د.إكرام الحسو Parasitology Lec:1
9-3-2017Medically important Cestodes (Tapeworms) of human beings
Class Cestoidea include 2 orders:
Order Cyclophyllidea:which includeEchinococcus Spp. 3) T. solium
2) Taenia saginata 4) Hymenolepis nana
5) Hymenolepis Diminuta
6) Diphyllobothrium caninum
2. Order Pseudophyllidea : include Diphyllobothrium latum
Echinococcus Spp.Genus Echinococcus include three species:
E. granulosus
E. multilocularis
E. vogeli
E.granulosis
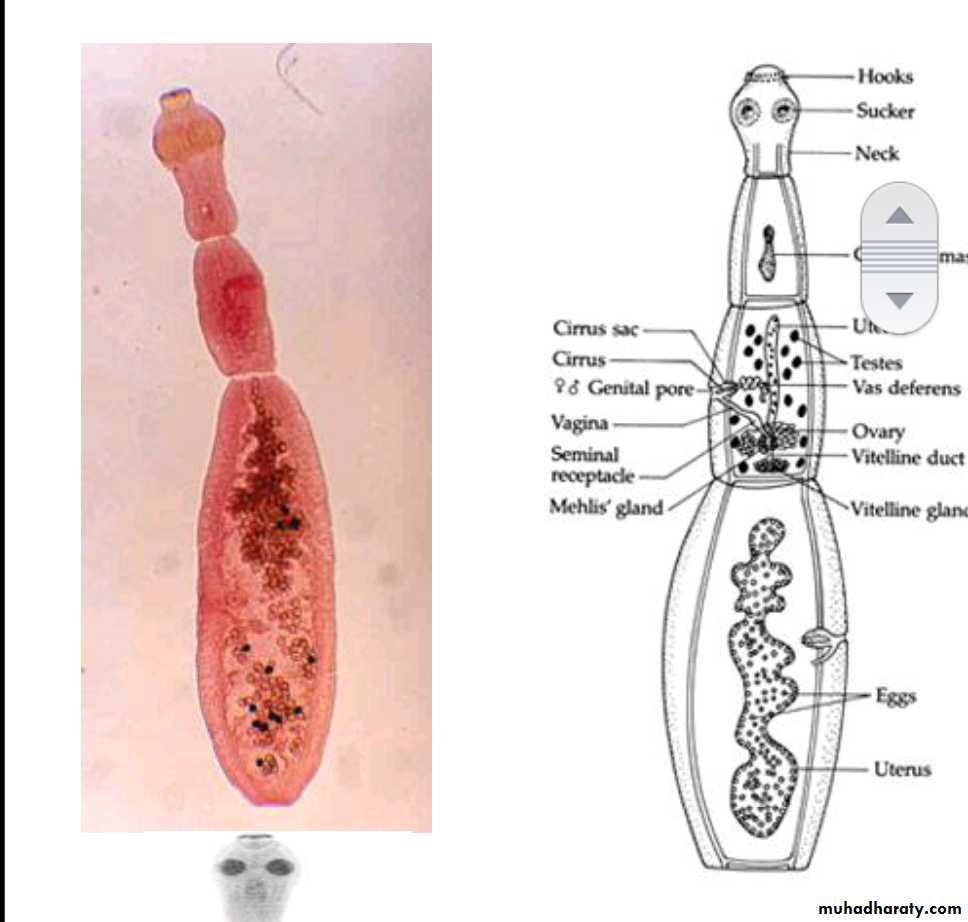
Morphology of adult worm
2-6 mm long.
The body consist of:
head (scolex) with 4 suckers and rostellum with two rows of hooks.
three segments (proglottids):Immature, mature and gravid.
The mature segment: contain fully developed male and female sexual organs.
The gravid segment: contain only uterus full with eggs.
Morphology of the egg (Taenia spp. Egg ).
Spherical, 35-45 um in diameter
Hexacanth Embryo centrally located
Radially staited shellInfective stage to human, sheep & cattle .
The same egg of Echinococcus Spp., Taenia saginata & T. solium
Life cycle
The adult E. granulosus inhabit the upper part of small intestine of the definitive (final) hosts, dogs or other canids ( cats, foxes and wolves).Gravid proglottids release eggs that are passed in the feces .
