Spirochetes
Spiral motile bacteria, includes 2 families:1) Spirocheataceae: (free-living bacteria).2) Treponemataceae include: Treponema, Borrelia &LeptospiraTreponemaT.pallidum subsp. Pallidum causes syphilis, a long {0.2X(5-15) mm}, slender, helically coiled, spiral, G-bacilli
Structural characteristics:1) Outer sheath (glucosaminoglycan coating).2) Outer membrane (peptidoglycan).3) Endoflagella (axial filaments, encapsulated by the outer membrane & wind around the organism).4) Inner membrane (cytoplasmic membrane).5) Cytoplasm contains body fibrils (cytoplasmic tubules).
• Actively motile & so thin-→cannot be seen unless immunofluorescin stain or dark-field microscope isemployed.• Never been cultured on artificial media or in fertile eggs or in tissue culture.
Antigenic Structure:1) Does not contain LPS.2) The endoflagella: similar to bacterial flagellin protein.3) Cardiolipin (an important treponemal antigens).
4) Hyaluronidase (breaks down the hyaluronic acid in tissue & enhances the invasiveness of this organism, so it is Virulence Factor). Human with syphilis develops antibodies (can be used for staining T.pallidum by direct IF test or complementfixation test.• Also develops Ab-like substances or non-specific Abs. called reagin, directed against some Ags. distributed innormal tissues.
Pathogenesis & Clinical Findings:1) Acquired syphilis: T.pallidum transmitted by sexual contact (the infectious lesion is on the skin or mucous membrane of genitalia & only 10-20% on intrarectal, perianal & oral lesions).• It is penetrate through mucous membrane or a break in theepidermis, multiply locally-→ spread to lymph nodes-→ bloodstream.• In 2-10 weeks after infection: primary syphilis or primarylesion (a papule develops at the site of infection breaks down to form an ulcer with clean, hard base calledhardchancre), heals spontaneously.
• 2-10 weeks later: secondary syphilis or secondary lesions (a red maculopapular rash anywhere of the body) & condylomas (a moist, pale papules in the anogenital region, axilles & mouth). Also may be appear syphilitic meningitis, chorioretinitis, hepatitis or periostitis → heals spontaneously.
Secondary syphlis


• Both primary & secondary lesions are rich in spirochetes & highly infectious.• 40% progresses to the tertiary stage (latent syphilis)-→gummas (a granulomatous lesion in skin, bones, liver & degenerative changes in CNS or cardiovascular lesions. This lesion due to hypersensitivity to the organisms).
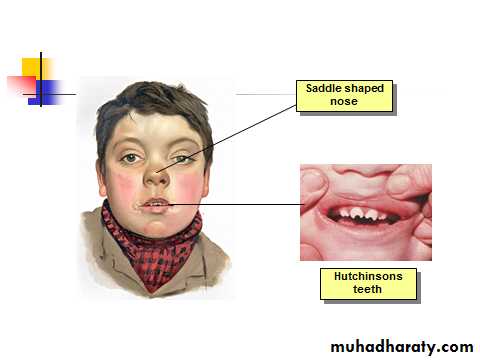
2) Congenital syphilis:• Pregnant syphilitic women can transmit T.pallidum to the fetus through the placenta in 10th-15th weeks of gestation. • Some infected fetus die, others are borne live with sings of congenital syphilis in childhood (keratitis, Hutchinson’s teeth, saddlenose, periostitis & variety of CNS anomalies).• Treatment mother during pregnancy prevents congenital syphilis.
Diagnostic Lab. Tests:• Specimens: Tissue fluids (lesions) & serum (serological tests).• Dark-field examination: drop of tissue fluid examined by dark-field microscope-→ motile spirochetes.• Immunofluorescence test: Tissue fluid stained with a fluorescein-labeled antitreponemal serum examined by fluorescent microscope-→ fluorescent spirochetes.
Serological tests:1)Nontreponemal Ag tests: using cardiolipin (extracted from normal mammalian tissue) + patient’sserum (reagin).Reagin appears in serum after 2-3 weeks or in CSF after 4-8 weeks of infection. 2 types:A. Complement fixation (CF) test or Wassermann-Kolmer test: rarely used.B. Flocculation test: VDRL (Venereal Disease Research Lab.) or RPR (Rapid Plasma Reagin). Cardiolipin form visible clumps with reagin containing sera.
2)Treponemal Ab tests: 2 types:A. Fluorescent treponemal Ab-Absorbance (FTA-ABS) test: Killed T.pallidum Reiter strain + patient’s serum +labeledantihuman gamma globulin (very specific& sensitive test)B. T.pallidum hemagglutination (TPHA) test:-Red blood cells treated to adsorb treponemes on their surface + patient’sserum-→ red cells clumped
Immunity: after cure-→ patient become susceptible. Treatment:•Syphilis less than 1 year-→ benzathine penicillin (IM).•Older (latent syphilis) -→ = = (3 times weekly intervals).•Neurosyphilis-→ penicillin (large amount, IV).
Epidemiology:Transmitted sexually.An infected person may remain contagious for 3-5 years.Control:1) Treatment of all discovered cases. 2) Follow-up on sources of infection & contacts. 3) Safe sex.
Borreliae (Borrelia SPP.) 1) Relapsing Fever•(Borrelia recurrentis) transmitted by the human bodylouse. Endemic relapsing fever in western USA (B.hermsii) transmitted by ticks (Orinthodoros hermsii). • Irregular spiral {0.3 X (10-30)μm}, flexible motile has many endoflagella. Stained by bacteriological dyes & blood stains (Giemsa’sor Wright’sstains).•Can be cultured in fluid media containing blood, serum ortissue or in chick embryos
Antigenic Structure:Have antigenic variation-→ relapsing course due to the multiplication of antigenic variants against which the host must then develop new Abs. After 3-10 relapses-→Ultimate recovery (associated with the presence of Abs against antigenic variants).
Pathogenesis & Clinical Findings:After incubation period (3-10 days), sudden chills & fever (spirochetes found in blood). The fever persists for (3-5 days, febrile period). Then declines leaving the patientweak but not ill (afebrile period), followed by a 2nd attack of chills, fever,headache & malaise(3-10 such recurrences)-→ recovery
Diagnostic Lab. Tests:•Specimens: Blood (during fever) for smear & animal inoculation.•Smear: Thin or thick blood smear stained with Giemsa’s or Wright’s→ Large, loosely coiled spirochetes amongthe red cells.
Animal inoculation: White mice or rats inoculated (I.P), after 2-4 days-→stained blood film for examined of spirochetes. Serology: + ve VDRL or CF testsImmunity: Short duration.Treatment: Tetracycline or erythromycin & penicillin for single day may be sufficient
2)Lyme Disease (B.burgdorferi) transmitted by tick called Ixodes.• Spiral, highly motile, stained with acid & aniline dyes &by silver impregnation techniques.• Isolated from erythema migrans skin lesions & ticks.• Grows in a complex medium (BSKII medium), seldomused because it takes 6-8 weeks to grow & lackssensitivity with low diagnostic yield
Antigenic Structure:Have large No. of lipoproteins (Outer Surface Proteins; Osp A-F) → help this organism live in the very different tick & mammalian hosts
Pathogenesis & Clinical Findings:• Transmitted to human by injection of the organisms intick saliva, migrates (from the bite site) → skin lesionscalled erythema migrans (a flat reddened area near the tick bite slowly expands with central clearing, begins 3 days to 4 weeks after bite) →flu-like illness with fever, chills, myalgia & headache (the initial stage) →dissemination by lymphatics or blood to the other skin area & organs (the second stage) occurs weeks to months later (arthralgia & arithritis, meningitis, cardiac disease).• The third stage begins years later with chronic skin,nervous system or joint involvement (the organism can be isolated from all these sites).
Erythema migrans(lyme disease)(B.burdgorferi)

