
DISEASES OF EXTERNAL EAR
DISEASES OF THE PINNA
Congenital conditions1.Bat ear(prominent or lop ear)
This is an abnormally protruding ear. The concha is large with poorly developed antihelix. The deformity can be corrected surgically around the age of 6 years.
2. Preauricular appendages
They are skin-covered tags that appear in front of the tragus. They may contain small pieces of cartilage(accessory auricle)
3. Preauricular pit or sinus
This is commonly seen at the root of helix and is due to incomplete fusion of tubercles. It may get repeatedly infected causing purulent discharge. Abscess may also form. Treatment is surgical excision of the track if the sinus gets repeatedly infected
4. Anotia
It is complete absence of pinna, and usually forms part of the first arch syndrome
5. Macrotia
It is excessively large pinna.6. Microtia
It is a major developmental anomaly. Degree of microtia may vary. It is frequently associated with anomalies of external auditory canal, middle and internal ear. The condition may be unilateral or bilateral. Hearing loss is frequent.
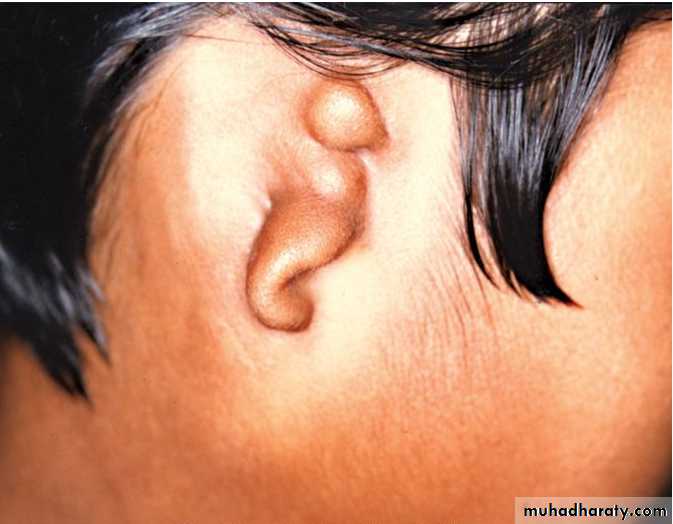
B. Trauma to the Auricle
1. Haematoma of the auricleIt is collection of blood between the auricular cartilage and its perichondrium. Often it is the result of blunt trauma seen in boxers, wrestlers and rugby players. Extravasated blood may clot and then organise, resulting in a typical deformity called Cauliflower ear . If haematoma gets infected, severe perichondritis may set in.
Treatment is aspiration of the early haematoma under strict aseptic precautions and a pressure dressing, of to prevent reaccumulation.. When aspiration fails, incision and drainage should be done and pressure applied by dental rolls tied with through and through sutures. All cases should receive prophylactic antibiotics
.

2. Lacerations
They are repaired as early as possible. The perichondrium is stitched with absorbable sutures.. Skin is closed with fine non-absorbable sutures. Broad spectrum antibiotics are given for one week.3. Avulsion of pinna
When pinna is still attached to the head by a small pedicle of skin, primary reattachment should be considered. Completely avulsed pinna can be reimplanted in selected cases by the microvascular techniques; in others, the skin of the avulsed segment of pinna is removed and the cartilage implanted under the postauricular skin for later reconstruction(Baudet technique)
4. Frostbite
Injury due to frostbite varies between erythema and oedema, bullae formation, and complete necrosis of the affected part.Treatment of a frost-bitten ear consists of: (a) rewarming with moist cotton pledgets at a temperature of 38-42°C, (b) analgesics (c) systemic antibiotics, (d) surgical debridement should wait several months as the true demarcation between the dead and living tissues appears quite late.
5. Keloid of auricle
It may follow trauma or piercing of the ear for ornaments. Usual sites are the lobule or helix. Surgical excision of the keloid usually results in recurrence. Some prefer local injection of steroid after excision(other treatments: 5 FU, Interferon-γ, LASER, cautery or cryosurgery,)
C. Inflammatory Disorders
1. PerichondritisIt results from infection secondary to lacerations, haematoma or surgical incisions. It can also result from extension of infection from diffuse otitis externa or a furuncle of the meatus. Pseudomonas and mixed flora are the common pathogens.
