RHEUMATOID ARTHRITIS
Dr.Fakhir Yousif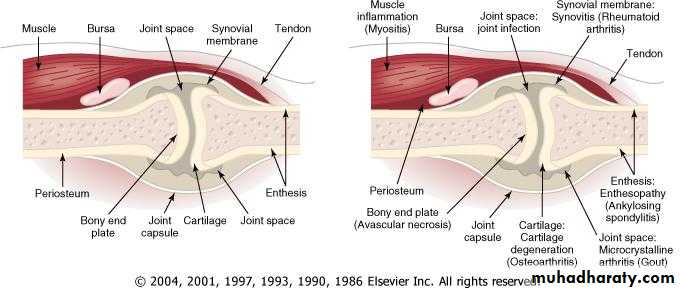
Definition
Rheumatoid factor (RF), an immunoglobulin M (IgM) auto-antibody against the Fc portion of an IgG molecule first described by Waaler in 1940, is the main serologic marker, found in 75% to 80% of patients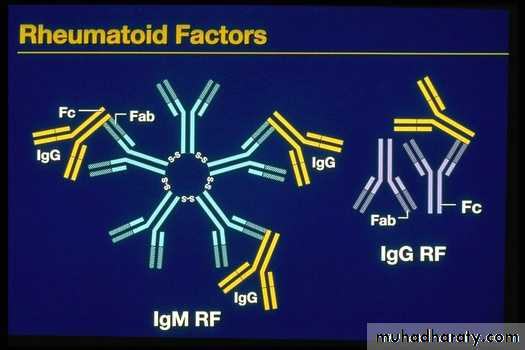
Epidemiology
RA occurs throughout the world and in all ethnic groups. The prevalence is lowest in black Africans and Chinese, and highest in the Pima Indians of Arizona. In Caucasians it is around 1.0-1.5% with a female:male ratio of 3:1. Before the age of 45, the female:male ratio is 6:1. Prevalence increases with age, with 5% of women and 2% of men over 55 years being affected.Etiology
Genetic factors in RA are important in defining disease susceptibility and severity.
Family studies have demonstrated an increased risk for disease in siblings of persons affected with RA. Concordance has been found to be 12% to 15%
in monozygotic and 4% in dizygotic twins, strong evidence for a major influence of genetic factors in disease causation .
Enviromental
viruses (e.g., parvovirus B19, Epstein-Barr virus), Mycoplasma, and other bacteria (e.g., streptococci).Possible auto-antigens include type 2 collagen proteoglycan, chondrocyte antigens, heat shock proteins .
Urbanization
has a major impact on incidence & severity of R.A.cigarete smoking
11
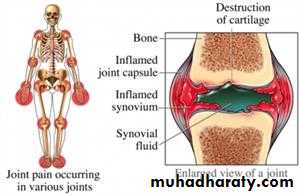
Histopathology
. In the early months of RA, edema, angiogenesis, hyperplasia of synovial lining, and inflammatory infiltrate are already present. Once the disease enters a more chronic phase, massive hyperplasia, mainly of type A synovial cells, and subintimal mononuclear cell infiltrationThe synovium of RA assumes the appearance of a reactive lymph node because of the extensive infiltration by plasma cells, macrophages, and lymphocytes in the form of large lymphoid follicles.
One characteristic feature of RA is the invasion of and damage to cartilage, bone, and tendons by an infiltrating inflammatory synovial tissue mass called the pannus
Clinical Characteristics of Rheumatoid Arthritis
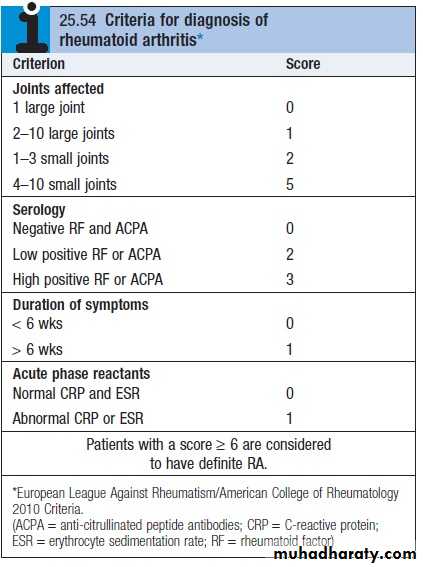
Diagnosis of RA is made with four or more of the following
Morning stiffness (> 1 hourArthritis of three or more joint areas
Arthritis of hand joints
Symmetrical arthritis
Rheumatoid nodules
Seropositive - Rheumatoid factor OR Anti-CCP (citrullinated C peptide)
Radiological changes
Duration of 6 weeks or more
Joints Affected :
Typically involves elbows, wrists, MCP, and PIP joints1st & 2nd cervical vertebrae frequently involved
Unaffected joints :
Thoracolumbar spine, DIPs & SI joints
Rheumatoid Arthritis: PIP Swelling
Swelling is confined to the area of the joint capsule
Synovial thickening feels like a firm sponge
19
Rheumatoid HAND
An across-the-room diagnosisProminent ulnar deviation in the right hand
MCP and PIP swelling in both hands
MCP sublaxation
Synovitis of left wrist
20
Rheumatoid arthritis: swan-neck and boutonnière deformity, hand

