


TONGUE PROTHESIS
Dr. Monia MN Kandil
صناعة \ خامس اسناند. منية م(11)4\4\2017
Definition of the ? ? ? ? ? ? ?
.It’s
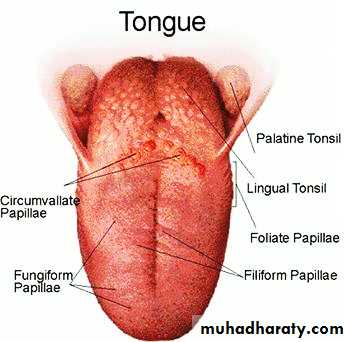
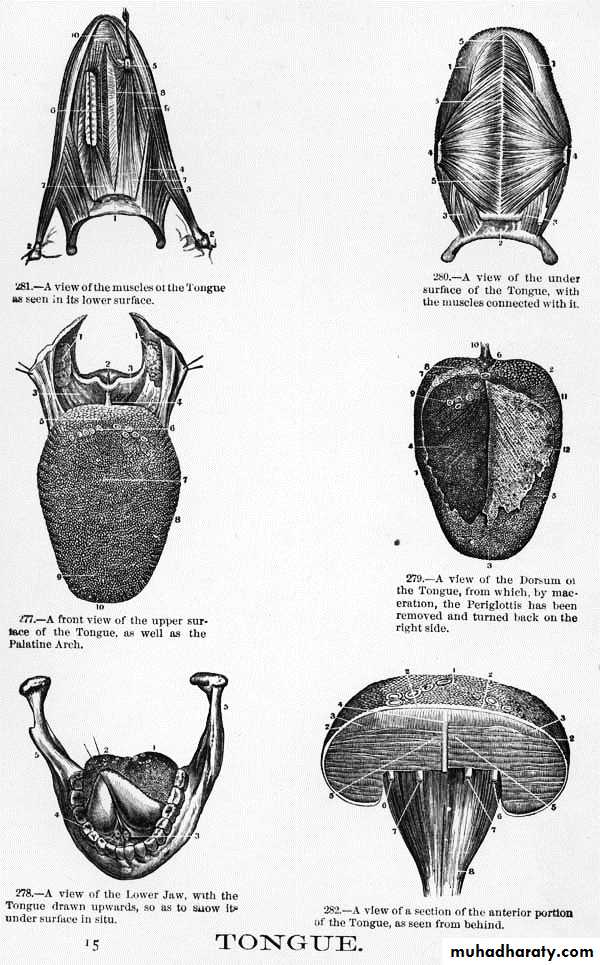
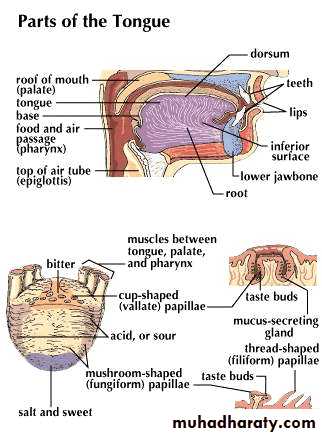
a mucous membrane bag stuffed with muscles. The tongue bluges upwards from the floor of the mouth, and its posterior part forms the anterior wall of the oral part of the pharynx. It consists of mass of striated muscles interspersed with little fat & numerous glands, especially in the posterior part.
Muscles of the Tongue
• 1-Intrinsic muscles• 2-Extrinsic muscles
• 3-Accessory muscles
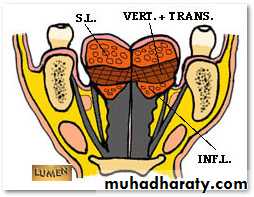
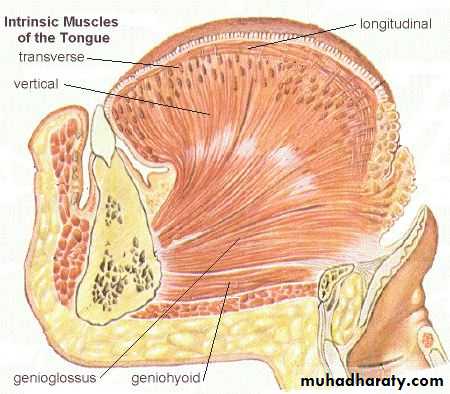
Intrinsic Muscles of the Tongue
Inferior and Superior Longitudinal Muscle:Go the length of the tongue
moves tip up and down
Transverse Muscle:
Go across the tongue
narrows and lengthens the tongue
Vertical Muscle:
Go up and down in the tongue
flattens and depresses the tongue
Extrinsic muscles:
• a- Genioglossus muscle.
• b- Hyoglossus muscle.
• c- Styloglossus muscle.
• d- Palatoglossus muscle.
•
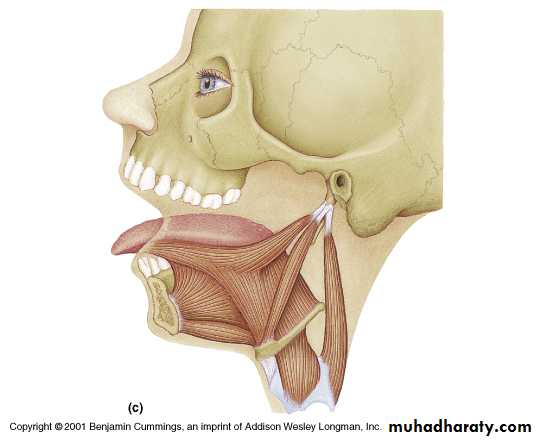
Genioglossus
StyloglossusHyoglossus
Palatoglossus
• The extrinsic muscles attach the tongue to the hyoid bone, mandible, soft palate, and the styloid process of the temporal bone.
