
True bacteria – Cocci- Gram positive cocci
Streptococci
Most of Strep. species are commensal resident of mouth, throat, so
several may act as opportunistic pathogens, also few spp. like
Strep. pyogenes and Strep. agalactiae act as primary pathogen.
Classification of Streptoccoci
Strep. are classified by 2 major methods:
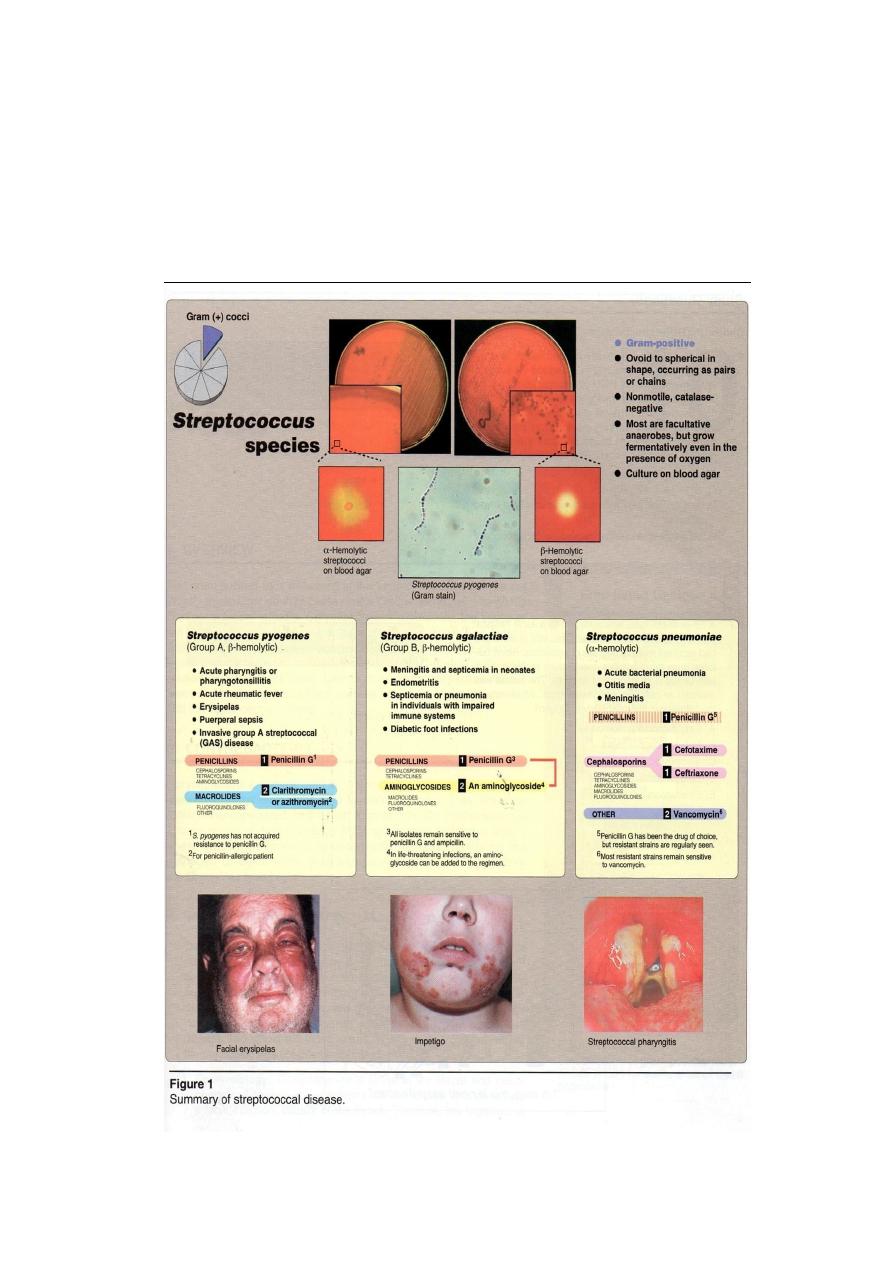
1- Classification by hemolytic activity:
The initial classification of the Strep. depends on the type of
hemolysin produced on blood agar (under anaerobic conditions about
(5-10 % Co
2
): (Figure 1).
