
Lecture 1 Treatment of Heart Failure
Aim and intended learning outcome:
The student should be able to
Understand the pathophysiology and compensatory mechanisms.
of heart failure
Describe the strategies and the drugs used in the treatment of heart failure, their
classification and rationale .

CHF usually occurs when the cardiac output is inadequate to meet the
metabolic needs of the body.
In CHF, the ventricular dysfunction may be primarily systolic (i.e.
inadequate force generation to eject blood normally as in ischemic heart disease)
or it is may be diastolic (inadequate relaxation to permit normal filling as a result
of hypertrophy or stiffness of the myocardium).
CHF due to sytolic dysfunction usually respond to inotropic drug e.g.
digoxin while CHF due to diastolic dysfunction does not respond optimaly to these
drugs.
Rarely high output failure occurs whereby needs of the body are so great inspite
of the C.O. this form of failure poorly responds to +ve inotropic drugs.
Treatment is by correcting the underlying cause

the primary symptoms of all types of CHF include: tachycardia,
decreased exrecise tolerance, SOB, peripheral and pulmonary edema,
cardiomegaly on x ray
.
.
The decreased exercise tolerance and easy fatigability are due to decreased co.
while the other
manifestations are due to compensatory mechanisms.
Physiology Of Cardiac Muscle Contraction:
Contraction of the cardiac muscle is due to movement of actin
and myosin in cardiac sarcomers during systole resulting from the
interaction of Ca
+
with actin troponin tropomyosin system.
This activator Ca
+
comes from 2 sources:
•From outside the cell, enter during plateau phase of action potential
through voltage gated Ca
+
channels.
•Release of Ca
+
from the sarcoplasmic reticulum which depend on
the amount stored in the SR and the amount of trigger Ca
+
that
enter the cell.
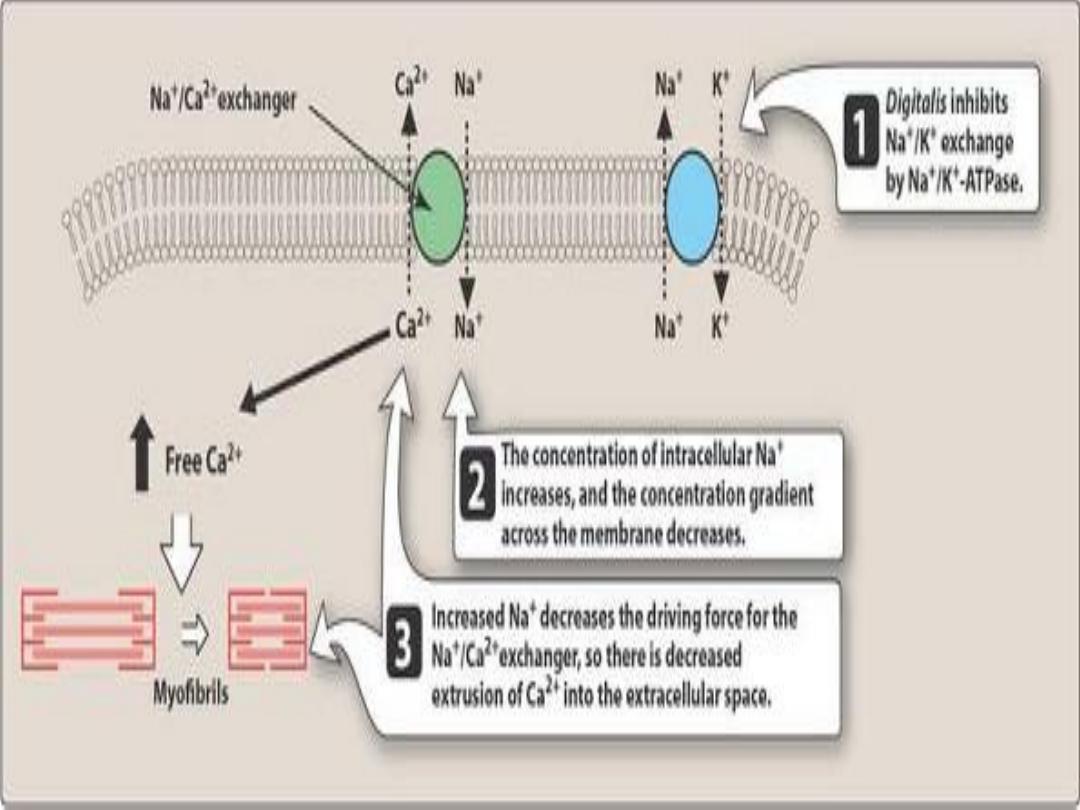
Therefore the contraction of cardiac muscle is directly related to the
concentration of the free cystolic Ca
++
. Removal of Ca
+
: Na-Ca exchanger: which exchange Ca with Na
thus any change in the intracellular concentration of Na will affect
the cellular levels of Ca
+
.