21
Nonreducible flexion at the PIP joint with concomitant hyperextension of the DIP joint of the finger (boutonniere deformity, occurs as a consequence of synovitis with stretching of, or rupture of, the PIP joint through the central extensor tendon with concomitant volar displacement of the lateral bands.
Hyperextension at the PIP joint with flexion of the DIP joint (swan-neck deformity, may be initiated by disruption of the extensor tendon at the DIP joint with secondary shortening of the central extensor tendon and hyperextension of the PIP joint,
Rheumatoid arthritis: arthritis mutilans, hand (clinical and radiograph)

24
Rheumatoid arthritis: ruptured right popliteal cyst

25
EXTRA-ARTICULAR MANIFESTATIONS OF RHEUMATOID DISEASE
Haematological
AnaemiaThrombocytosis
Eosinophilia
Lymphatic
Splenomegaly
Felty's syndromeOcular
EapiscleritisScleritis
Scleromalacia
Keratoconjunctivitis sicca
Vasculitis
Digital arteritisUlcers
Pyoderma gangrenosum
Mononeuritis multiplex
Visceral arteritis
Cardiac
Pericarditis
Myocarditis
Endocarditis
Conduction defects
Coronary vasculitis
Granulomatous aortitis
Pulmonary
NodulesPleural effusions
Fibrosing alveolitis
Bronchiolitis
Caplan's syndrome
Neurological
Cervical cord compressionCompression neuropathies
Peripheral neuropathy
Mononeuritis multiplex
Cutaneous features
Subcutaneous rheumatoid nodules occur almost exclusively in seropositive patients, usually at sites of pressure or friction such as the extensor surfaces of the forearm, sacrum, Achilles tendon and toes
Rheumatoid arthritis: subcutaneous nodule, olecranon

37
Rheumatoid arthritis: episcleritis
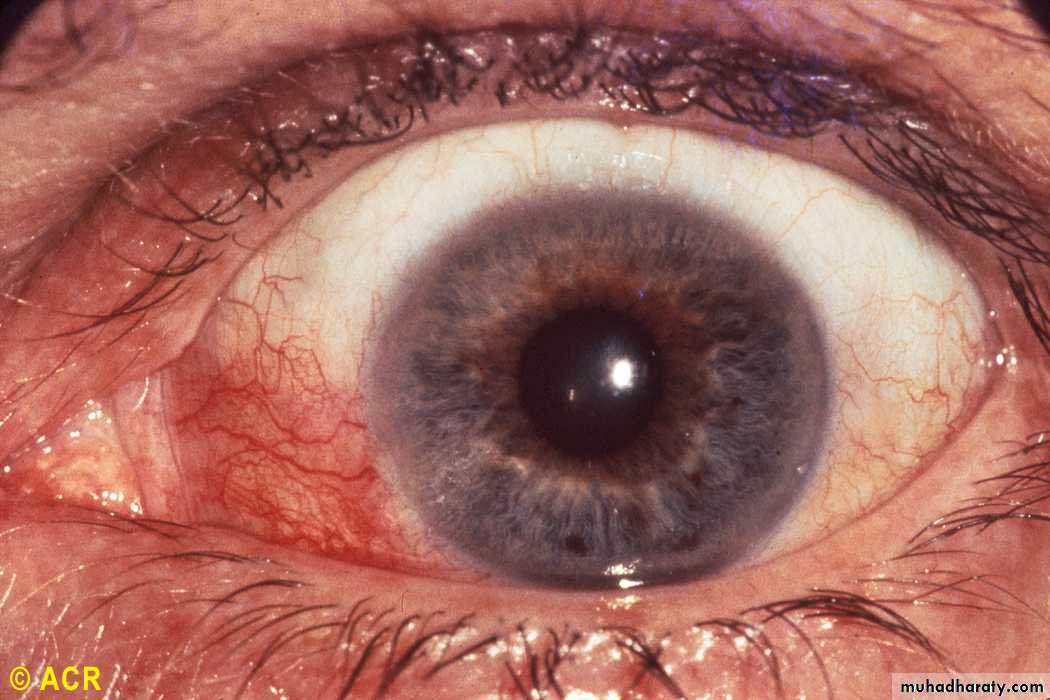
38
Rheumatoid arthritis: vasculitis and gangrene, fingers

39
Rheumatoid arthritis: pulmonary nodules

40
Laboratory Tests
Raised inflammatory markers . Reasonable correlation with clinical activityMild anemia & thrombocytosis
S. Rheumatoid factor (Agglutination method). Positive in near 70-80% cases (western countries). Not specific
Anti-CCP (citrulline – containing proteins) antibodies. Similar sensitivity to RF but more specific (up to 95%)
41
Examination of joint fluid
the most helpful laboratory procedure. The fluid is inflammatory, with more than 10,000 white blood cells and a predominance of polymorphonuclear leukocytes, typically 80% or more. Rheumatoid factor, an IgM antibody directed to IgG, is found in 80 to 90% of patients with RA.... XR-Findings
Peri articular osteopeniaMarginal erosions (at least months of persistent activity)
Joint space narrowing (cartilage loss)
Ankylosis (wrists)
Deformities
43
A. Soft-tissue swelling, no erosions
B. Thinning of the cortex on the radial side and minimal joint space narrowing
C. Marginal erosion at the radial side of the metacarpal head with joint space narrowing
Joint damage progression in R.A. hand
44
Prognosis
The following factors at presentation are associated with a poor prognosis: higher baseline disabilityfemale gender
involvement of MTP joints
positive rheumatoid factor
disease duration of over 3 months.
45