Diagnostic Lab. Tests•Can be established clinically by observing the erythema migrans, if not present→diagnostic lab.T.•Specimens: Blood (serological tests) & biopsy (smear). -Serology: IFA, EIA or ELISA, Western blot.•Molecular probes: PCR (detection of B.burgdorferi DNA in body fluids).
Immunity:4-6 weeks after infection IgG to OspA & OspB. Treatment:• Amoxicillin or doxycycline (20-30 days).• Arithritis: penicillin + probencide (30 days or longer).
Epidemiology & Control:• In USA, Europe & other areas.• Mice & deer (the main reservoirs), rodents & birds also infected.• Prevention by avoidance ticks (using insecticides for control)• OspA vaccine efficient 66-76 % for those who live or work in endemic areas.
Leptospira & LeptospirosisLeptospirosis includes 2 worldwide diseases:1) Infectious jaundice (L.interrogans serovar. canicola) (dogs) 2) Weil’sdisease (L.interrogans serovar. icetrohaemorrhagia)(rats).• Tightly coiled, thin, flexible spirochetes {(0.1-0.2) X (5-15) μm}, one end as a hook & actively motile. Does not stain,seen by dark-field microscope as a chain of minute cocci.Grow aerobically at 28-30Cº in serum containing media(Fletcher’sor Stuart’smedia)-→ diffuse zone of growth.
liptospira

Antigenic Structure:Have LPS variable from one strain to another (used for classification & determines the immune response).
Pathogenesis & Clinical Findings:Infection results by ingestion of water or food contaminated with leptospirae from urine of dog, rats, mice, cattle, swine & others (rare through mucous membranes or breaks in the skin). After incubation period (1-2weeks), variable febrile onset, flu-like illness (spirochetes in blood) → establish in parenchymatous organs (liver & kidneys) → hemorrhage & necrosis of tissues & dysfunction of organs (initial phase) →second phase, when IgM titer rises, aseptic meningitis,nephritis, hepatitis & may be skin, muscle & eye lesions.
Diagnostic Lab. Tests: Specimens: Blood, CSF, urine & tissues.•Smear: Dark-field microscope or fluorescein-conjugated Abs or immunohistochemical techniques. • Culture: Fletcher’ssemisolid medium (8weeks). -Animal inoculation: hamsters or guinea pigs. • Serology: microscopic slide agglutination test.
Immunity: serovar specific immunity but reinfection with different serovar may occur. Treatment:• Mild disease: doxycycline, ampicillin or amoxicillin(orally)• Sever = : penicillin or ampicillin (I.V).