a- Strains that produce soluble hemolysin(Streptolysin O or S)
colonies that produce streptolysin causing complete clearness around
the colony in blood agar are called β-hemolytic Streptococci e.g
Strep. pyogenes, Strep. agalactiae.
b- Strains that produce insoluble hemolysin which causes partial lysis
called α-hemolytic Streptococci e.g Strep. pneumonia, Strep.viridans.
c- Starins that are non-hemolytic, give no change around the colonies
called γ-hemolytic streptococci e.g Strep. faecalis.
2- Serological classification (Lancefield classification).: (Figure 2)
Made by Lancefield, based on the presence of polysaccharide
antigen
called
"C-substance" or "C-carbohydrate" present in the cell wall which differ
from group to another .A,B,C,D which are implicated in human
infections, and E,F,H,G and K-U which are implicated in animal
infections.
Group A causes tonsillitis in human.
Group B causes mastitis which is transmitted from cows to human
through contaminated milk.
Group C causes strangles disease which transmitted to human from
horses.
Group D which are enterococci present as normal flora in intestine
of human.
All above are β- hemolytic Strep. and the clinical important groups
are types A and B.

Antigenic Structure of Streptococci:
Several antigentic substances are formed in the hemolytic Strep. cells:
1- Group-Specific cell wall antigen
This carbohydrate is contained in the cell wall of many
Streptococci and forms the basis of serologic grouping
(Lancefield A-U)which is determined by an amino sugar which
are:
Group A Rhamnose-N- acetylucosamine.
Group B Rhamnose-glucosamine polysaccharide.
Group C Rhamnose-N-acetylgatasamine.
Group D glycerol techoic acid containing D-alanine and glucose.
2- M-protein
This protein is associated with virulence of group A and occurs
in organisms producing mucoid colonies.This protein resists the
phagocytosis.
3- T- substance
This antigen has no relationship to virulence of Strep. and used
to differentiate between certain types of Strep. by agglutination
with specific antisera.
4- Nucleoproteins (P-substance)
That make up most of the Strep. cell body and a little of serologic
specificity.

Groups of Streptococci
A- β-hemolytic Streptococci
1) Group A Streptococcus pyogenes
is the human pathogen of primary importance, produce human
respiratory infection, such as Tonsillitis, bronchopneumoniae, scarlet
fever, erysipelas, cellulitis, glomerulonephritis and rheumatic fever.
Group A are usually bacitracin sensitive.
2) Group B Streptococcus agalactiae
are endogenous to the vaginal mucosa and been responsible for
puerperal fever, fatal neonatal meningitis and endocarditis.This group is
rarely bacitracin sensitive.
3) Group C and G
Causes erysipelas, puerperal fever, throat infection, sinusitis,
bacteremia or endocarditis, occur sometimes in pharynx and produce β-
hemolysin on sheep blood agar e.g. Strep. equisimilis and Strep.equi
4) Group D
Includes Enterococci, e.g. Strep. faecalis and non-Enterococci,e.g.,
Strep. bovis produces α and γ hemolysin which may causes UTI or
endocarditis.
5) Group E, F, H and K, U
Occur primarily in animals others can infect humans.
B- Non β-hemolytic Streptococci
These usually produce α-hemolysis or no hemolysis on blood agar.
This group includes:
1- Strep. pneumoniae (pneumococci)
(1) bile soluble , (2) inhibited by optochin disks , (3) Quellung
reaction positive (capsule swelling test) (4) can cause pneumomia and
other infection processes.
2- Strep. viridans
(1) not bile soluble , (2) not inhibited by optochinn disks , (3) Quellung
reaction negative, (4) they are normal flora in upper respiratory tract in
human and may cause endocarditis.

C- Peptostreptococci
They are members of the normal flora of the gut and female genital
tract, grow under aerobic or microaerophilic condition and produce
variable hemolysin.
