Cardio-Lect-2 Prof.Dr.Hussain Al-Janabi.
VI.Conclusion of ECG interpretation(Dx) :A.normal ECG(No abnormal changes seen in the trace)&reported as follows:(Regular sinus rhythm, Heart rate-----bpm,PR interval -----Sec. QT normal,axis----&tracing is normal.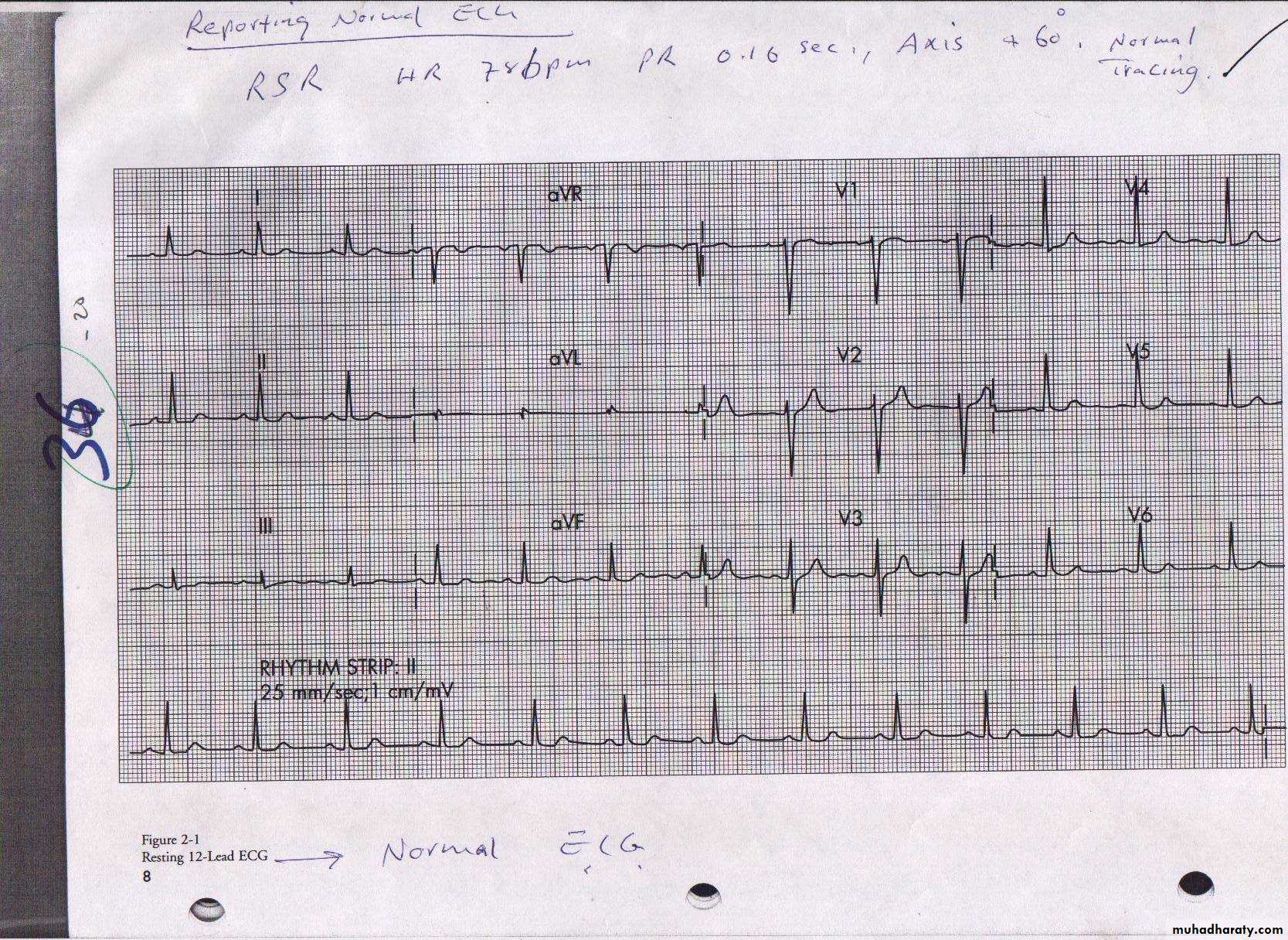
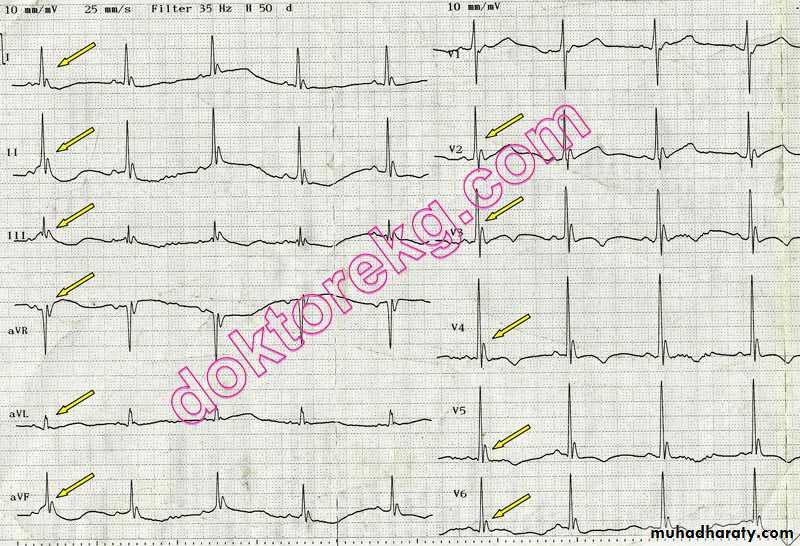
B.Abnormal ECG;screen all leads for abnormal changes&try to make an an a abnormal pattern out of them i.e ECG Dx. ECG p Patterns:The ECG Dx. I.Hypertrophy patterns(chamber enlargement). I. *RA RAE(RAH):Tall peaked