VALVULARHEART DISEASE
د. محمد سعيد عبد الزهره
What Is Valvular Heart Disease?
Heart valve disease occurs when your heart's valves do not work the way they should.How Do Heart Valves Work?
MAINTAIN ONE-WAY BLOOD FLOW THROUGH YOUR HEARTThe four heart valves make sure that blood always flows freely in a forward direction and that there is no backward leakage.
Heart Valves
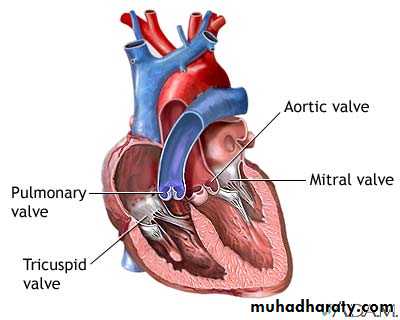
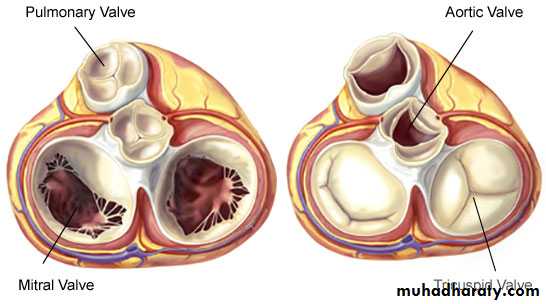
ANY DISEASE OF THESE VALVES ARE CALLED AS
VALVULAR HEART DISEASE!Types of valve disease
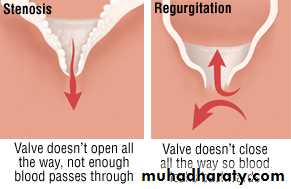
Valvular Stenosis
THE VALVE OPENING NARROWSthe valve leaflets may become fused or thickened that the
valve cannot open freely obstructs the normal flow of blood
EFFECTS:
the chamber behind the stenotic valve is subject to greater stress must generate more pressure (work hard) to force blood through the narrowed opening
initially, the compensates for the additional workload by
gradual hypertrophy and dilation of the myocardium
heart failure
Valvular Regurgitation
LEAKAGE OR BACKFLOW OF BLOOD RESULTS FROM INCOMPLETE CLOSURE OF THE VALVEdue to:
• Scarring and retraction of valve leaflets
OR
• Weakening of supporting structures
EFFECTS:
causes the to pump the same blood twice(as the blood comes back into the chamber)
the dilates to accommodate more blood
ventricular dilation and hypertrophy eventually leads to
heart failure
Principal Causes
• Valve stenosis• Valve regurgitation
• Congenital
• Rheumatic carditis
• Senile degeneration
• Congenital
• Rheumatic carditis (acute or chronic)
• Infective endocarditis
• Valve ring dilatation
(e.g. dilated cardiomyopathy)
• Syphilitic aortitis
• Traumatic valve rupture
• Damage to chordae and
• papillary muscle (e.g. MI)
• Senile degeneration
Valvular Heart Disease
• MITRAL STENOSIS• MITRAL REGURGITATION
• AORTIC STENOSIS
• AORTIC REGURGITATION
• TRICUSPID STENOSIS
• TRICUSPID REGURGITATION
• PULMONARY STENOSIS
• PULMONARY REGURGITATION
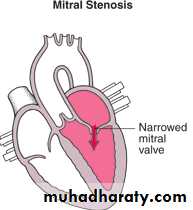
1. MITRAL STENOSIS
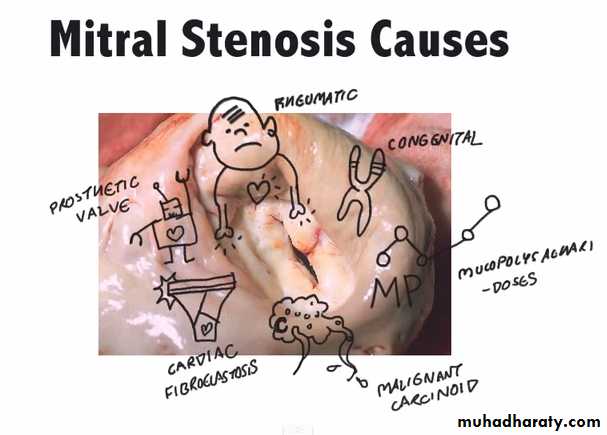
Aetiology
Almost always rheumatic in originOlder people: can be caused by heavy calcification of mitral valve congestion
