Open bite malocclusion.
Deep bite malocclusion.
Deep bites are more prevalent than open bites and can be managed well with comprehensive orthodontic treatment.
Vertical orthodontic problems
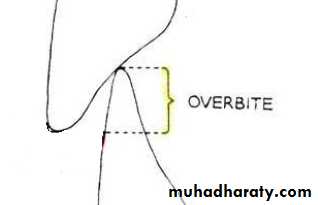
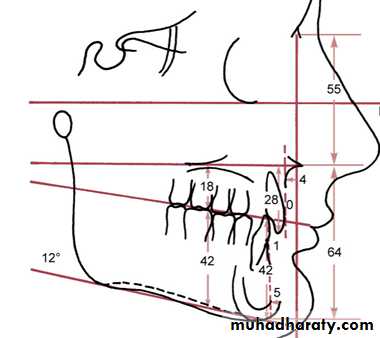
In normal vertical relation 1/4 to 1/3 of crown length of lower incisors should be overlapped by the upper incisors, and is governed by the degree of vertical development of the anterior dentoalveolar segments.
Deep bite: is increased vertical overlapment of the mandibular incisors by their maxillary antagonists when posterior teeth are in contact (increased overbite).
Deep pen bite malocclusion

Classification
DentalSkeletal
Combination of both
Dental deep bite: Result from lack of eruption of posterior teeth or overeruption of the anterior teeth, also it can occur due to premature loss of posterior teeth.
Skeletal deep bite: Associated with horizontal growth pattern with a tendency of upward and forward rotation of the mandible causing reduced lower facial height (short face)

Thorough clinical and radiographic evaluation is needed to decide whether the condition is dental or skeletal in origin or combination of both.
Diagnosis
Increased overbite,
Excessive curve of spee in lower arch.Absent or reverse curve of spee in upper arch.
Gingival inflammation resulting from trauma
Clinical features of dental deep bite
Clinical features of skeletal deep bite
Extraoral featuresShort lower facial height
1Everted and prominent lips
2
flat mandibular plane angle
3
Often associated with some degree of mandibular deficiency
4

Clinical features of skeletal deep bite
• Excessive overbite, Crowded incisors
1Often accompanied by Cl II division 2 malocclusion
2
Gingival inflammation resulting from trauma
3


Cephalometric features of skeletal deep bite (short face syndrome)
• Decreased mandibular plane angle.• Decreased basal plane angle.
• Decreased anterior facial height.
• Decreased posterior dentoalveolar height.
•
Treatment plan
Deep bite may result from:
Reduced lower face height (skeletal problem) which can be treated with growth modification in preadolescent children (mixed dentition).
Lack of eruption of posterior teeth or Overeruption of anterior teeth. Both are complex problems and can be managed well with comprehensive treatment during adolescence and are rarely treated during mixed dentition years.
Treatment
Treatment of skeletal deep bite (short face) in preadolescentsTreatment is directed toward increasing eruption of posterior teeth so that the mandible would rotate downward.

There are 2 method for growth modification in short face children:
• Functional appliance usually with mandibular advancement (deep bite bionator).It is constructed to allow eruption of posterior teeth and block eruptions of incisors.

• Cervical headgear
As its directed below center of resistance of maxilla it will exert extrusive force on upper molars.Headgear can be used with anterior biteplate so that both upper and lower molars can erupt.
The appliance is worn for 10-12 h/day with a forceof 12ounces/side.

Deep bite correction is performed routinely during first stage of comprehensive orthodontic treatment by leveling out the arches.
There are 2 ways to correct increased overbite:
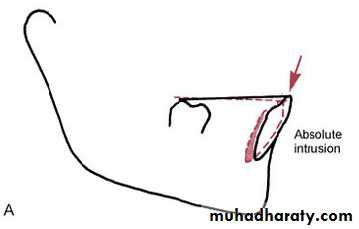
• Intrusion of the upper and lower incisors, moving their root apices close to the nose and lower border of the mandible.(absolute intrusion)
Correction of deep bite with comprehensive treatment
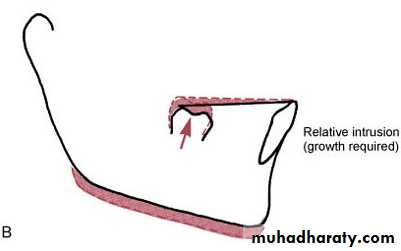
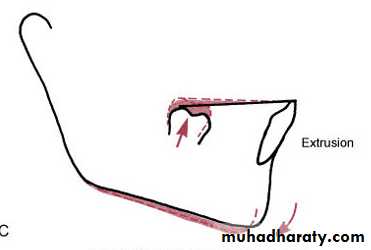
• Extrusion of posterior teeth:
If performed in growing patients (adolescents and young adults up to 18 years), the growth of ramus will compensate for increase in molar height and MP angle is maintained.(relative intrusion)In the absence of growth elongation of posterior teeth would rotate the mandible downward and backward and increases the MP angle.
Correction of deep bite with comprehensive treatment
As a general rule intrusion is preferred in non growing patients while extrusion of posterior teeth (relative intrusion) is quite acceptable for adolescents and young adults.
However 2 factors should be considered in choosing the approach for deep bite correction :
• The vertical relationship between maxillary lip and maxillary incisors.
• Anterior facial height.
Correction of deep bite with comprehensive treatment
If the display of upper incisors on smile is appropriate, deep bite is corrected by intrusion of lower incisors. If display is excessive, intrusion of upper incisors is indicated.
If face height is short, elongating posterior teeth slightly (usually lower molars) would be acceptable, if face height is long intrusion of incisors would be needed

