



Open bite malocclusion.
Deep bite malocclusion.
Vertical orthodontic problems
Classification
Based on dental or skeletal components
Dental
Skeletal
Based on location
Anterior
Posterior
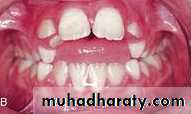
Open bite malocclusion
Anterior open bite: lack of vertical overlapment and lack of contact between upper and lower incisors when the mandible is brought into full occlusion.
Open bite malocclusion

Anteroir open bite

Edge to edge incisor relationship
Posterior open bite: lack of contact between upper and lower posterior teeth in centric occlusion. It may be unilateral or bilateral
Open bite malocclusion

Anterior open bites occur more often than posterior open bites.
Majority of anterior open bites are dental in nature.Anterior open bite
Problems associated with AOB
Esthetically unattractive particularly during speech when the tongue is pressed between the teeth and lips.
Difficulties during speech (lisping and distortion of /th/,/sh/,/ch/ sounds).
Tongue thrust swallowing which is physilogic adaptation to help patient seal off the front of mouth during swallowing.
Masticatory problems with difficulty to incise.
Tongue thrust
Anterior open biteEtiology of AOB
Environmental factors:
• Thumb/digit sucking habit.
• Forward resting tongue posture.
• Mouth breathing.
• Iatrogenic factor e.g. extruding molars during orthodontic treatment.
Abnormally increased tongue size.
Abnormal skeletal growth pattern.Sucking habits
Children who produce 6 h or more of pressure, can cause significant malocclusions.characterized by flared and spaced maxillary incisors, lingually positioned lower incisors, anterior open bite and a narrow upper arch.
This malocclusion arise from a combination of direct pressure on the teeth and an alteration in the pattern of resting cheek and lip pressures.
Forward tongue posture: This could alter the equilibrium pressures of lips and tongue on anterior teeth resulting in proclination and spacing of upper and lower incisors.
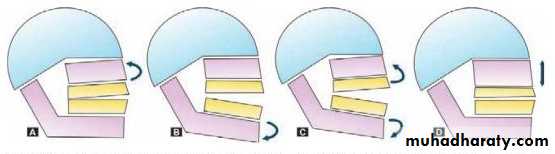
Abnormal skeletal growth pattern
skeletal anterior open bite may result from
• Upward maxillary rotation.
• Downward mandibular rotation.
• Combination of Downward mandibular rotation and Upward maxillary rotation.
• Vertical maxillary excess.
•
Thorough clinical and radiographic evaluation is needed to decide whether the condition is dental or skeletal in origin.
Diagnosis
Clinical features of dental anterior open bite
Intraoral featuresOpen bite limited to anterior segment, often asymmetrical
1Proclined maxillary and/or mandibular incisors
2
Spacing between maxillary and/or mandibular incisors
3
Narrow maxillary arch is a possibility
4
Extraoral features
No unusual features


Clinical features of skeletal anterior open bite
Intraoral featuresMild crowding with upright incisors
1Open bite may involve premolar teeth
2
Generally has occlusal contacts only at molars with both maxillary and mandibular occlusal planes diverging anteriorly
3

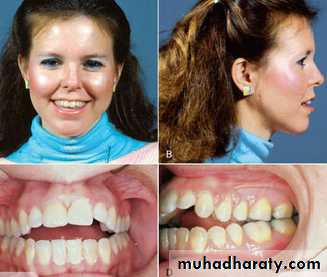
Clinical features of skeletal anterior open bite
Extraoral features
Long face due to increased lower anterior facial height
1Incompetent lips
2
Steep mandibular plane angle
3

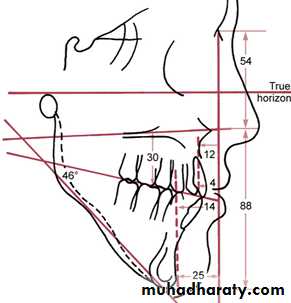
Cephalometric features of skeletal AOB
(long face syndrome)• Increased mandibular plane angle.
• Increased gonial angle.
• Increased basal plane angle.
• Increased anterior facial height.
• increased upper posterior dentoalveolar height.
Diagnosis