Congenital (rare)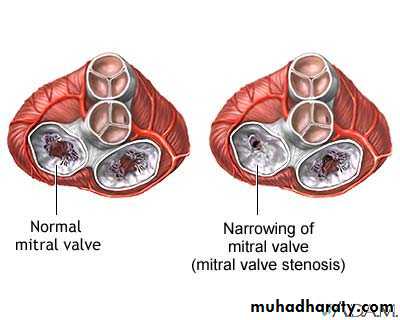
Pathophysiology
Normal mitral valve orifice is 5cm2 in diastole & may be reduced to 1cm2 in severe mitral stenosis



Pathophysiology
Atrial fibrillation due toprogressive dilatation
of the LA is very common.
Its onset often precipitates
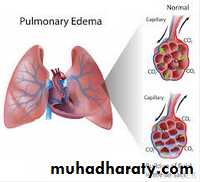
pulmonary oedema
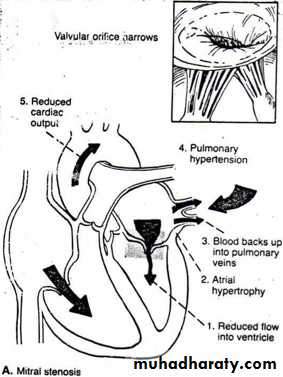
In contrast, a more gradual rise in left atrial pressure tends to cause an increase in pulmonary vascular resistance pulmo. HTN RVH, TR RHF


Atrial fibrillation due to
progressive dilatationof the LA is very common.
Its onset often precipitates
pulmonary oedema
In contrast, a more gradual rise
In left atrial pressure tends to cause
an increase in pulmonary vascular
resistance pulmo. HTN RVH, TR RHF
Pathophysiology
Narrowing of mitral valve CO
O2/CO2 exchange
(fatigue, dyspnea, orthopnea)
Left ventricular atrophy
pulmonary congestion
pulmonary pressure
left atrial pressure
Hypertrophy left atrium
blood flow to left ventricle
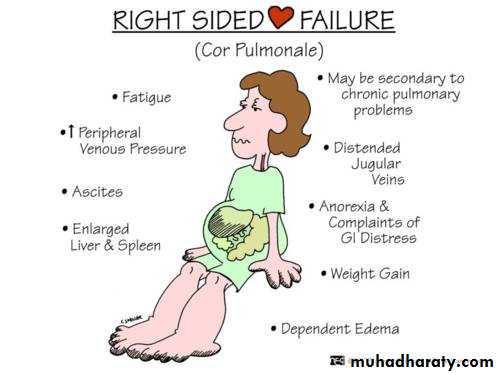
Right-sided failure
Fatigue
Clinical features
SymptomsBreathlessness, cough (pulmonary congestion)
Chest pain (pulmonary hypertension)
Hemoptysis (pulmonary congestion or hypertension)Fatigue (low cardiac output)
Oedema, ascites (right heart failure)Palpitation (atrial fibrillation)
Thromboembolic complicationsClinical features
SignsAtrial fibrillation
Mitral facies (abnormal flushing of the cheeks that occurs from cutaneous vasodilation in the setting of severe mitral valve stenosis)
Auscultation - Loud first heart sound, opening snap
(created by forceful opening of mitral valve)
- Mid-diastolic murmur (apex)
Crepitations, pulmonary edema, effusions (raised pulmonary capillary pressure)
RV heave, loud P2 (pulmonary hypertension)

Mitral stenosis
…Lub Hoot…
InvestigationsECG: - right ventricular hypertrophy tall R waves
Chest x-ray: - enlarged LA & appendage
- signs of pulmonary venous congestion
ECHO: - thickened immobile cusps
- reduced valve area- enlarged LA
- reduced rate of diastolic filling of LV
Doppler: - pressure gradient across mitral valve