p-wave>2.5mm. best seen in inferior leads(II II&aFV). Causes: 1.pulmonary hypertension(PH)due to any cause like primary pulmonary h PH, hypertension ,Corpulmonale, left – right shunt. 2.TV disease 3.PV disease. 4.Ebistien anomaly.

*LAE 1.Widened p-wave(>0.12Sec.)& maybe notched.Best seen in leads(I&II).
2.Wide &deep terminal part of P(−Ve component) in V1( duration >0.04s&>1mm depth) . Causes: 1.Chronic LV dysfunction as in IHD,CMP&LVHdue to any cause.2.Mitral valve disease.
ECG Criteria of LAE.
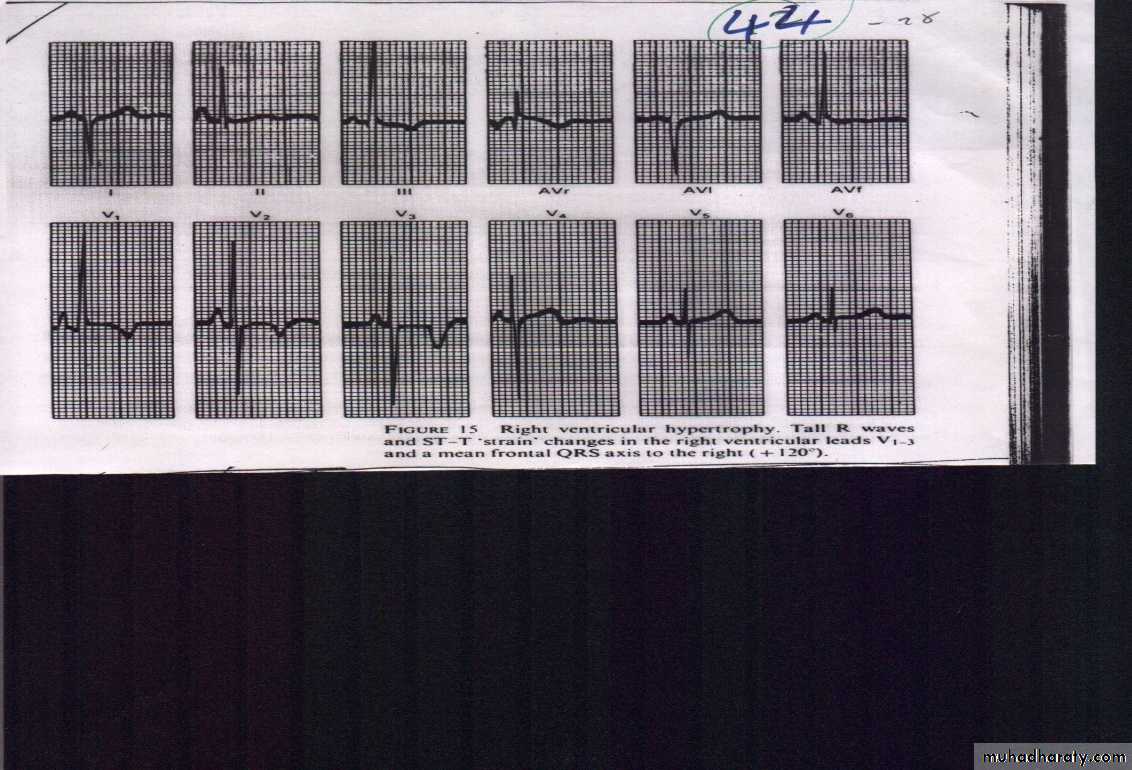