These eggs are infective stage to a suitable intermediate host (sheep, goat, cattle and man).
After ingestion, the eggs hatches in the small intestine and releases an oncospher (emberyo) that penetrates the intestinal wall and migrates through the circulatory system to various organs, especially the liver and lungs.
In these organs, the oncosphere develops into a hydatid cyst that enlarges gradually, producing protoscolicis inside the cyst.
The dogs ( definitive host )and other canids becomes infected by ingesting the hydatid cyst-containing organs of the infected intermediate host. After ingestion, the scolex evaginate, attach to the intestinal mucosa, and develop into adult stages in 30 to 80 days.
Hydatid disease (hydatidosis)
Is caused by the larval stages (hydatid cyst) of tapeworm called Echinococcus granulosus.Types of hydatid cysts : Unilocular, Osseous & Multilocular or alveolar.
Unilocular type:
It is the larval stage of E. granulosus composed of single cavity. The majority of human H. cysts are unilocular type. It may reach 15 cm or more in diameter after 10 to 20 Years.
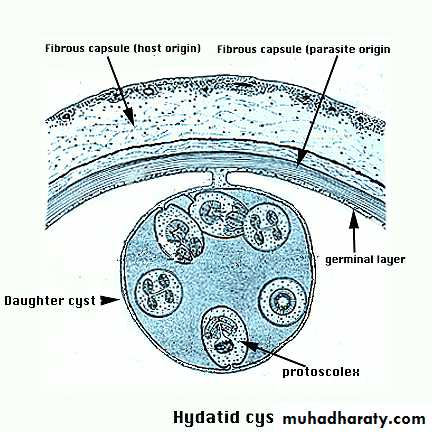
Morphology:
consist of three layers with central fluid contain protoscolices
The three layers :
1- Inner nucleated germinal layer .
2- non-nucleated laminated layer.
3- Outer (fibrous layer):This layer formed as a result of defense mechanism of the host against the parasite.
Inner germinal layer :thin, delicate, one cell layer and nucleated.
From inner germinal layer the following structures arise:
A- Brood Capsule: Develop from germinal layer and hold by short pedicle to the germinal layer. In the brood capsule multiple protoscolices develops.
Hydatid cyst with protoscolices and brood capsule is known as fertile hydatid cyst. Sometimes hydatid cyst will not contain protoscolices, so it is known as sterile or acephalocyst.
Fertile hydatid cyst is more dangerous because:
each protoscolex will develop to adult worm when ingested by definitive host
if fertile hydatid cyst rupture it will lead to dissemination of the disease.
B- Hydatid Fluid: The cavity of unilocular hydatid cyst is filled with hydatid fluid, which is highly antigenic, bacteriologically sterile and colorless.
C- Hydatid Sand: If the brood capsule detached from germinal layer, the brood capsule and protoscolices become free in hydatid fluid and they are called hydatid sand.
D- Endogenous Daughter Cyst: morphologically resemble mother cyst but it is smaller in size and free in hydatid fluid.

osseous H. cyst :
When the embryo of E. granulosus reaches bony tissues it will develop to osseous hydatid cyst.Occure in bony tissues.
The larva grows as a protoplasmic stream that erodes the cancellous tissues and lead to multiple bone fractures.
It is occur in the ends of long bones and pelvic arch.
Multilocular or Alveolar Hydatid Cyst:
It is the larval stage of E. multilocularis, it is composed of numerous small spaces or cavities, separated from each other by connective tissue. Each space filled with jelly-like matrix, mostly it is sterile but occasionally it may contain protoscolices. The germinal and laminated layers are poorly developed, it has no fibrous capsule.It is occurs usually in the liver and rarely in lung. Because of its fast growth, it is usually fatal.
Rupture of Hydatid Cyst:
Rupture of hydatid cyst may occur naturally, due to coughing, muscle strain or surgical procedures. Such patients may suffer from anaphylactic shock, eosinophilia and allergic reactions or even death.
The escape cyst fluid with protoscolices has the capacity of spreading to other sites and forming a new cyst (secondary hydatidosis).
Rupture of the cyst are most important than the mass effect of the cyst, except in the brain where the mass effect has severe consequences.
Epidemiology
Worldwide in its distribution .Rural infection more than urban aeas because it is a sheep raising areas .
Transmission
Ingestion of uncooked vegetables and fruits(eg: lettuce &parsley) & drinking water contaminated with eggs.
