



Morphology of primary teeth
Importance of primary teeth1- Efficient mastication of food.
2- Maintenance of a normal face appearance (aesthetics).3- Formulation of clear speech (phonetics).
4- Prevent malocclusion.
5- Guide the eruption of permanent teeth and maintain of space and arch continuity for the emergence of permanent teeth.
Introduction
The morphology of primary teeth is very important clinically during performing various procedures.Cavity preparations must conform to the thickness of enamel & dentin keeping in mind the size & location of pulp horns .
Restoration of normal morphology of primary teeth is needed for function , this is can be achieved by good knowledge of morphology
• They have short crowns
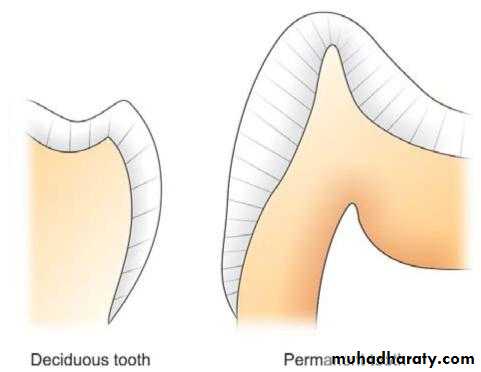
They are constricted at the cervical portionThey have thin enamel & dentin layers
Enamel rods in the cervical portion extend slightly occlusally from the CEJ
The occlusal surface is narrow labiolingually
The color of primary teeth is whiter than the permanent teeth
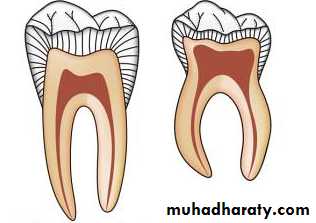
• The roots of primary anterior teeth are narrow mesiodistally
The roots of primary molars are longer & more slender in relation to their crownsThe roots of primary molars are more flare when approach to the apex (this provides a room for development of the buds of their successors)
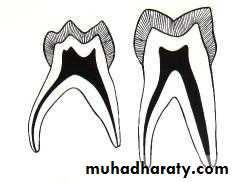

• Relatively larger
Pulp horns are closer to the outer surfaceGreat variation in size and location
Mesial pulp horn is higher
Form of the pulp follows the external anatomy , Usually a pulp horn under each cusp
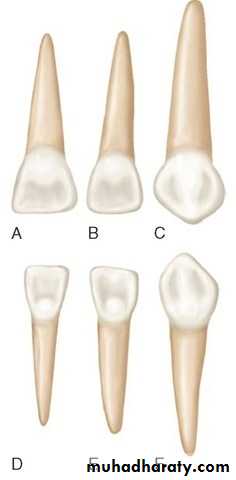
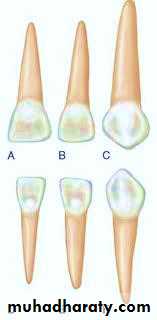
• Maxillary Central Incisor
Only tooth that has a greater mesiodistal width than heightProminent cingulum
Incisal edge straight
• Maxillary Lateral Incisor
Similar form to central but smallerdistoincisal angle is more rounded
• Mandibular Central Incisors-
Symmetrically flat when viewed from buccalCrown about 1/3 length of root
Cingulum present on lingual surface
Mandibular Lateral Incisor
Similar form to centralUsually longer
Incisal edge slopes toward distal and DI angle more rounded
• Maxillary Canine
Crown constricted at cervical region
Well developed, sharp cusp
Root is long, more than twice the length of the crown
Mandibular Canine
Similar form to maxillary
Crown shorter and narrower labiolingually.