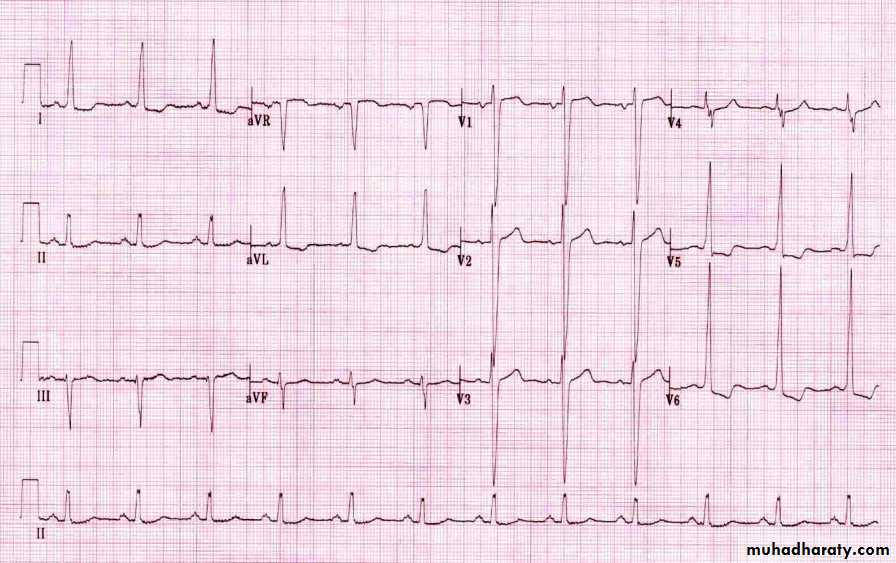
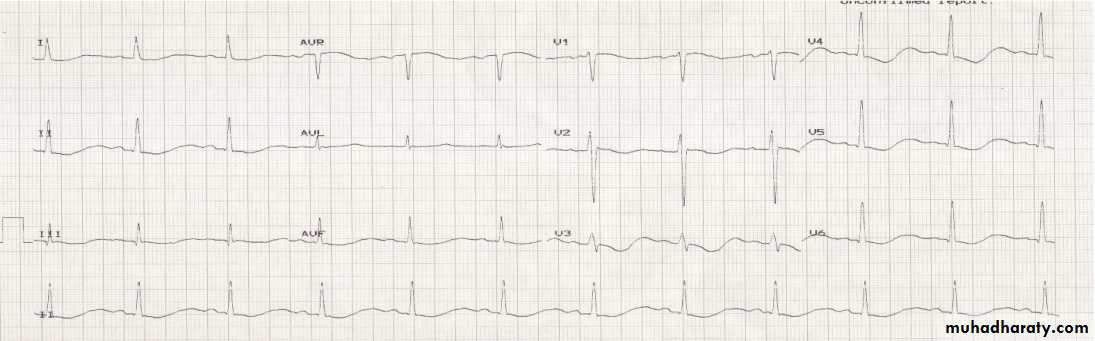
*RVH: The ECG criteria: 1.Tall R-wave >S in rightward-leads(V1-V4) 2.R in V1/V2+S in V5/V6 >10.1 mm(1.10mV).3.RAD. 4.RV strain(ST↓ +T↓ in rightward leads(V1-V4). Causes of RVH:A.RV-Pressure overload as in PH(due to various causes)&PS B.RV-volume overload as in L-R shunt (ASD,VSD&PDA)&TR.
RVH(Note*RAD (+150)*Dominant R wave in V1 (> 7 mm tall; R/S ratio > 1)*Dominant S wave in V6 (> 7 mm deep; R/S ratio > 1).*Right ventricular strain pattern with ST depression and T-wave inversion in V1-V4.
