Chronic Pharyngitis
Dr. Abdullah R. AlkhalilCollege Of Medicine
University Of Duhok
Chronic Pharyngitis
Common conditionMale to Female Ratio is 1:1 “ Women seek medical attention more than Men”
One of the most troublesome symptom due to difficulty in diagnosis and in treatment
Wide variety of causes
Idiopathic!!!
Chronic Pharyngitis
Nonspecificchronic simple pharyngitis
Specific
syphilis
TB
Chronic Pharyngitis
Symptoms include
Cervical pain
Choking sensation
Chronic cough
Constant throat clearing
Dysphagia “ Improved with eating!”
Food sticking in throat
Chronic Pharyngitis
Globus sensationHalitosis
Hoarseness
Unilateral otalgia
Pharyngeal tightness
Sore throat
Chronic Pharyngitis
Etiology:Chronic Pharyngitis
BE AWARE OF THESE SYMPTOMS:Dysphagia
Weight loss
Hoarseness
Haematemesis
Haemoptysis
Unilateral earache with normal eardrum
Neck swelling
Neurology
Chronic Pharyngitis
SIGNS:Non specific
Granular pharyngitis
Halitosis
Tonsillar enlargment
tonsilolith
Chronic Pharyngitis

Chronic Pharyngitis
Treatment:
Difficult
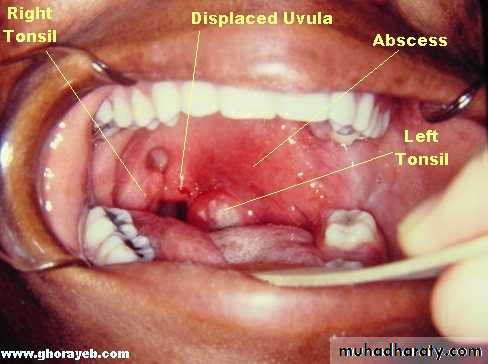
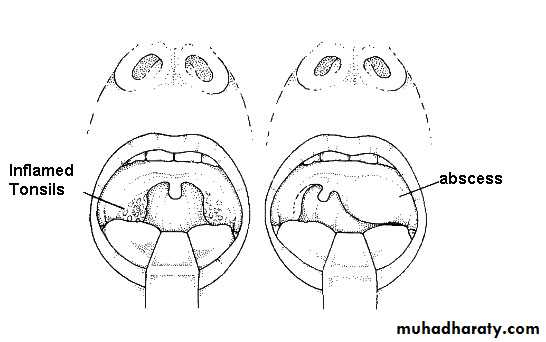
Treat underlying causesPeritonsillar abscess (Quinsy)
Etiology:The infection spreads to the peritonsillar area (peritonsillitis). This region comprises loose connective tissue susceptible to formation of abscess.
Both aerobic and anaerobic bacteria can be causative. Commonly involved species include streptococci, staphylococci and hemophilus.
Epidemiology:
- occur as complication of acute tonsillitis.
- more in adults (15-30) than in children.
Peritonsillar abscess (Quinsy)
Clinical featuresFever, dehydration.
severe dysphagia
Edema of soft palate
Uvular deviation (downward and medially)
Involvement of motor branch of CN V increased salivation and trismus (Persistent contraction of the masseter muscles due to failure of central inhibition)
Hot potato voice
Unilateral referred otalgia
Peritonsillar abscess (Quinsy)
Peritonsillar abscess (Quinsy)
Peritonsillar abscess (Quinsy)
Complications:Airway obstruction
BacteremiaAspiration pneumonia secondary to rupture of abscess
Peritonsillar abscess (Quinsy)
Treatment:Preferably admitted to hospital and treated with analgesics and antibiotics.
In a patient with an early peritonsillar abscess which is really a peritonsillar cellulitis incision and drainage are not recommended.
Peritonsillar abscess (Quinsy)
Treatment:surgical incision and drainage of pus forming outside the capsule -- relieving the pain dramatically.
Under general anesthesia – in children and anxious pts.
Peritonsillar abscess (Quinsy)
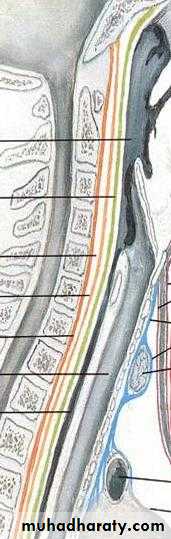
Retropharyngeal Abscess
Retropharyngeal Space:Entire length of neck.
Anterior border - pharynx and esophagus (buccopharyngeal fascia)Posterior border - alar layer of deep fascia
Superior border - skull base
Inferior border – superior mediastinum
Combines with buccopharyngeal fascia at level of T1-T2
Midline raphe connects superior constrictor to the deep layer of deep cervical fascia.
Contains retropharyngeal nodes.Retropharyngeal Abscess