Treatment plan
Successful treatment planning of open bites should consider:
Etiology of open bite (persistence of the cause will limit correction of AOB).
Dental and/or skeletal components of AOB.
Age of the patient.
Treatment plan
If Open bite is associated with habits the first step of treatment should be directed towards cessation of the habit.
Skeletal open bite in preadolescent children (mixed dentition) can be managed with growth modification appliances.
Open bites that persist until adolescence (with no habits) usually have a skeletal component contributing to the problem and are best managed by intrusion of upper molars.
Sever open bites in adults are best treated with orthognathic surgery.
Treatment
Dental AOB associated with habits:Thumb sucking
Primary dentition: in children with good facial proportions no treatment is needed since there is a good chance of spontaneous correction with incisor eruption.
Thumb sucking
Mixed dentition (preadolescent children):• Counseling.
• Reminder therapy: adhesive bandage around finger.
• Mechanically obstructing hand with sleeping gown or bandage loosely wrapped around elbow.

Thumb sucking
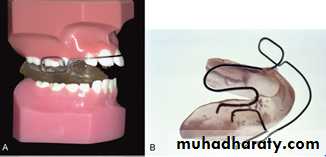
• Appliance therapy: fixed appliance is indicated due to lack of patient compliance. The appliance acts as a reminder and provides mechanical obstruction for sucking.
The preferred type is maxillary lingual arch with an anterior crib device.

Thumb sucking
Quad helix appliance can be used if there is posterior crossbite for expansion.It is better to leave the crib in place for 6 months after the habit has been eliminated.

Thumb sucking
The open bite associated with sucking in children with normal jaw relationships often resolves after sucking stops and the remaining permanent teeth erupt.An appliance may be needed for expansion of constricted maxillary arch.
Flared and spaced incisors may need retraction using removable Hawley appliance.


Forward tongue posture
Fixed appliance with lingual spurs or crib this will aid in correcting tongue posture .Removable or fixed orthodontic appliance is then needed for open bite correction.


Treatment of skeletal open bite in preadolescents
Vertical facial growth is the last to stop and may continue until late teens and early 20s.Early intervention in young children is not recommended and its better to delay treatment until preadolescence, or even adolescence the growth of the patient should be assessed using cervical vertebral maturation staging.
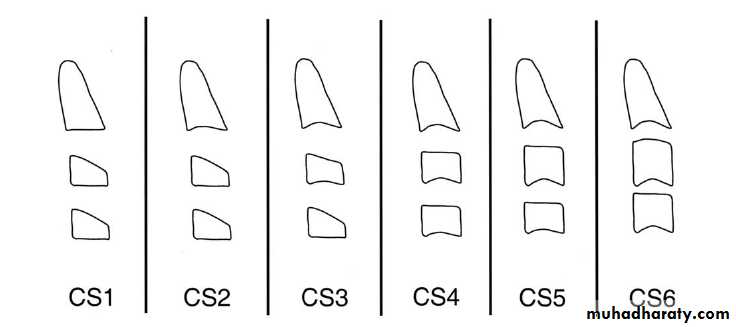
Treatment of skeletal open bite in preadolescents
Skeletal AOB (long face) can be treated during growth period by controlling posterior vertical growth of maxilla so that the mandible would rotate in an upward and forward direction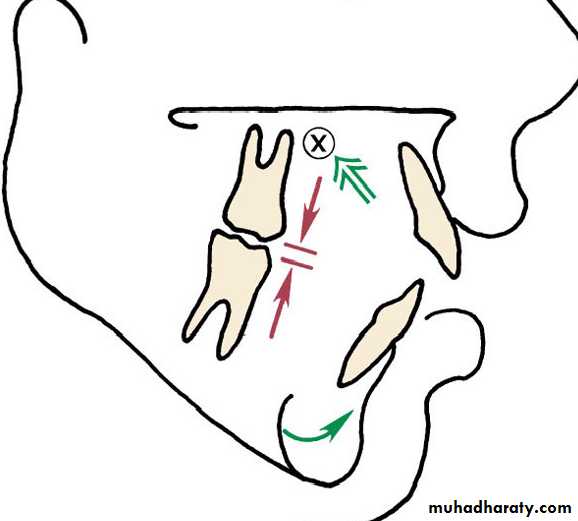
Treatment of skeletal open bite in preadolescents
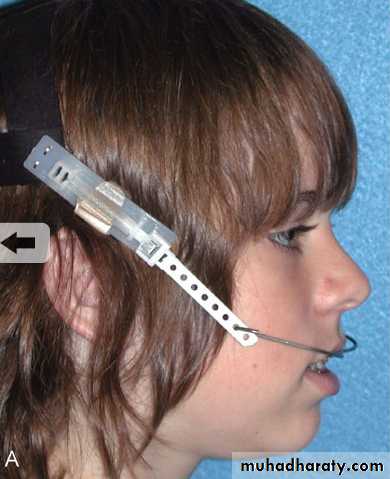
High pull headgear to molars: this will inhibit eruption of maxillary posterrior teeth while the anterior teeth are allowed to eruptThe appliance should be worn 14 hours/day with a force greater than 12 ounces per side.
Treatment of skeletal open bite in preadolescents
• Functional appliance with bite blocks like Franckle VI and open bite bionator.The bite blocks inhibit eruption of posterior teeth and vertical descent of maxilla and this is achieved by fabricating the appliance with the bite opened past the normal resting vertical dimension.

