is sufficient for 4 month.
Causes of folate deficiency
Diet Poor intake of vegetables
Malabsorption Coeliac disease
Increased demand Cell proliferation (haemolysis), Pregnancy
Drugs Certain anticonvulsants (e.g. phenytoin), Contraceptive pill, Certain cytotoxic drugs (e.g. methotrexate).
Usually only a problem in patients deficient in folate from another cause.
Investigation of folic acid deficiency
Diagnostic findingsSerum folate levels may be low but are difficult to interpret
Low red cell folate levels indicate prolonged folate deficiency and are probably the most relevant measure
Corroborative findings
Macrocytic dysplastic blood picture
Megaloblastic marrow
Management of megaloblastic anaemia
Blood transfusions should be avoided , since circulatory overload may result. However if transfusion is needed to treat anoxia 1 or 2 units of packed cells can be administered slowly with concurrent administration of diuretics or phlebotomy on the other arm.The severely anaemic pt. who urgently needs therapy but whose vit deficiency is not clearly known should be given both folate & vit. B12. If this patient receive folate for what is actually a vit. B12 deficiency neurological abnormalities may precipitate and worsen.
Treatment of Vit B12 Deficiency
Vitamin B12 deficiency is treated with hydroxycobalamin 1000 μg IM for 6 doses 2 or 3 days apart, followed by maintenance therapy of 1000 μg every 3 months for life.Elderly pts with heart failure : should receive diuretics and oral potassium supplements for 10 days to prepare for Potential hypokalaemia.
The reticulocyte count will peak by the 5th–10th day after starting replacement therapy. The haemoglobin will rise by 10 g/L every week until normalised .
A sensory neuropathy may take 6–12 months to correct; long-standing neurological damage may not improve.
TREATMENT OF Folate deficiency
Oral folic acid 5 mg daily for 3 weeks for acute deficiency
5 mg once weekly is adequate for maintenance.
Prophylactic folic acid in pregnancy prevents megaloblastosis in women at risk, and reduces the risk of fetal neural tube defects
Supplementation Prophylactic is also given in chronic haematological disease associated with reduced red cell lifespan (e.g.haemolytic anaemias).