Initial symptoms are red, hot and painful pinna. Later abscess may form between the cartilage and perichondrium with necrosis of cartilage. Treatment in early stages consists of systemic antibiotics and local application of aluminium acetate compresses. When abscess has formed, it must be drained promptly and culture and sensitivity of the pus obtained. Incision is made in the natural fold and devitalised cartilage removed. Some prefer to place a catheter in the abscess and administer a continuous drip of antibiotics(e.g :gentamicin).
2. Relapsing polychondritis
It is a rare autoimmune disorder involving cartilage of the ear. Other cartilages may also be involved. The entire auricle except its lobule becomes inflamed and tender. External ear canal becomes stenotic. Treatment consists of high doses of systemic steroids(dapsone.& colchicine may be used also)3. Chondrodermatitis nodularis chronica helicis (Winkler's disease)
Small painful nodules appear near the free border of helix in men about the age of 50 years. Nodules are tender and the patient is unable to sleep on the affected side. Treatment is wedge excision of the nodule with its skin and cartilage.
D. Tumours
II. DISEASES OF EXTERNAL AUDITORY CANALA. Congenital Disorders
1. Atresia of external canalCongenital atresia of the meatus may occur alone or in association with microtia, due to failure of canalisation of the ectodermal core that fills the dorsal part of the first branchial cleft. The outer meatus is obliterated with fibrous tissue or bone. It may be associated with abnormalities of the middle ear, internal ear and other structures.
2. Collaural fistula
This is an abnormality of the first branchial cleft. The fistula has two openings; one, situated in the neck just below and behind the angle of mandible, and the other in the external canal or the middle ear. The track of the fistula traverses through the parotid in close relation to the facial nerveB. Trauma to Ear Canal
Minor lacerations of canal skin result from Q-tip injury (scratching the ear with hair pins, needles or match stick) or unskilled instrumentation by the physician. They usually heal without sequelae.
Major lacerations result from gunshot wounds, automobile accidents or fights. The condyle of mandible may force through the anterior canal wall. These cases require careful treatment. Stenosis of the ear canal is a common complication
C. Inflammations of Ear Canal
Otitis externa may be divided, on aetiological basis, into:(i) Infective group

(ii) Reactive group
Eczematous otitis externa
Seborrhoeic otitis externaNeurodermatitis
1. Furuncle (localised acute otitis externa)
A furuncle is a staphylococcal infection of the hair follicle. A furuncle is seen only in the cartilaginous part of meatus. Usually single, the furuncles may be multiple.Patient usually presents with severe pain and tenderness. Movements of the pinna are painful. Jaw movements, as in chewing, also cause pain in the ear. A furuncle of posterior meatal wall causes oedema over the mastoid with obliteration of the retroauricular groove. Periauricular lymph nodes (anterior, posterior and inferior) may also be enlarged and tender.
Treatment in early cases, without abscess formation, consists of systemic antibiotics(e.g flucloxacillin), analgesics and local heat. An ear pack of 10% ichthammol in glycerine provides splintage and reduces pain. If abscess has formed, incision and drainage should be done.
In case of recurrent furunculosis, diabetes should be excluded, and attention paid to the patient's nasal vestibules which may harbour staphylococci and the infection transferred by patient's fingers. Staphylococcal infections of the skin as a possible source should also be excluded and suitably treated.
2. Diffuse otitis externa
It is diffuse inflammation of meatal skin which may spread to involve the pinna and epidermal layer of tympanic membrane.Disease is commonly seen in hot and humid climate and in swimmers. Excessive sweating changes the pH of meatal skin from that of acid to alkaline which favours growth of pathogens.
Common organisms responsible for otitis externa are Pseud. aeruginosa , Staph. aureus, Proteus and Esch. coli but more often the infection is mixed.
Some cases of otitis externa are secondary to infection of the middle ear, or allergic sensitisation to the topical ear drops used for chronic suppurative otitis media.
Clinical features
Acute phase is characterised by hot burning sensation in the ear, followed by pain which is aggravated by movements of jaw. Ear starts oozing thin serous discharge which later becomes thick and purulent. Meatal lining becomes inflamed and swollen. Collection of debris and discharge accompanied with meatal swelling gives rise to conductive hearing loss. In severe cases, regional lymph nodes become enlarged and tender with cellulitis of the surrounding tissues.Chronic phase is characterised by irritation and strong desire to itch. This is responsible for acute exacerbations and reinfection. Discharge is scanty and may dry up to form crusts. Meatal skin which is thick and swollen may also show scaling and fissuring. Rarely, the skin becomes hypertrophic leading to meatal stenosis (chronic stenotic otitis externa).