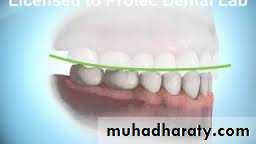
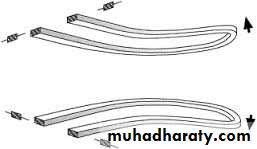
Leveling by extrusion
Can be accomplished with continuous archwires, simply by placing an exaggerated curve of spee in the upper archwire and a reverse curve of spee in mandibular archwire.
16 mil wire with reverse or accentuated curve followed by 18 mil wire are quite effective to complete leveling of arches.
Mechanics used for leveling


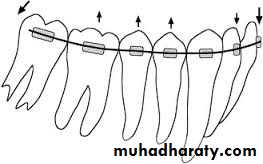
Leveling by intrusion
It requires a different mechanical arrangement that allows application of light continuous force toward tooth apex (10 gm/tooth) of incisors without causing extrusion of posterior teeth.
Mechanics used for leveling
This can be accomplished in 2 ways:• With continuous archwires that bypass the premolar teeth and sometimes the canine too.
• With segmented archwires (so that there is no connection along the arch between the anterior and posterior segments) along with an auxiliary depressing arch.
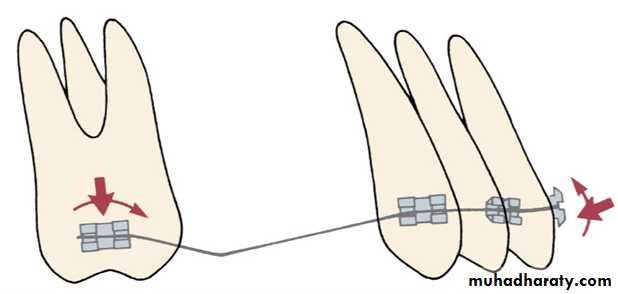
Leveling by intrusion
Bypass archesIn this approach intrusion is achieved using small diameter rectangular arch wire that by pass premolars and with an anchor bend mesial to the molars.
Usually transpalatal arch is used for additional anchorage and to control molar extrusion.
Leveling by intrusion
Bypass arches
Usually transpalatal arch is used for additional anchorage and to control molar extrusion.Leveling by intrusion


Segmented arches
This approach allows attachments on all the teeth so it provides better control of anchorage.A full dimensional rectangular archwire is placed in bracket slots of posterior teeth. A resilient wire is placed in anterior segment.
Leveling by intrusion

Segmented arches
An auxiliary intrusion arch (18x25) is placed in the auxiliary tube on the first molar and is adjusted so that it lies gingival to incisor teeth when passive.
The wire is tied beneath the brackets of incisors to apply light intrusive force (10 gm/tooth)
Leveling by intrusion




Auxiliary intrusion arch
In adults with extreme anterior deep bite who need considerable amount of anterior intrusion, using skeletal anchorage with temporary anchorage devices is more effective.
In this case intrusion is achieved using auxiliary wire anchored bilaterally to alveolar bone screws and tied beneath incisor brackets anteriorly.


Retention after deep bite correction
The key to retention is to control the vertical position of incisors after fixed orthodontic treatment is completed.Retention after deep bite correction
This is accomplished using a removable upper retainer made so that the lower incisors will contact the baseplate of the retainer that is to build a potential biteplate into the retainer.While the upper incisors contact the facial surface of the lower retainer

Retention after deep bite correction
Because vertical growth continues into late teens, wearing of the appliance is continued as a nighttime retainer until completion of growth.