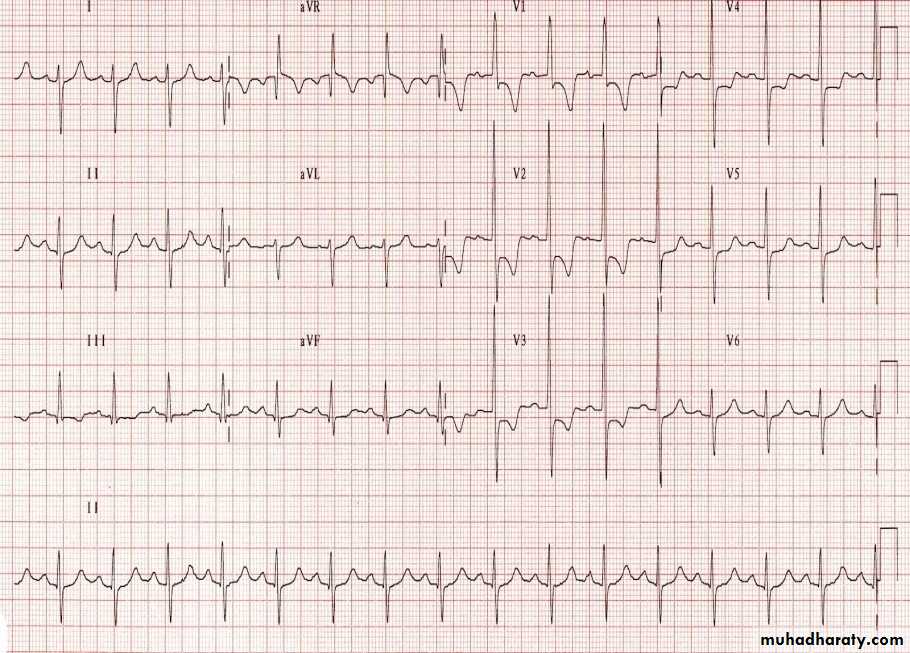
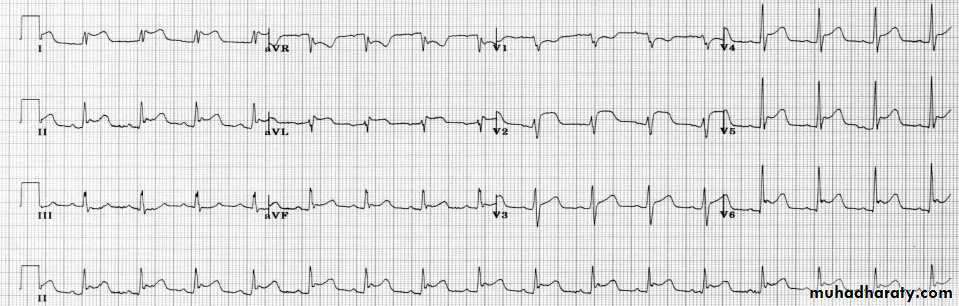
*LVH: ECG criteria:Voltage criteria1.Tall R in leftward leads(I aVL/V5/V6)>26mm 2.SV1/V2+RV5/V6 >35mm. confirmatory changes.(LV strain ( ST↓+T↓ )in leftward leads,LAD&LAE Causes(see text).
LVH(This ECG demonstrates many of the features of LV hypertrophy:*Markedly increased LV voltages: S wave in V1 + R wave in V6 > 35 mm; R wave in aVL > 26 mm.+confirmatory changes(*Left ventricular strain pattern: T wave inversion in the lateral leads V5-6, I and aVL*Left axis deviation&Signs of left atrial enlargement).
II.BBB Pattern:Either LBBB or RBBB. In BBB,The activation impulse has travel through the myocardium of the corresponding ventricle&as conduction through the myocardium is slower than conduction through Bundle of His- Purkinje fibres, the QRS complex become widened& often shows an extra deflection which reflects the rapid depolarisation of ventricle with normal bundle branch followed by the slower depolarisation of ventricle with blocked bundle branch.
*LBBB: is a cardiac conduction abnormality seen on ECGin which activation of the left ventricle is delayed→ LV to contract later than RV.