Correction of AOB in adolescents
If AOB is caused by thumb sucking, which is rare in adolescents, habit should be stopped first using fixed habit breaker.Mild open bites can be successfully treated using fixed orthodontic appliance.
placing anterior brackets more gingivally than posterior brackets and using box elastics encircling upper and lower incisors can help in closing open bite by extrusion of the anteriors.


Correction of AOB in adolescents
In majority of cases AOB is the result of elongation of posterior teeth (particularly upper molars) and downward-backward rotation of the mandible.these cases are best treated by intruding upper molars using temporary anchorage devices like miniscrews or miniplates which provides skeletal anchorage for tooth movement.




Correction of AOB in adults
For esthetic and more stable results AOB in adults are treated by intrusion of posterior segment since elongating anterior teeth to close the open bite makes facial appearance worse.
Correction of AOB in adults
In moderately sever cases this is achieved using bone screws attached with NiTi spring to a bonded occlusal splint (Erverdi plate)that is fabricated off the palate.Each 0.5mm of posterior intrusion provides 1mm closure of AOB.


Correction of AOB in adults
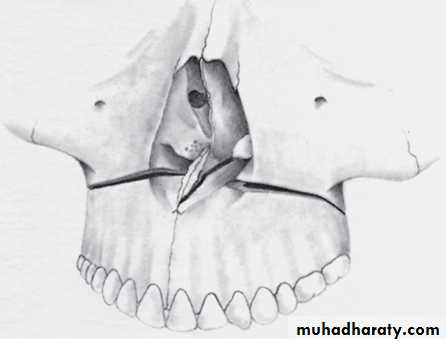
Sever cases of open bite that are associated with increased lower facial third (skeletal AOB) should be treated surgically.Surgery involves LeFort I osteotomy to move the maxillary posterior segment up and the anterior segment down.
This allow the mandible to rotate up and forward to close the open bite.
Correction of AOB in adults

Presurgical alignment and leveling of segments

Postsurgical orthodontics with vertical elastics to maintain correction of openbite
Retention after AOB correctionIf oral habit continues after orthodontic treatment, relapse is guaranteed.
In other patients where open bite is not caused by oral habits, the key to retention is to control the eruption of upper molars this is achieved using 2 approaches:
• Maxillary retainer with bite blocks (open bite bionator) to impede eruption.
• High-pull head gear .

Retention after AOB correction
These retainers should be worn full time for the first 3-4 months.
Continued on part time basis for at least 12 months.
In significant growth remains, continued part time (nighttime retainer) through the late teens until completion of growth.

Posterior open bite: lack of contact between upper and lower posterior teeth in centric occlusion. It may be unilateral or bilateral.
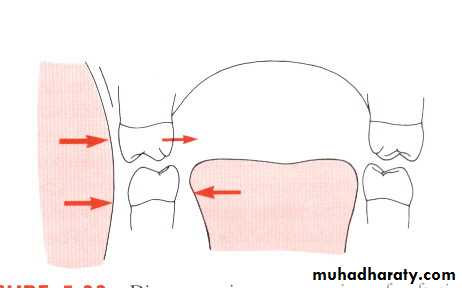
Posterior open bite are relatively rare compared to AOB and result mainly from mechanical interference with eruption either before or after the tooth emerges from the alveolar bone.
Posterior open bite