Handling soil or animal hair that containing eggs.
Clinical picture:
1. Disease called H. Cyst, Hydatid disease, Hydatosis.
2. The severity of the disease varies according to location of the cyst in tissues affected.
3. No symptoms until the cyst gets large or ruptures:Such patients may suffer from allergic reactions, eosinophilia and anaphylactic shock or even death.
4. Hepatic H.cyst
Liver affected in about 65 % of patients .Approximately 70% right lobe is affected.
Usually no symptoms until the cyst reach 10 cm in diameter : hepatomegaly, nausea, vomiting.
5. Pulmonary H.cyst
Lung affected in about 23% of patients .
Rupture of pulmonary H.cyst into bronchules results in :coughing, shortness of breath, secondary bacterial infection.
6. H. cyst of brain :Brain occasionally infected, produce mass effect.
Other organs, Bones, muscle, Kidney, heart and pancrease.
Diagnosis
Clinical manifestation: depend on the size and site of hydatid cyst. At the beginning the disease is asymptomatic. As the cyst continue to grow pressure effect usually results.
2. Imaging techniques:
X-ray picture: useful to detect the calcified cyst.
Ultrasound scan.
MRI & CT scan.
3. Serology tests : eg:
Indirect immunofluescence.
Enzyme-linked immunosorbent assay (ELISA).
Polymerase chain reaction (PCR).
Treatment
1. Surgical operation to remove the cyst is the only option for the treatment.
2. Mebendazol or albendazol
given to reduce the risk of secondary hydatidosis, it also given for 60 days on 200 mg dose duration to reduce the size of the cyst before the surgical interference.
Prevention &control
1. Avoiding close contact with dogs.2. Careful washing of the vegetable with running water.
3. Preventing home-slaughter of sheep will prevent dogs from consuming infected viscera.
Taenia saginata &Taenia solium
Taenia saginata Beef tapeworm
Taenia solium Pork tapewormDisease : Taeniasis.
Morphology of adult
1. They are flat , hermaphroditic worms , live in small intestine of man.2. Adult worms consist of a head , neck and segmented body (proglottids) may reach thousands.
3. The head (scolex) contain suckers (T. saginata), or suckers & hooks (T. solium).
4. Mature segment contain both male & female sexual organs.
5. Gravid segment contain only uterus full with eggs which usually passed with eggs out with feces as diagnostic stages.
6. The length of adult worms is usually 4-10m for T. saginata and 2 - 7 meter for T. solium.
7 . T. saginata usually have 1,000 to 2,000 segments,
while T. solium have an average of 1,000 segments.


Adult worm of Taenia saginata Adult worm of Taenia solium
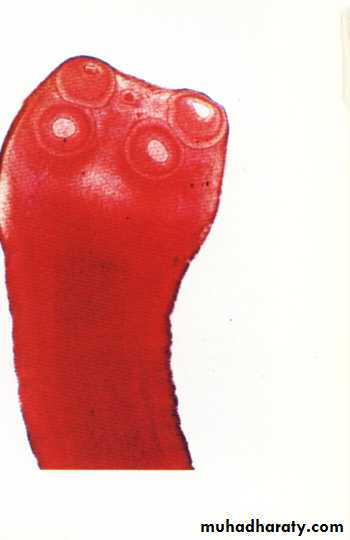
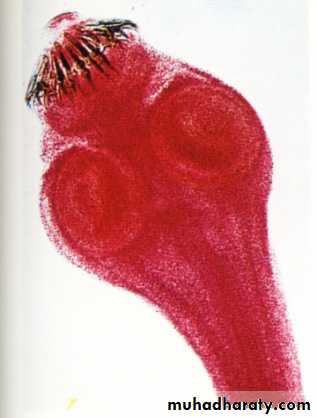
Scolex of T. saginata Scolex of T. Solium
Cysticercoids larva:It is bladder like cyst called bladder worm with invagenated or evagenated scolex.