LBBBcharacterestics: Dominant S wave in V1 with broad, notched (‘M’-shaped) R wave in V6
ECGcriteria:1.Rhythm must be supraventricular in origin.2.The QRS duration must be ≥ 120ms( 0.12s).3.Dominant S wave in V1 appearing as QS , rS complex or just notched S wave & RsR' wave in lead V6&lead I(or as M-shaped or notched or just broad monophasic R).5.absent q wave in leftward leads except in aVL may be present.6. Associated features; *Appropriate discordance: the ST segments and T waves always go in the opposite direction to the main vector of the QRS complex. A concordant T wave may suggest ischemia or myocardial infarction. *Poor R wave progression in the chest leads.*Left axis deviation
Left Bundle Branch Block
LBBB.
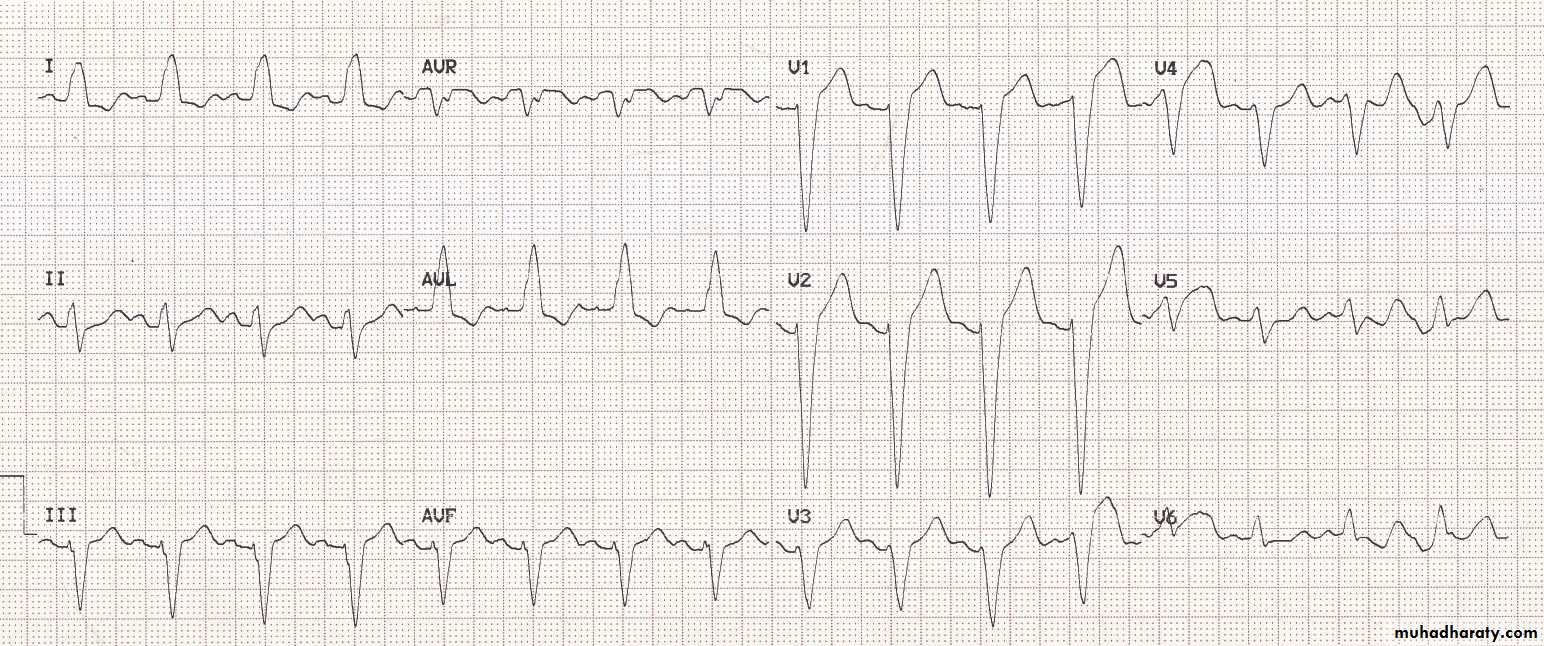
causes of LBBB :1.Aortic stenosis.2.Dilated cardiomyopathy.3.IHD.4.Primary disease of the conducting system. *RBBB:An interruption of impulse transmission through RBB →further delay in RV activation→undue delay of RV contraction after LV with classic ECG change
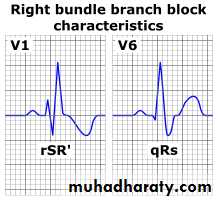
ECG characteristics of a typical RBBB showing wide QRS complexes with a terminal R wave in lead VI& slurred S wave in lead V6. ECG criteria: 1.rhythm must be supraventricular.2.The QRS duration must be equal or more than 120 ms(0.12s) 3. a terminal R wave in lead V1 appearing e. as broad R or as rR', rsR', rSR' or qR complex ,as notched or M-shaped R.4.There should be a slurred S wave in left leads I and V6.5. Associated features; *Appropriate discordance: the ST segments and T waves always go in opposite direction to the main vector of the QRS complex. A concordant T wave may suggest ischemia or infarction
.