Cardiac catheterization: - coronary artery disease
- pulmonary artery pressure
- mitral stenosis and regurgitation
Management
MedicallyAnticoagulant
• To reduce the risk of systemic embolism
Digoxin, beta blockers, or rate limiting calcium antagonists
• To control ventricular rate in atrial fibrillation
• To control pulmonary congestion
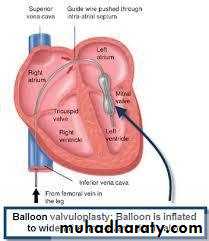
Surgically
Mitral balloon valvuloplasty***
Mitral valvotomy
Valve replacementBalloon mitral valvuloplasty
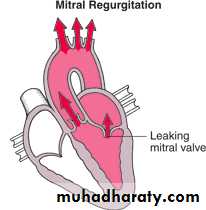
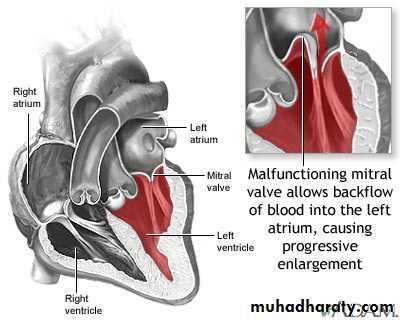
2. MITRAL REGURGITATION
Mitral regurgitation
Incomplete closure of mitral valve
AetiologyRheumatic disease is the principal cause (in countries where disease is common)
Mitral valve prolapse
Dilatation of the LV and mitral valve ring (e.g. coronary artery disease, cardiomyopathy)Damage to valve cusps and chordae (e.g. rheumatic heart disease, endocarditis)
Ischaemia or infarction of papillary muscle (MI)Pathophysiology
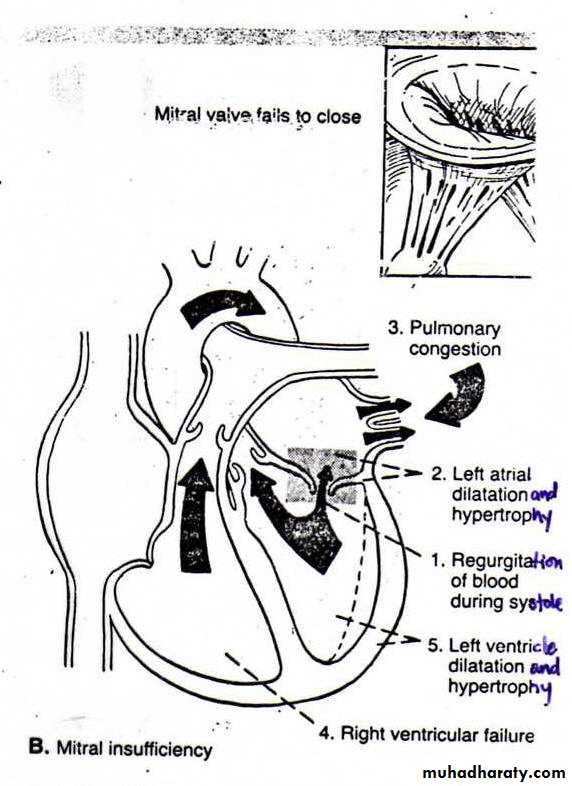
Pathophysiology
Incomplete closure of mitral valve vol. of blood ejected by left ventricle
Left atrial pressure
Right-sided heart failure
Left atrial hypertrophy
CO
Pulmonary pressure
Backflow of blood to the left atrium
Right ventricular pressure
mitral valve prolapse
A.k.a ‘floppy’ mitral valveOne of the most common cause of mild mitral regurgitation
Caused bycongenital anomalies
degenerative myxomatous changes
feature of connective tissue disorders like Marfan’s syndrome
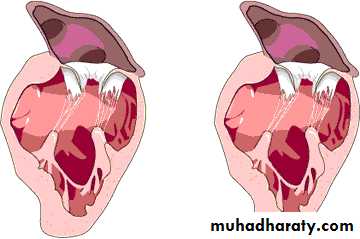
Mitral regurgitation
mitral valve prolapseMildest form:
Valve remains competent but bulges back into atrium during systole mid-systolic click but no murmur
In the presence of regurgitant valve:
Click is followed by a late systolic murmur, which lengthens as the regurgitation becomes more severeSevere form:
Progressive elongation of chordae tendinae increasing regurgitation Chordal rupture severe regurgitationMitral regurgitation
Clinical Manifestations
• Fatigue & weakness – due to CO – predominant complaint
• Exertional dyspnea & cough – pulmonary congestion
• Palpitations – due to atrial fibrillation (occur in 75% of pts.)