They are infective stages to human and they are two type :
1. C. Bovis: scolex without hooks present in the muscles of cattles.
2. C.cellulosae : scolex with hookspresent in the muscles of pigs


Cysticercus bovis Cysticercus cellulosae
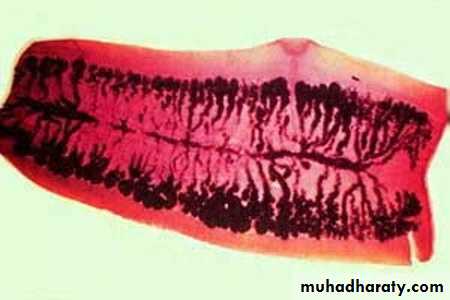
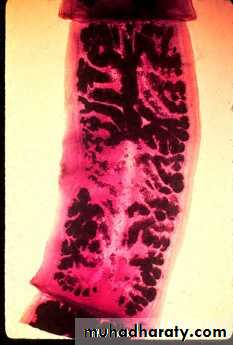
Gravid segment of T.Saginata Gravid segment of T.Solium
Gravid segment of T.Saginata:
gravid segments ;longer than wide consist of median uterus with 15-30 lateral uterine branches with unilateral genital pore .Gravid segment of T.Solium :
7 – 13 lateral uterine branches.
Life cycle of T. saginata and Taenia solium
1.Humans are the only definitive hosts for T.saginata and T. solium. Eggs or gravid proglottids are passed with feces .2.The intermediate host ( Cattle for T. saginata and pigs for T. solium).
3.The intermediate hosts become infected by ingesting vegetations contaminated with eggs or gravid proglottids.
4. In the animal's intestine, the oncospheres hatch, invade the intestinal wall, and migrate to the striated muscles, where they develop into cysticercus larva.
5. Humans become infected by ingesting raw or undercooked infected meat with cysticercus larva.
7. In the human intestine, the cysticercus develops over 2 months into an adult tapeworm, which can survive for years.
8. The adult tapeworms attach to the small intestine by their scolex .
Clinical Features:
1. mild abdominal symptoms.
2.because of the large size of the worm, it may be responsible for acute intestinal obstruction and anemia
3.Occsionally appendicitis can result from individual segment which may be lodged in the appendicial lumen
Taeniasis caused by T. solium : there is risk of development of cysticercosis.
Laboratory Diagnosis
Microscopic identification of scolex and segments in feces are diagnostic for taeniasis.
The gravid segments can differtiate between T.saginata and T. solium but the eggs are morphologically identical, and indistinguishable between taenia species.
Epidemiology
T. saginata: Cosmopolitan in beef eating countries, found in Europe, Asia & America.
T. solium: Cosmopolitan in pork eating countries, found in Latin America, Africa & central Asia.
Transmission
Human infection with Taenia spp occur by eating under cooked beef or pork containing cysticercoids larva.
Treatment
Niclosamide is the drug of choice .
In case of infection with T.Solium antivomiting drugs should be given one hour before treatment to prevent autoinfection with eggs, and 2 hours after treatment, saline purgative should be given to flush out of the worm .
Prevention
1. Treatment of infected patients .
2. Personal hygiene and enviromental sanitation are important .
3. Inspection of pork & beef meat for cysticercus larva .
4. Cooking very well the pork & beef before eating. 45-50 C for at least half hour is enough to kill the larvae.
5. Freezing at minus 2-10 C for 4 days enough to kill the larvae .
Cysticercosis
The most frequent and sever disease caused by accidental ingestion of eggs)feco-oral route) or by autoinfection may occurs in T. solium by regurgitation of gravid proglottid into the stomach & releas the eggs which pass to small intestine where embryo become free after hatching process , then penetrate the wall of the small intestine & carried via blood to different tissue of the body.The severity of cysticercosis depends on location , size and number of the larvae in the tissues , as well as the host immune response .
The most frequent locations are subcutaneous and intramuscular tissues , then eye and brain . they also may occur in the liver , lung , heart and abdominal cavity .
The most serious type of cysticercosis is neurocysticercosis which can lead to epilepsy , lesion in the brain , blindness and tumor like growths . and be can be fatal.
Diagnosis of human cysticercosis :
1-Biopsy: confirming the presence of hooks in the scolex of C. cellulosae by histopathological examination of biopsy materials
2-Serology(ELISA, IFAT).
3-MRI or CT scan of the brain.Treatment of cysticercosis
Usually asymptometicmanagement for patients with neurocysticercosis depend on the number and location of cysts, in this case surgical treatment indicated,
Praziquantil (5–10 mg/kg, single-administration)