Treatment Acute phase is treated as follows:
(a) Ear toilet: It is the most important single factor in the treatment of diffuse otitis externa. Ear toilet can be done by dry mopping, suction clearance or irrigating the canal with warm, sterile normal saline.(b) Medicated wicks: Wick is changed daily for 2-3 days when it can be substituted by antibiotic/steroid ear drops. Local steroid drops help to relieve oedema and erythema, and prevent itching.
(c) Antibiotics: Broad spectrum systemic antibiotics are used when there is cellulitis and acute tender lymphadenitis.
(d)Analgesics:
Chronic phase. Treatment aims at (a) reduction of meatal swelling so that ear toilet can be effectively done, and (b) alleviation of itching so that scratching is stopped and further recurrences controlled.
A gauze wick soaked in 10% ichthammol in glycerine and inserted into the canal helps to reduce swelling. This is followed by ear toilet with particular attention to antero-inferior meatal recess. Itching can be controlled by topical application of antibiotic steroid cream.
When the meatal skin is thickened to the point of obstruction and resists all forms of medical treatment, i.e. chronic stenotic otitis externa, it is surgically excised, bony meatus is widened with a drill and lined by split-skin graft.
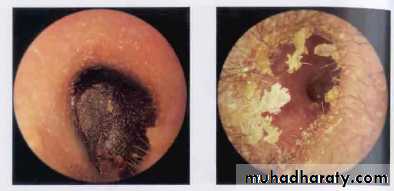
3. Otomycosis
Otomycosis is a fungal infection of the ear canal that often occurs due to Aspergillus niger, A. fumigatus or Candida albicans. It is seen in hot and humid climate of tropical and subtropical countries. Secondary fungal growth is also seen in patients using topical antibiotics for treatment of otitis externa or middle ear suppuration.The clinical features of otomycosis include: intense itching, discomfort or pain in the ear, watery discharge with a musty odour, and ear blockage. The fungal mass may appear white, brown or black and has been likened to a wet piece of filter paper(wet newspaper). Meatal skin appears sodden, red and oedematous.
Treatment
(a) Thorough ear toilet to remove all discharge and epithelial debris which are conducive to the growth of fungus. It can be done by syringing, suction or mopping.(b) Specific antifungal agents can be applied. Nystatin is effective against Candida. Other broad spectrum antifungal agents include clotrimazole. 2% salicylic acid in alcohol is also effective. Antifungal treatment should be continued for a week even after apparent cure to avoid recurrences.
(c) Ear must be kept dry.
(d) Bacterial infections are often associated with otomycosis, and treatment with an antibiotic/steroid preparation helps to reduce inflammation and oedema and thus permitting better penetration of antifungal agents.
4. Otitis externa haemorrhagica(Bullous myringitis)
It is characterised by formation of haemorrhagic bullae on the tympanic membrane and deep meatus. It is probably viral in origin and may be seen in influenza epidemics(Mycoplasma pneumoniae?). The condition causes severe pain in the ear and blood-stained discharge when the bullae rupture. Hearing impairment(conductive or sensorineural) is common. Treatment with analgesics is directed to give relief from pain. Antibiotics are given for secondary infection of the ear canal, or middle ear if the bulla has ruptured into the middle ear.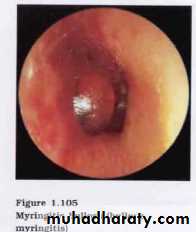
5. Herpes zoster oticus
It is characterised by formation of vesicles on the tympanic membrane, meatal skin, concha and postauricular groove. The seventh and eighth cranial nerves may be involved.


6. Malignant (necrotising) otitis externa
It is an inflammatory condition caused by pseudomonas aeruginosa infection usually in the elderly diabetics, or in those on immunosuppressive drugs. Its early manifestations resemble diffuse otitis externa but there is excruciating pain and appearance of granulations in the meatus. Facial paralysis is common. Infection may spread to the skull base and jugular foramen causing multiple cranial nerve palsies. Anteriorly, infection spreads to temporomandibular fossa, posteriorly to the mastoid and medially into the middle ear and petrous bone. MRI & CT scans are useful, to know the extent of disease.Treatment consists of high doses of i.v. antibiotics directed against pseudomonas (tobramycin, ciprofloxacin, ticarcillin or third generation cephalosporins). Antibiotics are given for 6-8 weeks or longer. Diabetes should be controlled. Surgery has a limited role.