Group A Hemolytic Streptococci :
The most clinically important species of this group is Strep.
pyogenes it can invade in the skin or mucous membrane and cause
infection .
Structural Features :
These are involved in the identification of Group A Streptococci:
Capsule:
Hyaluronic acid resemble to that found in human connective tissue,
it is not recognized as foreign by the body, so it is non-immunogenic.
Cell wall:
Contains no. of clinically important components:
a. Fimbriae: contain the major Strep. pyogenes virulence factor,
the M protein .
b. Group A specific C-carbohydrate: composed of rhamnose &
N-acetylglucoseamine (all gp A Strep. contain this antigen).
c. Protein F (Fibronectin binding protein): which mediated
attachment to fibronectin in pharyngeal epithelium .
Extracellular products play a role in the pathogenesis (Figure3)
More than 20 extracellular products (exotoxins) that are antigenic are
produced by group A Strep. including :-
1- Streptokinase (Fibrinolysin)
produced by many strains of group A hemolytic Strep. Transforms
the plasminogen of human plasma into plasmin, which is an active
proteolytic enzyme that digests fibrin and other proteins.
2- Streptodornase (DNase)
This E. depolymerizes DNA in exduates and purulent exudates,
their viscosity to deoxyribonucleoprotein, both streptokinase and DNase
help to liquefy exudates and facilitate removal of pus and necrotic tissue,
both enzymes are used for diagnosis test of Strep. in general.
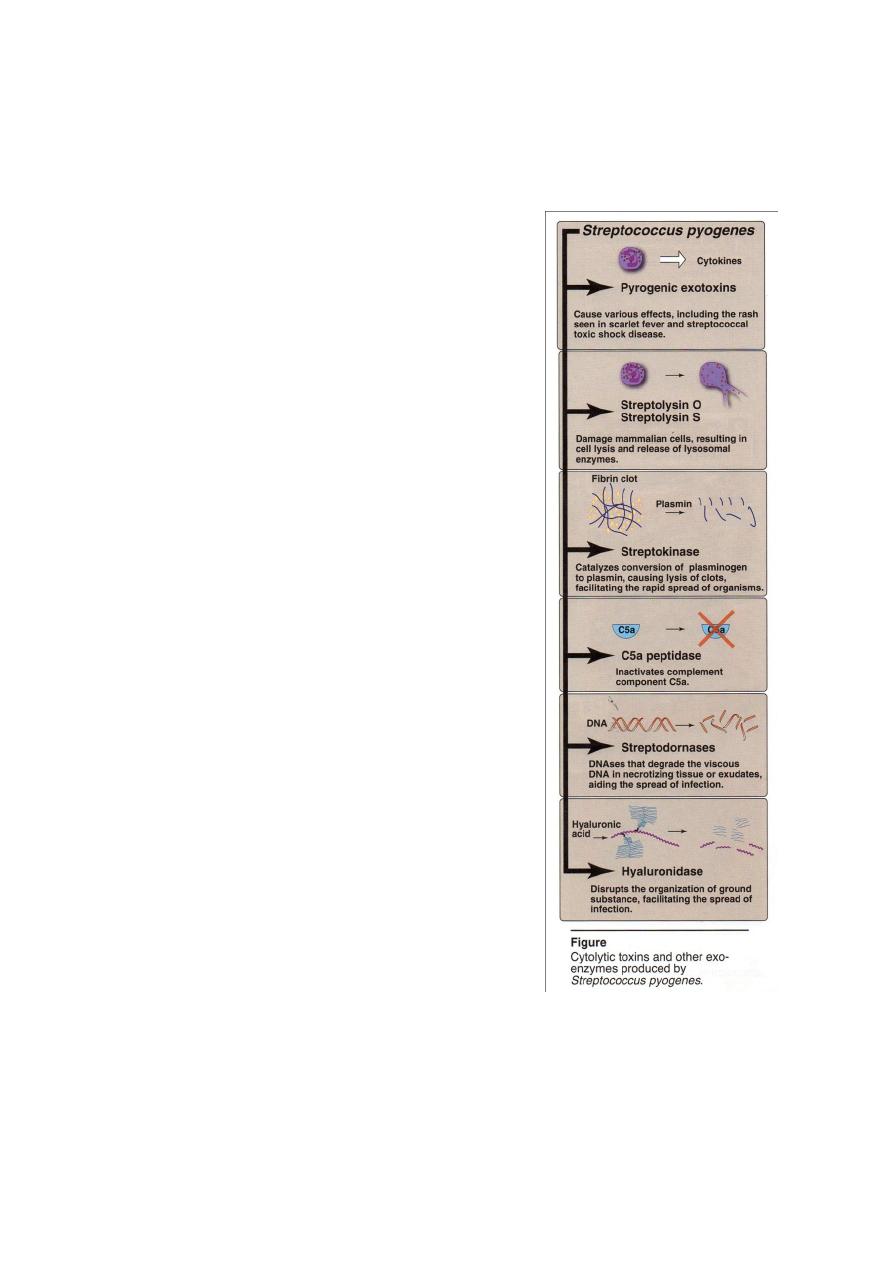
3-Hyaluronidase
E. splits hyaluronic acid, an important component of connective
tissue. This hyaluronidase aids in spreading infecting microorganisms
(Spreading factor), it's antigenic.
4- Diphosphopyridine Nucleotidase
E is kill leukocytes. Proteinase and
amylase are produced by some strains.
5-Erythrogenic Toxin (Pyrogenic exotoxins)
It causes the rash in scarlet fever and
elaborated
by
lysogenic
Strep.
(Strep.
pyogenes) also called Dick toxin, and detected
by dick test (anti toxin).
6- Hemolysin
In
β-hemolytic group A Strep.
pyogenes
elaborates
two
hemolysins
(streptolysins):
a- Streptolysin O= labile and inactivated in
O
2