Uptake by SR, more than 99% of Ca
+
is stored in the SR and
mitochondria
Pathophysiology of Cardiac
performance
:
It's a function of 4 primary factors:
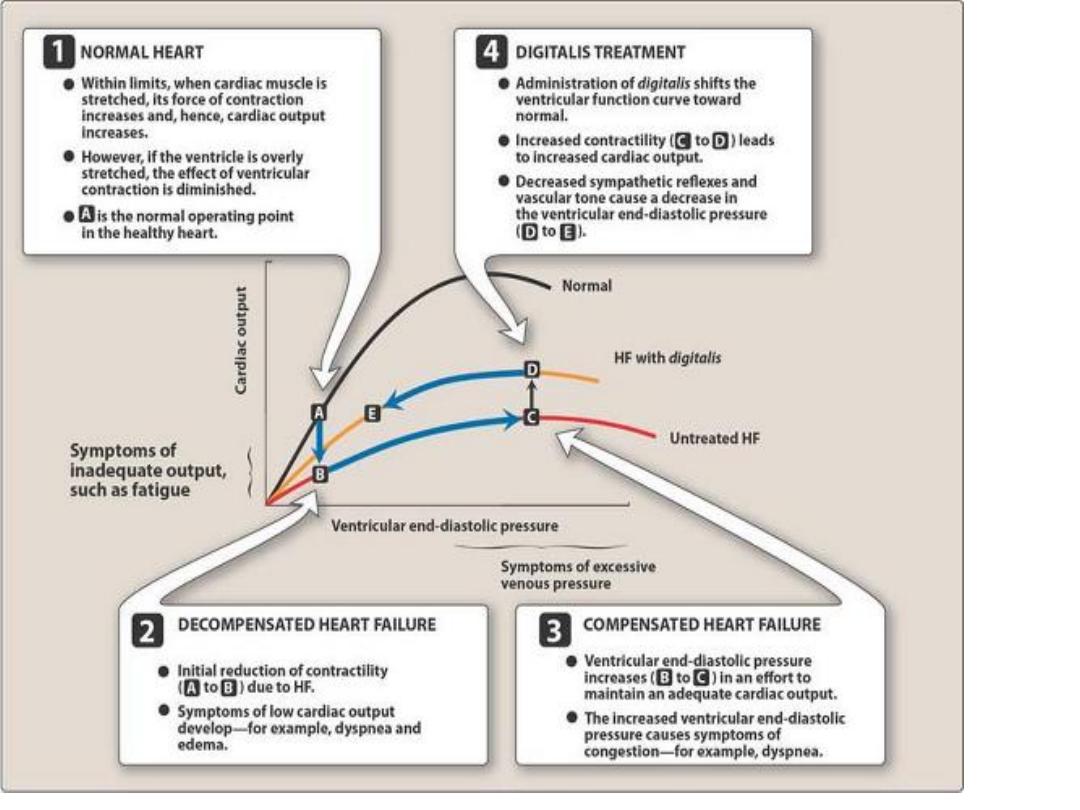
Preload: is the volume of the blood that fills the ventricles in diastole, when it is increased.
it causes overfilling of the heart which Increases the work load
Starling law: within limits, the ventricular performance is related to the degree of
myocardial stretching.
When left ventricular performance (e.g. stroke volume or C.O.) is plotted as a function of
L.V. filling pressure (preload), then the resulting curve is called L.V. function curve…
therefore when preload is increased leads to increase
in ventricular stretching and will enhance the ventricular function.
The limit is End Diastolic Pressure (EDP) of 15 mmHg when there is plateau of
performance ,

•
On the other hand marked stretching causes marked deterioration of
ventricular function and EDP of 20 mmHg or more results in pulmonary
congestion.
In HF, preload usually increases because of increeased blood volume and
venous tone.
•Reduction of preload is the goal of salt restriction and diuretic therapy.
Vasodilators also reduce preload by redistributing the blood into peripheral
veins away from the heart
Afterload: is the systemic vascular resistance against the heart must pump the
blood, this is frequently increased in HF which leads to decreased CO. This
sets the stage for the use of the drugs that reduce arterial tone in CHF.
Contractility: in patients with chronic low output failure, there is reduction
in the intrinsic contractility of myocardium resulting in reduction of pump
performance; here comes the role of +ve inotropic drugs.
Heart rate: which is the major determinant of C.O. (i.e., C.O. = S.V. x Ht.
rate). The heart rate as the S.V. , this is the 1
st
compensatory mechanism to
maintain the C.O.