7. Eczematous otitis externa
It is the result of hypersensitivity to infective organisms or topical ear drops such as neomycin. It is marked by intense irritation, vesicle formation, oozing and crusting in the canal. Treatment is withdrawal of topical antibiotic causing sensitivity, and application of steroid cream.8. Seborrhoeic otitis externa
It is associated with seborrhoeic dermatitis of the scalp. Itching is the main complaint. Greasy yellow scales are seen in the external canal, over the lobule and postauricular sulcus. Treatment consists of ear toilet, application of a cream containing salicylic acid and sulphur, and attention to the scalp for seborrhoea.
9. Neurodermatitis
It is caused by compulsive scratching due to psychological factors. Patient's main complaint is intense itching. Otitis externa of bacterial type may follow infection of raw area left by scratching. Treatment is psychotherapy and management of any secondary infection. Ear pack and bandage to the ear are helpful to prevent compulsive scratching.10. Primary cholesteatoma of external auditory canal
Squamous epithelium of the external canal invades its bone. It may be post-traumatic or postsurgical. Clinical features include purulent otorrhoea and pain; tympanic membrane being normal. Granulations associated with sequestrated bone need histological examination to differentiate it from carcinoma, necrotizing otitis externa and a benign sequestrum.Treatment consists of removal of necrotic bone and cholesteatoma, and lining the defect with fascia
D. Tumours
E. Miscellaneous Conditions1. Impacted wax or cerumen
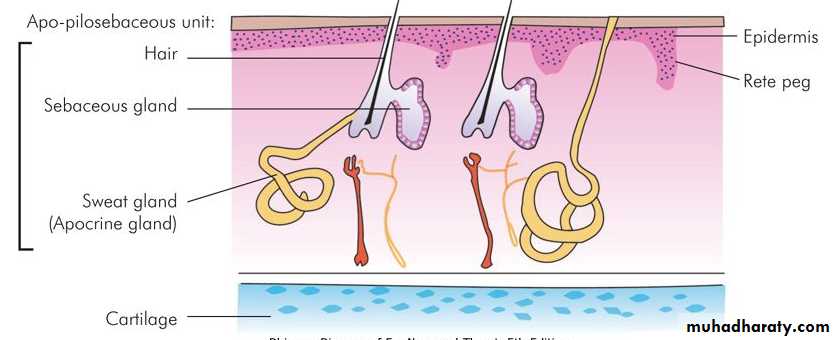
Wax is composed of secretion of sebaceous glands, ceruminous glands(modified sweat glands), hair, desquamated epithelial debris, keratin and dirt.Wax has a protective function as it lubricates the ear canal and entraps any foreign material that enters the canal. Normally, only a small amount of wax is secreted, which dries up and is later expelled from the meatus by movements of the jaw. The activity of ceruminous glands varies; excessive wax may be secreted and deposited as a plug in the meatus. Certain other factors like narrow and tortuous ear canal, stiff hair or obstructive lesion of the canal, e.g. exostosis, may favour retention of wax. It may dry up and form a hard impacted mass.
Patient usually presents with impairment of hearing or sense of blocked ear. Tinnitus and giddiness may result from impaction of wax against the tympanic membrane. Reflex cough due to stimulation of auricular branch of vagus may sometimes occur. Onset of these symptoms may be sudden when water enters the ear canal during bathing or swimming and wax swells up
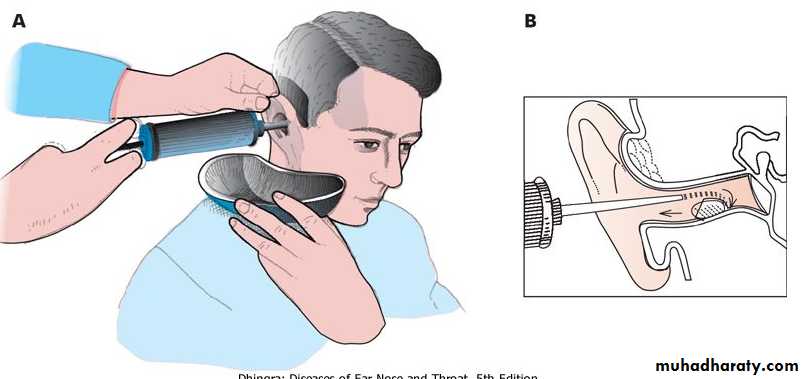
Treatment of wax consists in its removal by syringing or instrumental manipulation(Jobson-Horne probe & suction). Hard impacted mass may sometimes require prior softening with wax solvents.