, this antigen is responsible for the produce
of Ab called (antistreptolysin O) (ASO) in
human following infection and act as a titers
for diagnosis if the serum titers of 160-200
units suggests recent infection.
b- Streptolysin S=stable in O
2
and causes
hemolytic zones around Strep. colonies on
blood agar this is not antigenic.
Clinical Findings
A- Disease due to invasion : by β-hemolytic
group
(A)
such
as
Strep. pyogenes : Pathogenicity is determined
by (1) portal of entry of the Strep., (2)
diffusion of spreading of Strep. to different parts of the body (3) extend
along lymphatic pathways → to the blood stream.
3

1- Erysipelas
If the portal of entry is the skin, erysipelas results with massive
brawny edema, and rapidly advancing margin of infection.
2- Puerperal fever
If the Strep. enters the uterus after delivery, puerperal fever
develops which is essentially a septicemia originating in the infected
wound.
3- Sepsis/ bacteremia
Infection of traumatic or surgical wounds with Strep. results in
bacteremia/ sepsis, which can be fatal rapidly.
B- Diseases due to local infection: by
-hemolytic group (A)
1- Streptococcal sore throat
Patients have intensive nasopharyngitis, tonsillitis and intense redness
and edema of the mucous membrane, with purulent exudates, and usually
a high fever.If the infecting Streptococci produce erythrogenic toxin
scarlet fever rash will be produced.
2- Streptococcal pyoderma
Local infection of superficial layers of skin, in children, called
“impetigo”.
C- Infection of endocarditis
1- Acute endocarditis
Rapid destruction of the valves leads to fatal cardiac failure.
2- Subacute endocarditis
Due to members of the normal flora of respiratory or intestinal tract
that have accidently reached the blood.
D- Other infection
Various
Strep.,
such
as
Enterococci
can
cause
UTI,
Peptostreptococci which occurs in the female genital tract, the gut and
intestine causes suppurative lesion in the genital tract of the female.

E- Post streptococcal disease
1- Acute glomerulonephritis
occurs after 3 weeks of the infection by Strep. group A and about
23% of children with skin infection with type 49 strain develops nephritis
or hematuria.