Causes of RBBB:1..Right ventricular hypertrophy due to any cause 2.Pulmonary embolus 3.Ischaemic heart disease 4.Rheumatic heart disease 5.Myocarditis or cardiomyopathy. 6.Degenerative disease of the conduction system. 7.Congenital heart disease (e.g. atrial septal defect) 8.May be normal variant III.Ischaemic pattern: Horizontal ST seg or dowen slopping STseg. depression . IV.Myocardial infarction pattern: regional convex STseg.↑ ±T ±abnormal Q . V.Acute pericarditis : Concave ST↑ in almost all leads i,e diffuse changes as in this ECG
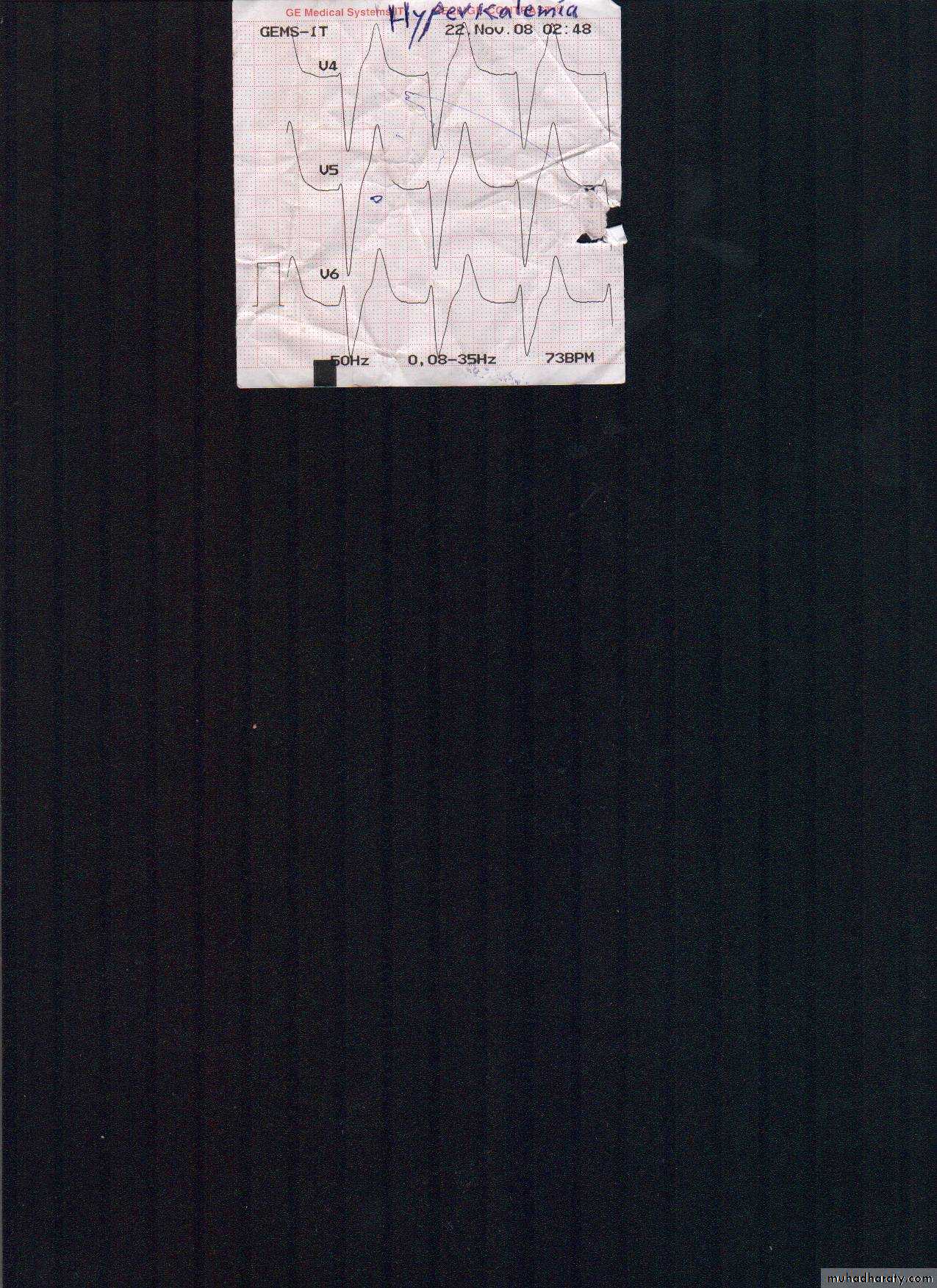
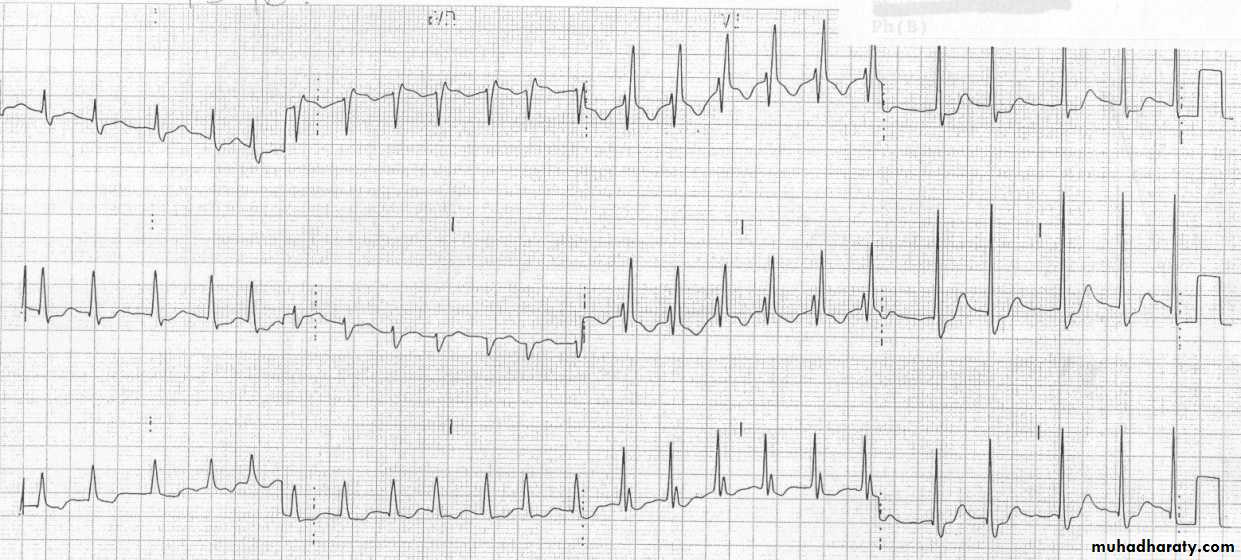
VI.Arrhythmic patterns &AV conduction VII.Nonspecific ST/T changes : the specificity of ST-T and U wave abnormalities is provided more by the clinical circumstances in which the ECG changes are found than by the particular changes themselves hence termed nonspecific ST-T wave abnormalities, is frequently used when the clinical data are not available to correlate with the ECG findings. This does not mean that the ECG changes are unimportant&their cause needs to be searched for.Possible causes: 1.Intrinsic myocardial disease (e.g., myocarditis, ischemia, infarction, infiltrative or myopathic processes).2.Drugs (e.g., digoxin, quinidine, tricyclics, and many others) .3.Electrolyte abnormalities of potassium, magnesium, calcium 4.Neurogenic factors (e.g.,stroke,sub-arachnoid hemorrhage, trauma, tumor, etc.).5.Metabolic factors (e.g., hypoglycemia,hyperventilation)&6. &even as spurious changes in females. ECG changes in hyperkalemia(early changes).1.Tall, peaked T waves with a narrow base, best seen in precordial leads[4] 2.Shortened QT interval 3.ST-segment depression

ECG in hyperkalemia.
ECG changes in severe hypokalemia(ST↓&T↓+prominent U-wave+long QT-interval.
VIII:Other rare pattens:Long QTsynd.-preexcitation synd. hypothermia&low voltage ECG.
ST/T changes+J-waves(Diagnostic of hypothermia)