• Edema, ascites – Right-sided heart failure
Symptoms
Clinical Manifestations
• Atrial fibrillation• Cardiomegally
• Apical pansystolic murmur +/- thrill
• Soft S1, apical S3
• Signs of pulmonary venous congestion (crepitations, pulmonary edema, effusions)
• Signs of pulmonary hypertension & right heart failure
Signs
Mitral regurgitation
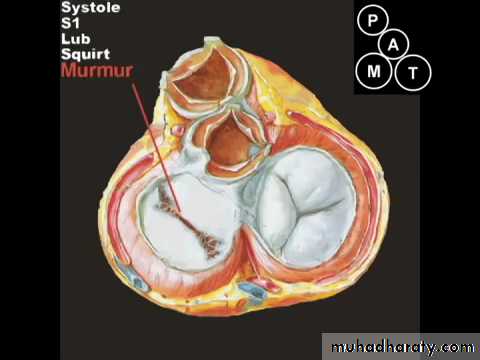
…Hoot Dub…
Investigations
ECG: - left atrial hypertrophy
• - left ventricular hypertrophy
Chest x-ray: - enlarged LA,LV
- pulmonary venous congestion
• - pulmonary oedema
ECHO: - dilated LA,LV
- structural abnormalities of mitral valve (e.g. prolapse)
Doppler: - detects and quantifies regurgitation
Cardiac catheterization: - dilated LA,LV- mitral regurgitation
- pulmonary hypertension
- coexisting coronary artery disease
Management
MedicallyVasodilators (e.g. ACE inhibitors)
Diuretics
If atrial fibrillation presents,
Anticoagulant
Digoxin
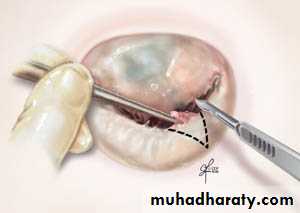
Surgically
Mitral valve repair
OR
Mitral valve replacement
To treat
mitral valve
prolapse
3. AORTIC STENOSIS
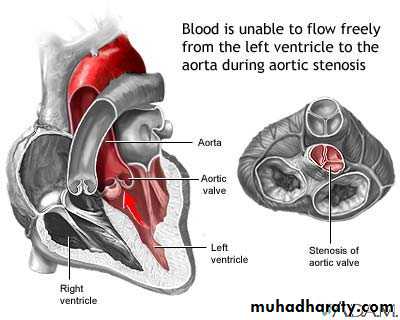
Aortic Stenosis
Narrowing of the aortic valveAetiology
INFANTS, CHILDREN, ADOLESCENTS
Congenital aortic stenosis
Congenital subvalvular aortic stenosis
Congenital subvalvular aortic stenosis
YOUNG ADULTS TO MIDDLE-AGED
Calcification and fibrosis of congenitally bicuspid aortic valveRheumatic aortic stenosis
MIDDLE-AGED TO ELDERLY
Senile degenerative aortic stenosisCalcification of bicuspid valve
Rheumatic aortic stenosis
Pathophysiology
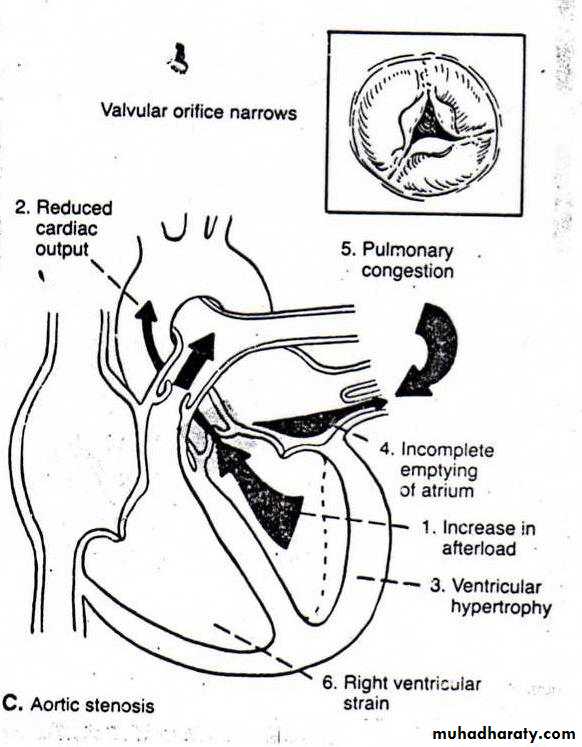
Pathophysiology
Stiffening/Narrowing of Aortic ValveIncomplete emptying of left atrium
Left ventricular hypertrophy
Pulmonary congestion
Compression of coronary arteries
Right-sided heart failure
CO
Myocardial O2 needs
Myocardial ischemia
(chest pain)
O2 supply
Clinical features
Symptoms
Mild or moderate stenosis: usually asymptomatic
Exertional dyspnea
Angina (due to demands ofhypertrophied LV)
Exertional syncope
Sudden deathEpisodes o acute pulmonary oedema
CARDINALSYMPTOMS
CO fails to rise
to meet demand
Clinical features
SignsEjection systolic murmur