2- Rheumatic fever
This is the most serious of Strep. group A infections, because it
results in damage to heart muscles and valves, appears after 1-4 weeks of
infection, causes a complex infection all parts of the heart (endocardium
– mycocardium – pericardium).
Diagnostic laboratory tests
Specimens : depend upon the nature of Strep. infection, as swab, pus,
blood is obtained for culture. Serum is obtained for Ab determination.
Microscopic examination
: G+ spherical or ovoid bacteria that are
arranged in chains of varying length, nonsporing , nonmotile
,noncapsulated .
Macroscopic examination
: facultative anaerobes require enriched
media as blood agar for growth. On blood agar incubated aerobically
and anaerobically to show the type of hemolysis and colonial
appearance. catalase negative
Strep. group A sensitive for bacitracin .
Serologic test : by using ELISA, or Agglutination test, also
antistreptolysin
O
(anti
ASO)
in
respiratory
infections,
antihyaluronidase in skin infection. Antistreptokinase, anti-M type –
specific Abs and others of these. The anti ASO titer is most widely
used.
Treatment
All
-hemolytic group A Strep. are still susceptible to penicillin G
and most are sensitive to erythromycin.
In endocarditis, which caused by enterococci, a combination of
penicillin G and aminoglycoside is used as treatment.
Penicillin prophylacticin is given to person with rheumatic fever, to
prevent recurrence of the disease (monthly for several years).
Amoxicillin is used for dental procedure.

Streptococcus agalactiae (group B,
-hemolytic)
Found as normal flora in vagina in 5-25% of woman and in
urethral mucous membranes of male carriers as well as in the G.I.T.
Their colonies on blood agar are larger and less hemolysis than Group
A
-hemolytic Strepococci (Strep. pyogenes).
It can transfer from infected mothers to infants at birth and may cause
(1) meningitis and septicemia in neonates with high mortality rate,
(2) endocarditis endometritis,
(3) septicemia or pneumonia in impaired immune systems individuals .
(4) diabetic foot infections.
Sensitive to penicillin G and ampicilline. Strep. group B resistant