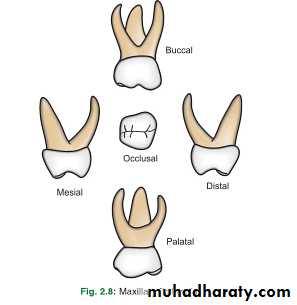
• Maxillary First Molar
Unique appearanceHas three cusps-MB, DB and Lingual
Prominent MB cervical bulge
Has three roots
• Mandibular First Molar
Also unique in appearanceFour cusps-MB, DB, ML and DL
Prominent MB cervical bulge
Has a transverse ridge
Has two roots

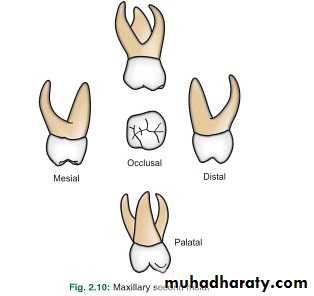
• Maxillary 2nd molar
It is larger than maxillary 1st molarResembles permanent maxillary first molar but smaller
Has a minor 5th cusp, cusp of carabelli
• Mandibular 2nd molar
Has an overall oval occlusal shapehas five cusps
Resembles permanent lower first molar but smaller


• Darker , more pigmented & have less translucent enamel
Whiter , less pigmented & have more translucent enamel
color
• Cusps are blunt & the crowns are not bulbous
Cusps are more pointed & the crowns are bulbous
shape• The enamel ends gradually at the neck
The enamel ends abruptly at the neck
Cervical area
Longer, stronger, less divergent away from the crown
Shorter, weaker, more divergent close to the crown
roots
• Placed obliquely on the jaws
Placed perpendicularly on the jawsPlacement in jaws
Mamelons may present
No mamelons
Incisal edges
thicker
thinner
dentin
• more calcified, less permeable, rods near the cervical portion directed apically
Less calcified, more permeable, rods near the cervical portion perpendicular to the DEJ
enamel
Clinical significance of teeth morphology
Thickness of E & D in primary teeth is less than in permanent teeth this means that the pulp chamber is very close to the external surface of the tooth. This should be kept in mind during cavity preparation .Aggressive removal of careis will lead to exposure .

Clinical significance of teeth morphology
Understanding tooth morphology is of great importance to restore the normal form of the tooth which is required for function .
Clinical significance of teeth morphology
Prominent buccal cervical ridge of mand. First molar provide resistance to the placement of crowns . So it requires more reduction .
Clinical significance of teeth morphology
flare roots of primary molars dictate the tooth therefore it require more caution during extraction .
Clinical significance of teeth morphology
Knowledge of teeth morphology can enable the dentist to identify the teeth when there are multiple extracted teeth , or in period of mixed dentition .
• The factors that have been related to the eruption of teeth include:
• 1. elongation of the root,• 2. forces exerted by the vascular tissues around and beneath the root,
• 3. growth of the alveolar bone,
• 4. growth of dentin,
• 5. growth and pull of the periodontal membrane,
• 6. hormonal influences,
• 7. presence of a viable dental follicle,
• 8. pressure from the muscular action, and
• 9. resorption of the alveolar crest
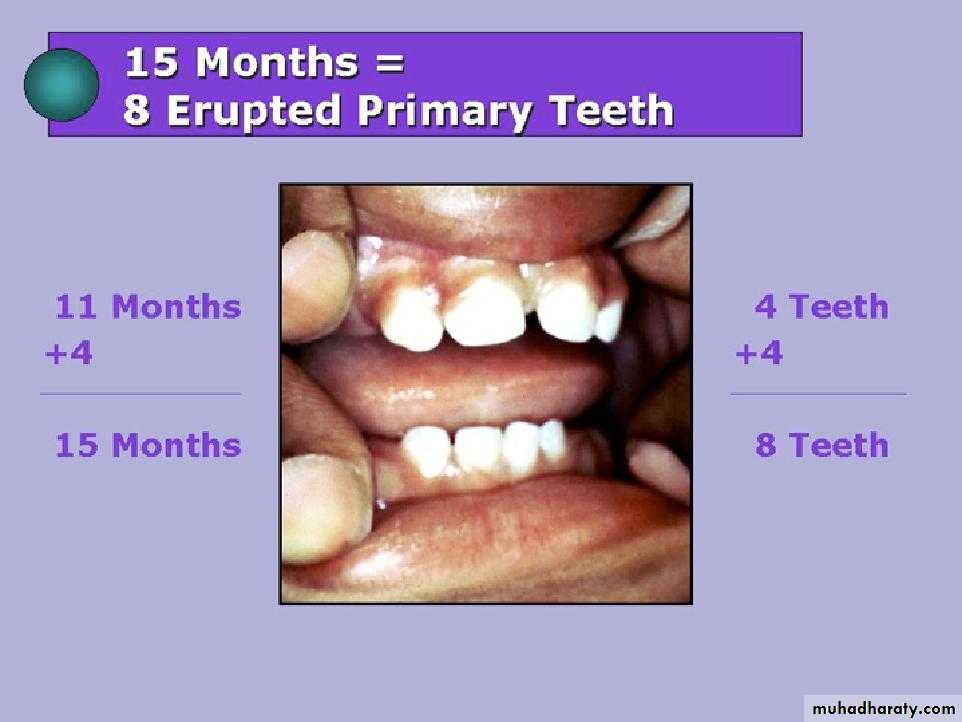
Sequence of eruption
Primary teeth upper arch ABDCE
lower arch ABDCE
Permanat teeth upper arch 61245378
lower arch 61234578TEETHING AND DIFFICULT ERUPTION
In most children the eruption of primary teeth is preceded by increased salivation, and the child will want to put the hand and fingers into the mouth.These observations may be the only indication that the teeth will soon erupt.