Slow-rising carotid pulse
Thrusting apex beat (LV pressure overload)
Narrow pulse pressureSigns of pulmonary venous congestion (e.g. crepititions)
InvestigationsECG: - left ventricular hypertrophy
- left bundle branch block
Chest x-ray: - may be normal
- enlarged LV & dilated ascending aorta (PA view)
- calcified valve on lateral view
ECHO: - calcified valve with restricted opening, hypertrophied LV
Doppler: - measurement of severity of stenosis
- detection of associated aortic regurgitation
Cardiac catheterization: - to identify asst. coronary artery disease
- may be used to measure gradientbetween LV and aorta
Management
Asymptomatic aortic stenosis kept under review
Moderate/severe stenosis evaluated every 1-2 years with Doppler echocardiography (to detect progression in severity)
Symptomatic severe aortic stenosis valve replacement
Congenital aortic stenosis aortic balloon valvuloplastyAtrial fibrillation or post valve replacement with a mechanical prosthesis anticoagulant
(as the development of angina, syncope,
symptoms of low CO or heart failure
has a poor prognosis and is an indication
for prompt surgery)
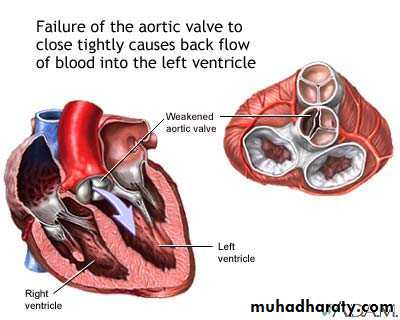
4. AORTIC REGURGITATION
CausesCongenital:
Bicuspid valve or disproportionate cusps
Acquired:
Rheumatic disease
Infective endocarditis
Trauma
Aortic dilatation (marfan’s syndrome, aneurysm, dissection, syphilis)
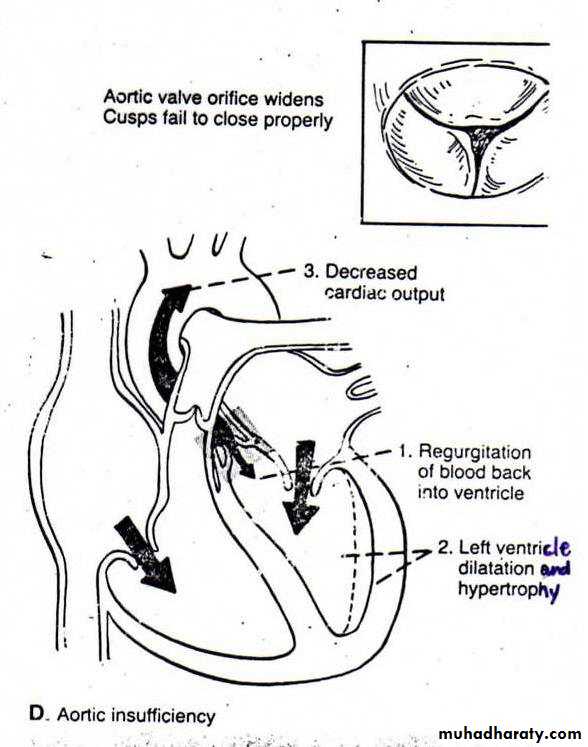
Pathophysiology
PathophysiologyIncomplete closure of the aortic valve
Backflow of blood to Left ventricle
Left ventricular hypertrophy & dilation
Left atrial pressure
Left-sided heart failure
(late stage)
Left atrium hypertrophy
CO
Pulmonary pressure
Right-sided heart failure
Right ventricular pressure
Clinical features
Symptoms
Mild or moderate aortic regurgitation:
Usually asymptomatic
Awareness of heartbeat, ‘palpitations’
Severe aortic regurgitation:Breathlessness
Angina
particularly when lying on the left side,
which results from increased in stroke volume
(because compensatory ventricular
dilatation&hypertrophy occur)
Clinical features
Pulses:Large volume or ‘collapsing’ pulse
Low diastolic and increased pulse pressure
Bounding peripheral pulse