for bacitracin .
Streptococcus pneumonia
Antigenic Structures
It posses a number of Ags:
A- The capsular polysaccharides (SSS)
Specific
Soluble
Substance
in
capsulated
form.
Capsular
polysaccharides are used to determine the type specificity of organisms
and virulence.Typing can carried out by:
1- Agglutination of cocci with type – specific antisera (Ag + Ab
reaction).
2- Precipitation of capsular polysaccharide with specific serum.
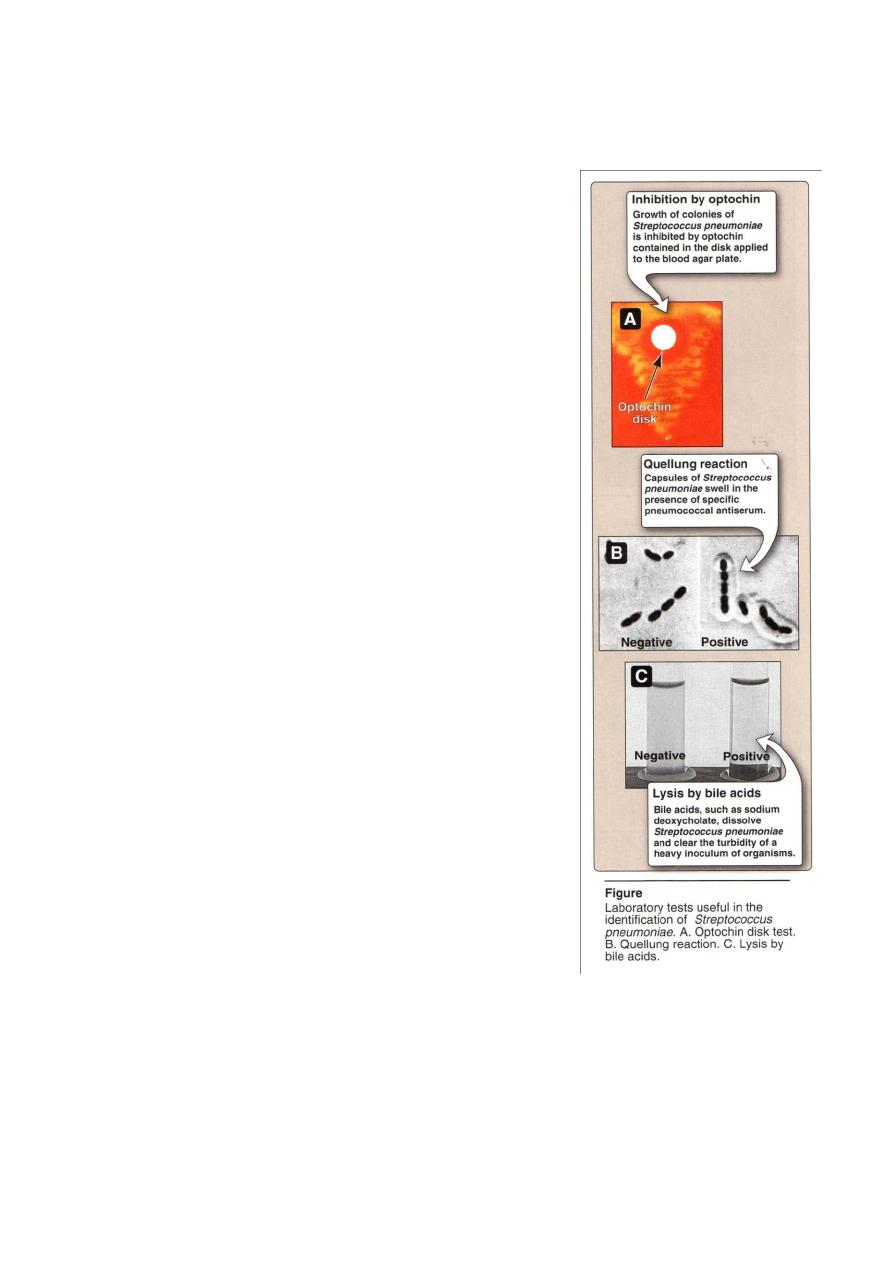
3- Capsular swelling reaction (Quellung reaction). Suspension of
pneumococci is mixed with specific anti-polysaccharide serum of
the same type or the polyvalent antiserum on slide, the capsule
swells.This reaction useful for rapid identification and for typing of
the microorganism (Figure 4).
B- M- Protein
It's characteristic for each type of Strep. pneumonia
C- Group – Specific Carbohydrate
This is common in all pneumococci , which it can be precipitated by
(c-reactive proten) in the serum of patients.
.
Toxin and Virulence Factors
1- Pneumolysin O
an oxygen sensitive toxin, cytolytic for cells.
2- Neuraminidase
E degrades surface structure of host tissues.
3- Capsular polysaccharide
It’s SSS which protects the microorganism from
phagocytosis and has association with virulence.
4- C- substance
The cell wall of pneumococci contain teichoic acid
(C-sub) that react with a certain antiserum protein,
C- reactive protein (CRP) and causes activation of
some nonspecific host immune response.
5- Leucocidin
Kills leukocytes W.B.C.
Pathogenesis
It’s a normal flora of nasopharynx and
oropharynx in 15% of children and 5% of adults.
They produce disease through their ability
to multiply in the tissues and the virulence of
pneumococci is a function of it’s capsule which
prevents ingestion by phagocytes.
The normal respiratory mucosa posses
natural resistance to the pneuomococci, many
factors lower this resistance and predispose to
infection, like:
1- Respiratory viral infection, bronchial obstruction, respiratory tract
injury, alcohol or drug intoxication .
2- Organism passes from person to another via respiratory secretions and
aerosols.