Some young children become restless and anxious during the time of eruption of the primary teeth
Conditions, including, diarrhea, fever, convulsions, have been incorrectly attributed to eruption
Inflammation of the gingival tissues before complete emergence of the crown may cause a temporary painful condition that subsides within a few days
If the child is having extreme difficulty, the application of a nonirritating topical anesthetic may bring temporary relief
ERUPTION HEMATOMA (ERUPTION CYST)
A bluish purple, elevated area of tissue, commonly called an eruption hematoma, occasionally develops a few weeks before the eruption of a primary or permanent tooth.The blood-filled cyst is most frequently seen in the primary second
molar or the first permanent molar regions
Usually within a few days the tooth breaks through the tissue, and the hematoma subsides.
Because the condition is almost always self-limited, treatment of an eruption hematoma is rarely necessary.
ECTOPIC ERUPTION
Arch length inadequacy, tooth mass redundancy, or a variety of local factors may influence a tooth to erupt or try to erupt in an abnormal position.Occasionally this condition may be so severe that actual transposition of teeth takes place.
N A T A L A N D N E O N A T A L TEETH
The prevalence of natal teeth (teeth present at birth) and neonatal teeth (teeth that erupt during the first 30 days) is low.They found that about 85% of natal or neonatal teeth are mandibular primary incisors, and only small percentages are supernumerary teeth.
Most prematurely erupted teeth (immature type) are hypermobile because of the limited root development.
Some teeth may be mobile to the extent that there is danger of displacement of the tooth and possible aspiration, in which case the removal of the tooth is indicated.
In some cases, the sharp incisal edge of the tooth may cause laceration of the lingual surface of the tongue ( Riga-Fede disease), and the tooth may have to be removed.
Extraction of such a tooth, if necessary, is a simple procedure but is emotionally difficult for the parents.
The preferable approach, however, is to leave the tooth in place and to explain to the parents the desirability of maintaining this tooth in the mouth because of its importance in the growth
A retained natal or neonatal tooth may cause difficulty for a mother who wishes to breast-feed her infant.
If breast-feeding is too painful for the mother initially, the use of a breast pump and bottling of the milk are recommended.
LOCAL AND SYSTEMIC FACTORS THAT INFLUENCE ERUPTION
ANKYLOSED TEETH
Application of the term submerged molar to this condition is inaccurate
This misconception results from the fact that the ankylosed tooth is in a state of static retention, whereas in the adjacent areas eruption and alveolar growth continue.
The term infraocclusion, although commonly used today
ankylosis should be considered an interruption in the rhythm of eruption and further observed that a patient who has one or two ankylosed teeth is more likely to have other teeth become ankylosed.
The mandibular primary molars are the teeth most often observed to be ankylosed
Primary molars may become firmly attached to the alveolar bone before their normal exfoliation time
Ankylosis of the anterior primary teeth does not occur unless there has been a trauma
The cause of ankylosis in the primary molar areas is unknown, but at least three theories have been proposed.
The occurrence is noted to have a familial tendency
There is a relationship between congenital absence of permanent teeth and ankylosed primary teeth.
Normal resorption of the primary molar begins on the inner surface or the lingual surface of the roots.
The resorption process is not continuous but is interrupted by periods of inactivity or rest.
A reparative process follows periods of resorption.
In the course of this reparative phase a solid union often develops between the bone and the primary tooth.
This intermittent resorption and repair may explain the varying degrees of firmness of the primary teeth before their exfoliation.