Capillary pulsation in nail beds: Quincke’s sign
Femoral bruit(‘pistol shot’): Duroziez’s sign
Head nodding with pulse: de Musset’s sign
Murmurs:
Early diastolic murmur
Systolic murmur (increased stroke volume)
Austin Flint murmur (soft mid-diastolic)
Other signs:
Displaced, heaving apex beat (volume overload)Pre-systolic impulse
4th heart sound
Crepitations (pulmonary venous congestion)
Signs
characteristic murmur is best heardto the left sternum during held expiration
Investigations
ECG: initially normal,later left ventricular hypertrophy & T-wave inversion
Chest x-ray: - cardiac dilatation, maybe aortic dilatation
• - features of left heart failure
ECHO: - dilated LV
- hyperdynamic LV
- fluttering anterior mitral leaflet
Doppler: - detects reflux
Cardiac catheterization: - dilated LV
• - aortic regurgitation• - dilated aortic root
Management
Treatment may be required for underlying conditions, such as endocarditis or syphilisAortic regurgitation with symptoms aortic valve replacement (may be combined with aortic root replacement and coronary bypass surgery)
Asymptomatic patients annually follow up with echocardiography for evidence of increasing ventricular size
Systolic BP should be controlled with vasodilating drugs, such as nifedipine or ACE inhibitors

5. TRICUSPID STENOSIS
Tricuspid Stenosisusually occurs together with aortic or mitral stenosis
may be due to rheumatic heart disease (<5%)
blood flow from right atrium to right ventricle right ventricular output
left ventricular filling co
systemic pressure
Tricuspid StenosisSymptoms
symptoms of right-sided heart failure
- hepatomegaly
- ascites
- peripheral edema
- neck vein engorgement
co – fatigue, hypotension
Signs
Raised JVPMid-diastolic murmur (best heard at lower left or right sternal edge)
Tricuspid StenosisManagement
Valve replacement
ValvotomyBalloon valvuloplasty
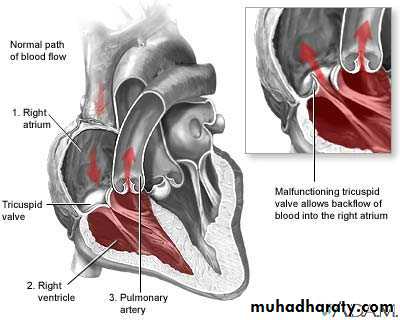
6. TRICUSPID REGURGITATION
Tricuspid Regurgitationcommon, and is most frequently ‘functional’ as a result of enlargement of right ventricle
an insufficient tricuspid valve allows blood to flow back into the right atrium venous congestion & right ventricular output blood flow towards the lungs