4

Clinical Findings
The onset of pneumococcal pneumonia is usually sudden with
fever, chills and sharp pleural pain, with blood or rusty sputum. In the
early disease, when the fever is high, bacteremia is present in about 10-
20% of cases, causes severe complication as meningitis, which is the
most serious infection common in children, endocarditis, septic arthritis.
1- Acute bacterial pneumonia
A leading causes of death in the aged and those whose resistance is
impaired. This disease caused mostly by Strep. pneumonia. Pneumonia is
preceded by an upper or middle respiratory viral infection, which
predisposes to Strep. pneumonia infection of pulmonary parenchyma, by
the mechanisms of:
1) increased volume and viscosity of secretions that are more difficult to
clear,
2) Secondary, inhibition of the action of bronchial cilia by viral infection.
2- Otitis media
Which is the most common bacterial infection of children, is most
caused by pneumococcus,followed by Haemophils influenza and
Moraxella catarrhalis
The traditional treatment of it with a
-lactam antibiotics (with or
without a penicillinase – inhibitor) has been threatened by the spread of
penicillin – resistant pneumococci.
3- Bacteremia/ sepsis
In the absence of a focus of infection is commonly caused by
pneumococcus, especially in splenectomized individuals.
4- Meningitis
H. influenzae was leading cause of bacterial meningitis in U.S.
After a vaccine was developed against this organism, Strep. pneumonia
became the most common cause, which is high mortality rate even when
treated.

Laboratory identification (Table 1) :
Specimens → nasopharyngeal swab, pus, sputum or spinal fluid.
Microscopic examination
: show many polymorphonuclear
neutrophiles and many RBC. (1) G + , (2) lancet shaped (3) diplococci,
(4) nonmotile, (5) nonsporing, (6) capsulated.
Macroscopic examination : need enriched media with blood or
serum for growth, produce
-hemolysin on blood agar growth is
enhanced by 5-10% CO
2
. On solid media → form a small round colonies
dome-shaped at first, few hours later it undergoes some autolysis in the
center of the colony and become flat while the edges are arised.
Biochemical tests →
1- Optochin sensitivity
2- Lysis the cell by bile acids
3- Capsular swelling (the Quellung reaction, see figure 4) is observed
when sputum treated by type– specific antisera as immunological
test.
4- Inuline fermentation to different from Sterp. viridans
Animal pathogenicity → mice are most susceptible to
pneumococcal infection and used for diagnosis, animal will die in 18-
48h.
Treatment and Prevention
Pneumococci are sensitive to sulfonamides and penicillin.
Amoxicillin, cephalosporins, erythromycin, cortimoxazole ,vancomycin
and penicillin G. Recently some drug resistance has appeared, e.g.
tetracycline, erythromycin and lincomycin.
Prevention
by
pneumococcal polysaccharides vaccine ppv,
immunizes against 23 serotype of Sterp. pneumoniae and is indicated for
the protection of high risk individuals older than 2 years, for 85-90% of
infections, including prominent penicillin-resistant strains.
Pneumococcal conjugate vaccine pcv7, is effective in infants (6
weeks – 5 years of age). Its made up of 7 pneumococci Ags conjugated to
CRM 197 (a mutant nontoxic diphtheria toxin). This vaccine protect
invasive pneumococcal disease, in older children and adults, effects on
pneumococci transmission (indirect effects on herd immunity) than
through it’s direct effect of protecting vaccinated children.
Streptococcus viridans
Include species : Sterp. nitis , Sterp. mutans and Sterp. salivarins
There growth is not inhibited by optochin disk , not soluble in bile
salt and not ferment Inuline (see table 1).
It’s a members of the normal flora of the upper respiratory tract, it
cause endocarditis, some like Strep. mutans produce large polysaccharide
which contribute to the genus of dental caries.