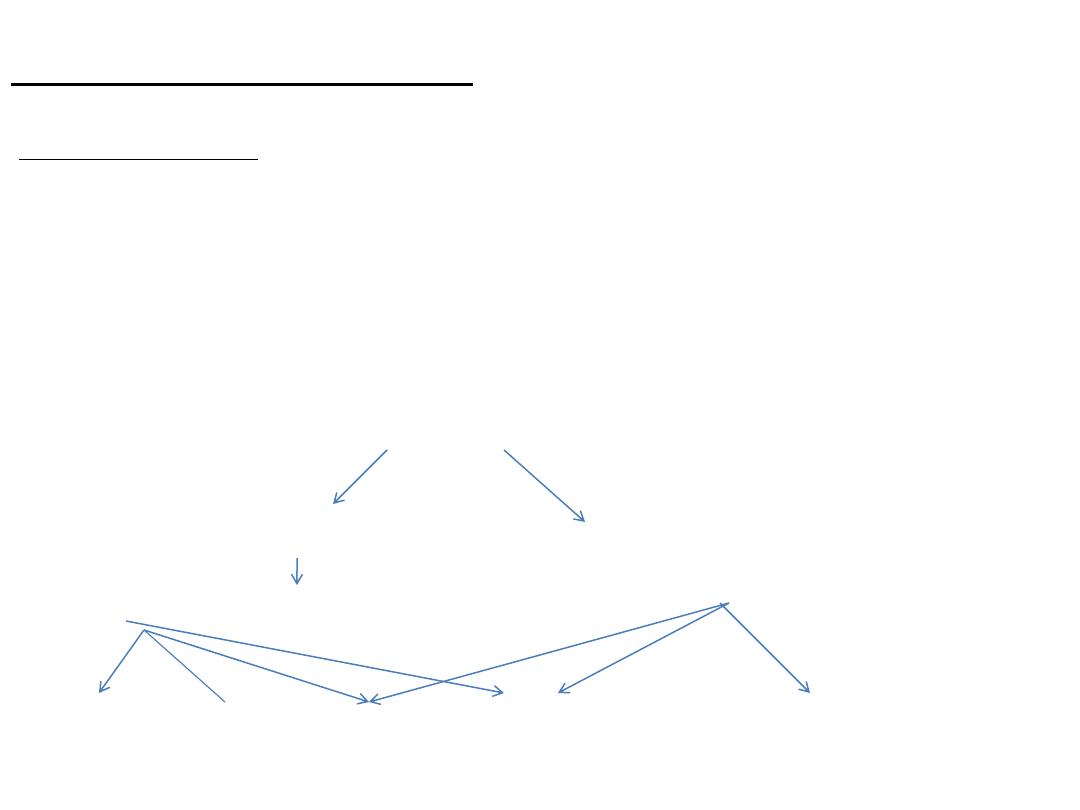
Compensatory Mechanisms in CHF:
•Neuro-hormonal reflex involves:
1.The sympathetic nervous system
2.The renin-angiotensin-aldosterone system
↓C.O.
↓Carotid sinus firing ↓Renal blood flow
↑Sympathetic discharge ↑renin ↑angiotensin II and ↑aldosterone
Force Rate Preload Afterload
Remodeling*
These compensatory mechanisms increase the work of the heart and can further
contribute to the decline in the cardiac function.
Myocardial hypertrophy: is the most important intrinsic compensatory
mechanism, the increase in myocardial mass helps to maintain cardiac
performance in the phase of pressure or volume overload. However, after initial
beneficial effect, hypertrophy can lead to ischemic changes, impairment of
diastolic filling and alteration in ventricular geometry (remodeling) due to
proliferation of abnormal myocardial cells and C.T. which die at the accelerated
rate leaving the remaining myocardial cells subject to even greater overload.
Drugs used to treat CHF
•Diuretics: loop diuretics and thiazides AND SPIRONOLACTONE.
•Vasodilators:
ACE inhibitors (arteries and veins) and angiotensin receptor blockers
Hydralazine Arteries
Minoxidil
Arteries
Isosorbide
mainly veins
Brain natriuretic peptide(BNP) Nesiritide
Endothelin antagonists Bosentan ,tezosentan
Cardiac inotropic agents
Cardiac glycosides (digoxin, digitoxin)
β-adrenergic agonist (dobutamine, dopamine)
Phospho diesterase inhibitors (amrinone, milrinone)
They increase cAMP by inhibiting phosphodiesterase iso enzyme III which in turn Ca
+
entry
during the A.P., they also have significant vasodilatory effect, they are used for acute heart
failure, their toxicity prevents long term use which includes B.M. toxicity, liver toxicity and
also cardiac arrhythmia
Beta-blockers: most patients with chronic stable heart failure respond favorably to
certain
β-blockers (carvedilol, metoprolol ,Bisoprolol) inspite of the fact that these drugs can
ppt. acute decompensation of cardiac function.
Newer agents
Ivabradine
acts by reducing the heart rate via specific inhibition of the funny channel
(I
f
) which is highly expressed in the
. I
f
is a mixed Na
+
–K
+
inward current that
initiates the spontaneous diastolic depolarization phase. It has no effect on contractility but
allowing more time for blood to flow to the myocardium due to reduction of the HR.
Sacubitril
is a neprilysin inhibitor.Neprilysin is responsible for the degradation of atrial and
brain naturetic peptides. Therefore the levels of these peptides are increased.it is usually used
in combination with valsartan.

Summary
Cardiac performance is a function of preload , afterload, contractility
and heart rate.
Compensatory mechanisms in CHF involve the sympathetic and the
angiotensin-renin system.
Drugs used in the treatment include
Diuretics
Vasodilators of arteries and/ or veins
Inotropic drugs
B-Blockers