primary
Rheumatic heart diseaseEndocarditis, particularly in injection drug-users
Ebstein’s congenital anomalysecondary
Right ventricular dilatation due to chronic left heart failure (‘functional tricuspid regurgitation’)
Right ventricular infarction
Pulmonary hypertension (e.g. cor pulmonale)Tricuspid Regurgitation
causes
Tricuspid RegurgitationSymptoms
Usually non-specific
Tiredness (reduced forward flow)
Oedema
Hepatic enlargement (venous congestion)
SignsRaised JVP
Pansystolic murmur (left sternal edge)
Pulsatile liverTricuspid Regurgitation
ManagementCorrection of the cause of right ventricular overload (if TR is due to right ventricular dilatation)
Use of diuretic and vasodilator treatment of CCF
Valve repair
Valve replacement7. PULMONARY STENOSIS
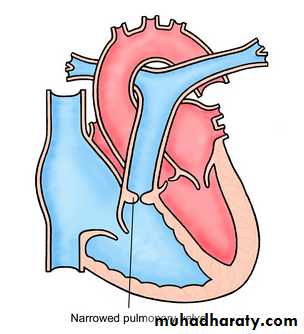
Pulmonary Stenosis
Symptoms
Fatigue, dyspnea on exertion, cyanosis
Poor weight gain or failure to thrive in infants
Hepatomegaly, ascites, edemaSigns
Ejection systolic murmur (loudest at the left upper sternum & radiating towards the left shoulder)Murmur often preceded by an ejection sound (click)
May be wide splitting of second heart sound (delay in ventricular ejectionMay be a thrill (best felt when patient leans forward and breathes out)
Investigations
ECG: - right ventricular hypertrophy
Chest x-ray: - post-stenotic dilatation in the pulmonary artery
Doppler echocardiography is the definitive investigation
ManagementMild to modearate isolated pulmonary stenosis is relatively common and does not usually progress or require treatment
Severe pulmonary stenosis percutaneous pulmonary balloon valvuloplasty
ORsurgical valvotomy
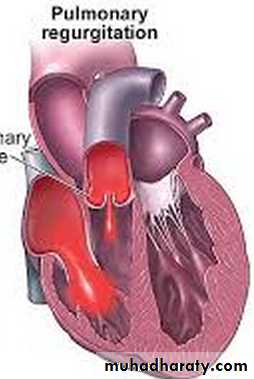
8. PULMONARY REGURGITATION
Pulmonary RegurgitationA rare condition
Usually associated with pulmonary hypertension
which may be• Secondary of the disease of left side of the heart
• Primary pulmonary vascular disease
• Eisenmenger’s syndrome
Blood flows back into right ventricle right ventricle
and atrium hypertrophy symptoms of right-sided
heart failure
• Trivial PR is a frequent finding in normal individuals and has no clinical significance