Five percent soda bicarb in equal parts of glycerine and water, hydrogen peroxide, liquid paraffin or olive oil may also achieve the same result. Commercial drops containing ceruminolytic agents like paradichlorobenzene 2% can also be used and above methods tried again. A burning candle was used in the past also!
2. Foreign bodies of ear
(a) Non-living. Children may insert a variety of foreign bodies in the ear; the common ones often seen are: a piece of paper or sponge, grain seeds (rice, wheat, maize), slate pencil, piece of chalk or metallic ball bearings. An adult may present with a broken end of match stick used for scratching the ear or an overlooked cotton swab. Vegetable foreign bodies tend to swell up with time and get tightly impacted in the ear canal or may even suppurate.Soft and irregular foreign bodies like a piece of paper, swab or a piece of sponge can be removed with fine crocodile forceps or suctioning.
Most of the seed grains and smooth objects can be removed with syringing. Smooth round and hard objects like steel ball bearing should not be grasped with forceps as they tend to move inwards and may injure the tympanic membrane. In all impacted foreign bodies or in those where earlier attempts at extraction have been made specially in children or uncooperative patients , it is preferable to use general anaesthetic and an operating microscope. Occasionally, postaural approach is used to remove foreign bodies impacted in deep meatus, or those which have been pushed into the middle ear.
Unskilled attempts at removal of foreign bodies may lacerate the meatal lining, damage the tympanic membrane or the ear ossicles.
(b) Living. Flying or crawling insects like mosquitoes, beetles, cockroach or an ant may enter the ear canal and cause intense irritation and pain. First, the insect should be killed by instilling oil (a household remedy), spirit or chloroform water. Once killed, the insect can be removed by any of the methods described above.
Maggots in the ear. Flies may be attracted to the foul-smelling ear discharge and lay eggs which hatch out into larvae called maggots. There is severe pain with swelling round the ear and blood-stained watery discharge. Maggots may be seen filling the ear canal.
Treatment consists of instilling chloroform water to kill the maggots which can later be removed by forceps.
3. Keratosis obturans
Collection of a pearly white mass of desquamated epithelial cells in the deep meatus is called keratosis obturans. This, by its pressure effect, causes absorption of bone leading to widening of the meatus so much so that facial nerve may be exposed and paralysed.
Aetiology. It is commonly seen between 5 and 20 years and may affect one or both ears. It may sometimes be associated with bronchiectasis and chronic sinusitis. Normally, epithelium from surface of tympanic membrane migrates onto the posterior meatal wall. Failure of this migration or obstruction to migration caused by wax may lead to accumulation of the epithelial plug in the deep meatus.
Clinical features. Presenting symptoms may be pain in the ear, hearing loss, tinnitus and sometimes ear discharge.
On examination, ear canal may be full of pearly white mass of keratin material disposed in several layers. Removal of this mass may show widening of bony meatus with ulceration and even granuloma formation
Treatment. Keratotic mass is removed either by syringing or instrumentation, similar to the techniques employed for impacted wax(sometimes under GA). Secondary otitis externa may be present and should be treated. Patient should be periodically checked and any reaccumulations removed. Recurrence can be prevented by the use of keratolytic agent such as 2% salicylic acid in alcohol.


4. Acquired atresia and stenosis of meatus
It can result from: (a) Infections, e.g. chronic otitis externa-an important (b) Trauma, e.g. lacerations, fracture of tympanic plate, surgery on ear canal or mastoid. (c) Burns-thermal( e.g radiotherapy) or chemical.Treatment is meatoplasty. Using a postaural incision, scar tissue and thickened meatal skin are excised, bony meatus is enlarged and the raw meatal bone is covered with pedicled flaps from meatus or split skin grafts.
QUIZ? Describe- Dx-Aetiology-RX?