Extensive bony ankylosis of the primary tooth may prevent normal exfoliation, as well as the eruption of the permanent successor
Ankylosis of the primary molar to the alveolar bone does not usually occur until after its root resorption begins.
If ankylosis occurs early, eruption of adjacent teeth may progress enough that the ankylosed tooth is far below the normal plane of occlusion and may even be partially covered with soft tissue
The diagnosis of an ankylosed tooth is not difficult to make.
1-Because eruption has not occurred and the alveolar process has not developed in normal occlusion, the opposing molars in the area seem to be out of occlusion.2-The ankylosed tooth is not mobile, even in cases of advanced root resorption.
3-The ankylosed tooth will have a solid sound, whereas the normal tooth will have a cushioned sound because it has an intact periodontal membrane that absorbs some of the shock of the blow.
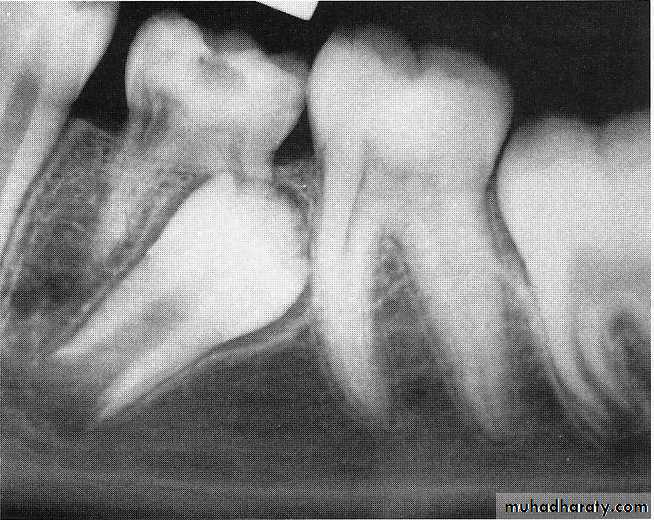
The radiograph is often a valuable aid in making a diagnosis.
A break in the continuity of the periodontal membrane indicating an area of ankylosis is often evident radiographically.In the management of an ankylosed tooth, early recognition and diagnosis are extremely important.
The eventual treatment may involve surgical removal
A tooth that is definitely ankylosed may at some future time undergo root resorption and be normally exfoliated.
When patient cooperation is good and recall periods are regular, a watchful waiting approach is best.
ANKYLOSIS OF PRIMARY MOLARS WITH ABSENCE OF PERMANENT SUCCESSORS
Kurol and Thilander emphasize the importance of the presence of a permanent successor for normal exfoliation of a primary molar.
In their longitudinal study no ankylosed primary molars without permanent successors were found to exfoliate spontaneously.
In situations in which permanent successors of ankylosed primary molars are missing, attempts have been made to establish functional occlusion using stainless steel crowns, overlays, or bonded composite resins on the affected primary molars.
This treatment is successful only if maximum eruption of permanent teeth in the arch has occurred. If adjacent teeth are still in a state of active eruption, they will soon bypass the ankylosed tooth
ANKYLOSED PERMANENT TEETH
The incomplete eruption of a permanent molar may be related to a small area of root ankylosis.The removal of soft tissue and bone covering the occlusal aspect of the crown should be attempted first, and the area should be packed with surgical cement to provide a pathway for the developing permanent tooth
If the permanent tooth is exposed in the oral cavity and at a lower occlusal plane than the adjacent teeth, ankylosis is the probable cause.
Unerupted permanent teeth may become ankylosed.
The close association of an infected apex to an unerupted tooth may give rise to the process. In the unerupted tooth, enamel is protected by enamel epithelium.The enamel epithelium may disintegrate as a result of infection (or trauma), the enamel may subsequently be resorbed, and bone or coronal cementum may be deposited in its place.
Trisomy 21 syndrome (Down syndrome [DS]) is one of the congenital anomalies in which delayed eruption of the teeth frequently occurs.
The first primary teeth may not appear until 2 years of age, and the dentition may not be complete until 5 years of age. The eruption often follows an abnormal sequence, and some of the primary teeth may be retained until 15 years of age.
These studies seem to confirm that delayed tooth eruption is common but sporadic in children with DS.
• TRISOMY 21 SYNDROME (DOWN SYNDROME)