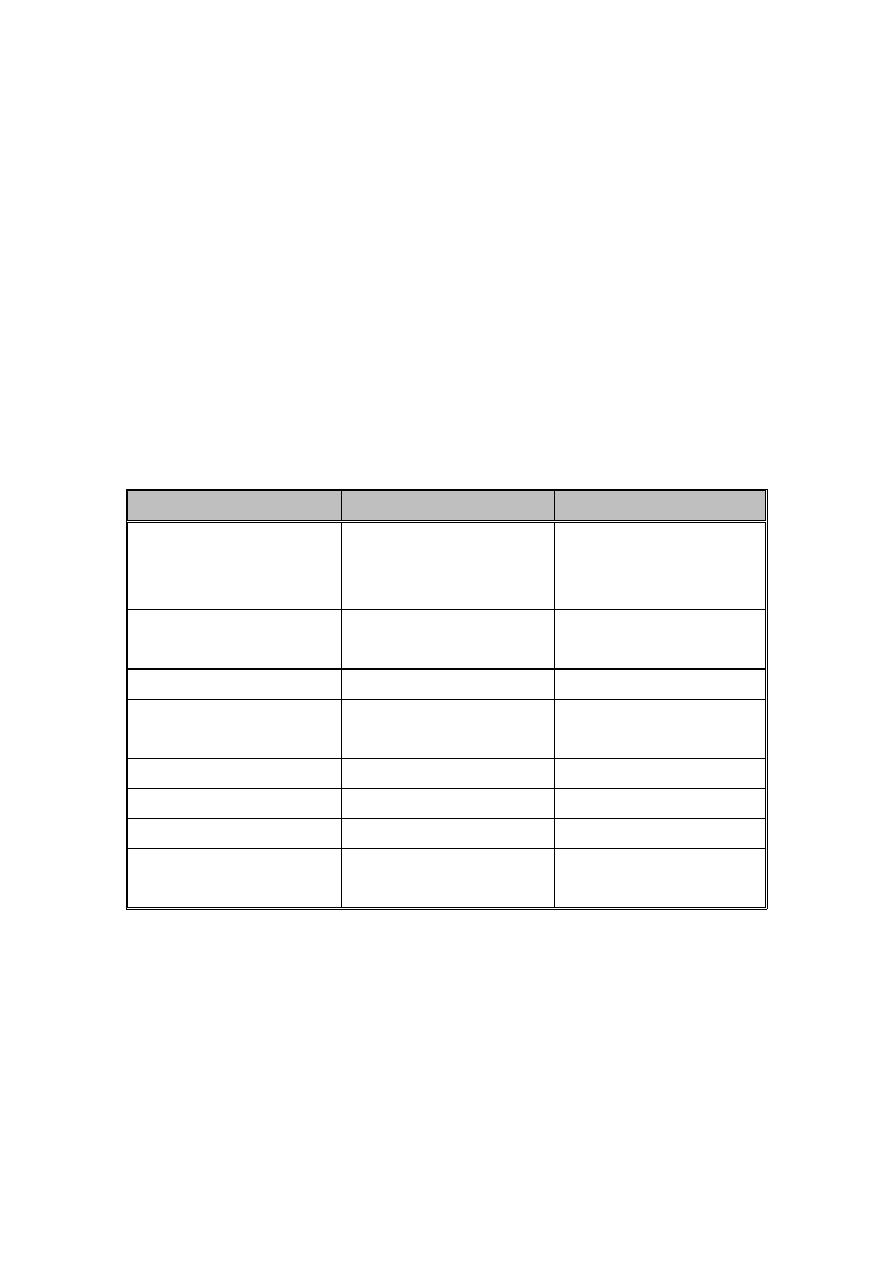
Table 1: Differentiation between Streptococcus pneumococcus and
Streptococcus viridans
Strepto. pneumonia
Strepto viridans
Microscopical
morphology
Capsulated
flame-
shaped diplococci
Non capsulated oval or
round
arranged
in
chains
Culture colonies
Initially dome-shaped
later flated colonies
Dome – shaped
Quelling test
+
-
Growth in liquid media Uniform turbidity
Granular turbidity and
powdery deposits
Bile solubility
+
-
Inuline fermentation
+
-
Optochin sensitivity
Sensitive
Resistant
Intraperitoneal
inoculation in mice
Cause fatal infection
non pathogenic