Retropharyngeal Abscess
Most common symptomsSore throat
Odynophagia
Neck swelling
Neck Pain
Retropharyngeal Abscess
PediatricFever
Decreased oral intake
Odynophagia
Malaise
Torticollis
Neck pain
Otalgia
Trismus
Neck swelling
Vocal quality change
Worsening of snoring, sleep apnea
Retropharyngeal Abscess
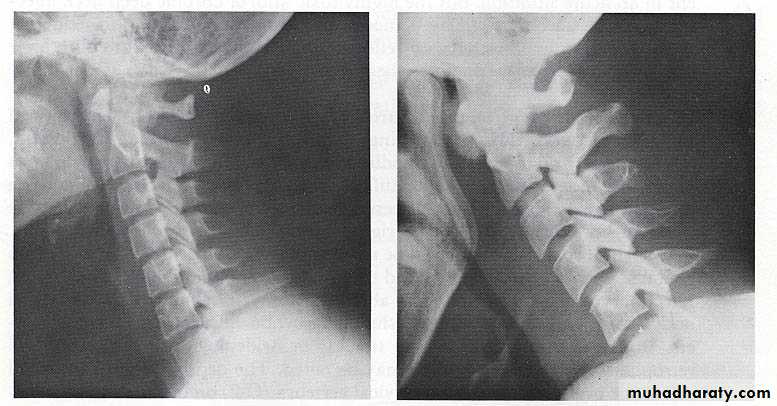
Imaging:
Lateral neck plain film
Screening examNo benefit in pts with DNI based on strong clinical suspicion.
Normal:
7mm at C-2
14mm at C-6 for kids
22mm at C-6 for adults
Technique dependent
Extension
Inspiration
Sensitivity 83%, compared to CT 100%
Retropharyngeal Abscess
Retropharyngeal Abscess

Retropharyngeal Abscess
Treatment:Initial therapy
Cover Gram positive cocci and anaerobesIf pt is diabetic, should consider covering gram negatives empirically.
Clindamycin, 2nd generation cephalosporin.
gentamicin and flagyl - developing nations.
IV abx alone (based on retro and parapharyngeal infections)
Patient stability and nature of lesion.Cellulitis/phlegmon by CT.
Abscesses in clinically stable patient.
If no clinical improvement in 24 - 48 hours proceed to surgical intervention.
Retropharyngeal Abscess
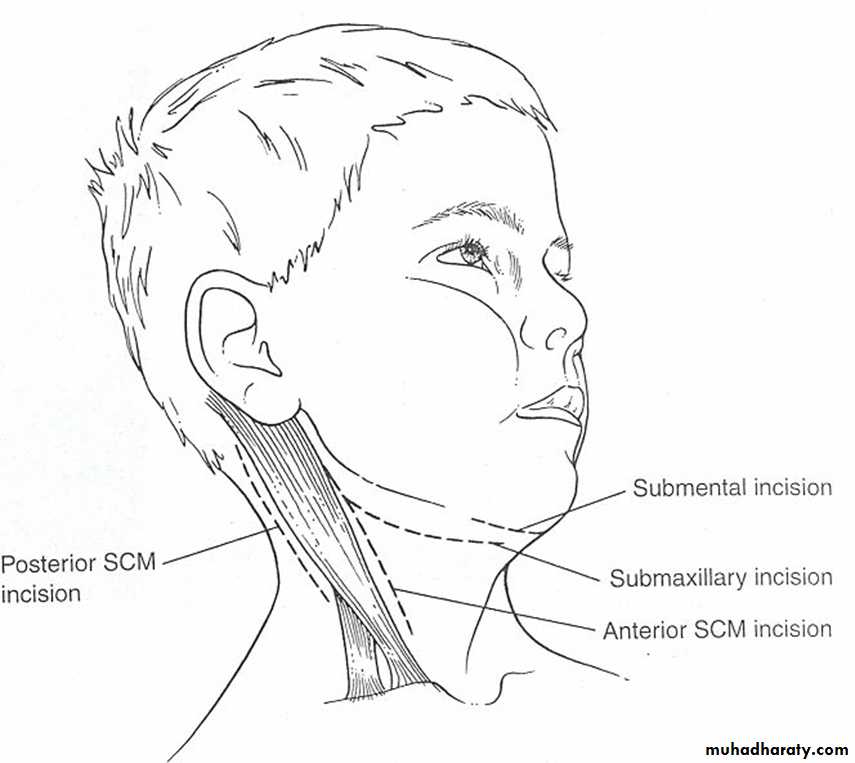
Treatment:External drainage
Landmarks
Tip of greater horn of hyoid
Cricoid cartilage
Styloid process
SCM
Transoral drainage
Parapharyngeal, retropharyngeal abscesses
Great vessels lateral to abscess
Tonsillectomy for exposure
Needle aspiration
Retropharyngeal Abscess
Complications:Airway obstruction
Trach 10 – 20%Ludwig’s angina - 75%
Mediastinitis – 2.7%
UGI bleeding
Sepsis
Pneumonia
IJV thrombosis
Skin defect
Vocal cord palsy
Pleural effusion
Hemorrhage
20 - 80% mortality
Multiple space involvement