• The extrinsic muscles reposition the tongue, while the intrinsic muscles alter the shape of the tongue for talking and swallowing.
Extrinsic tongue muscles
Accessory muscles:Which are indirectly affecting the tongue. These are:
Suprahyoid muscles
• Infrahyoid muscles
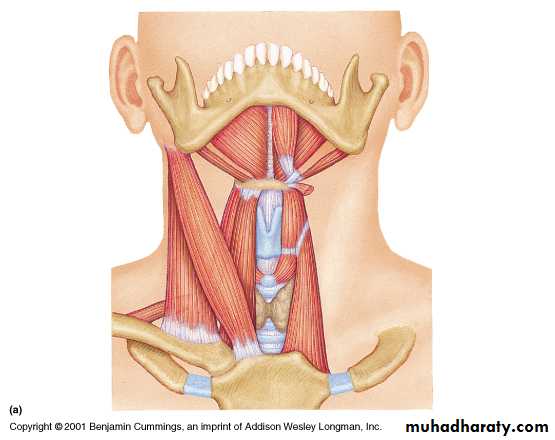
Posterior belly
Anterior bellyStylohyoid
MylohyoidGeniohyoid
Infrahyoid
DigastricMylohyoid
Stylohyoid
Geniohyoid
Suprahyoid muscles attach the hyoid bone to the mandible and are partly attached to the base of the skull
Infrahyoid muscles attach the hyoid bone to the sternum. They pull the hyoid bone downward
Functions of the Tongue
1- Mastication and deglutition.
2- Speech.
3- Taste.
4- Secretion: mucins - enzyme lingual lipase.

Functions of the Tongue
• In addition to previous normal physiologic function:• 5. Role in stabilizing complete denture.
6. Tongue dorsum side is pressed against the back of upper comp. dent. to prevent it’s dropping. While the tip is pressed down-word against the ant. Ling. Surf. Of lower dent. when lower lip tend to force the dent. back-word.
Clinical significance of the Tongue
1- Tongue size
2- Tongue position
3- Muscular development
& Neuromuscular control
Clinical significance of the Tongue
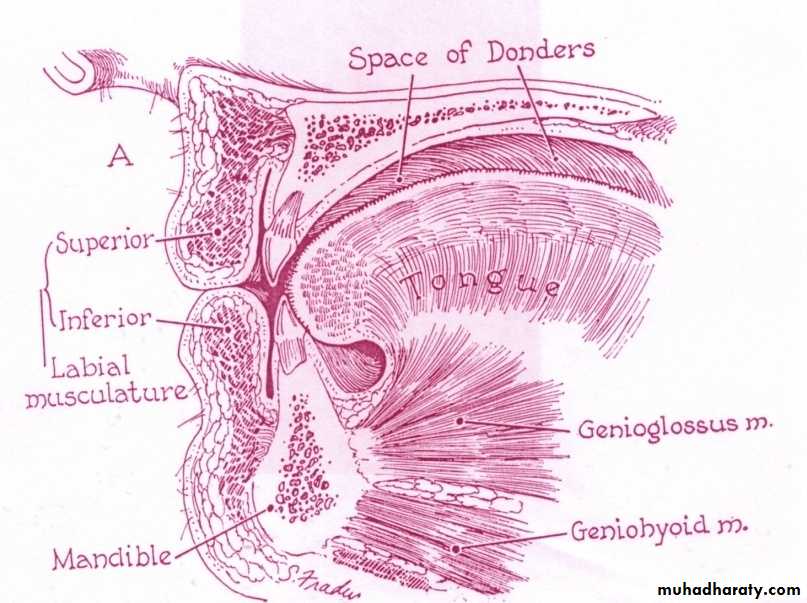
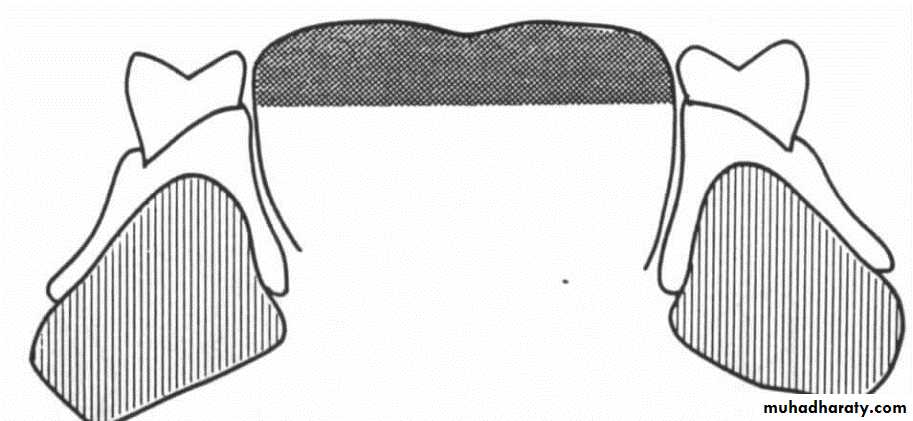
1- Tongue size:* Occupies the cavity between the ridges, teeth & hard palate except for a small air space-less than 1cm in height-beneath the hard palate called THE SPACE OF DONDERS
1- The size of the tongue
Normal size
MicroglossiaMacroglossia
Acquired macroglossia &
increased muscular tonicity
Inadequate upper denture
Unreplaced missing posterior teeth
Abnormal masticatory habit
2- Tongue position:
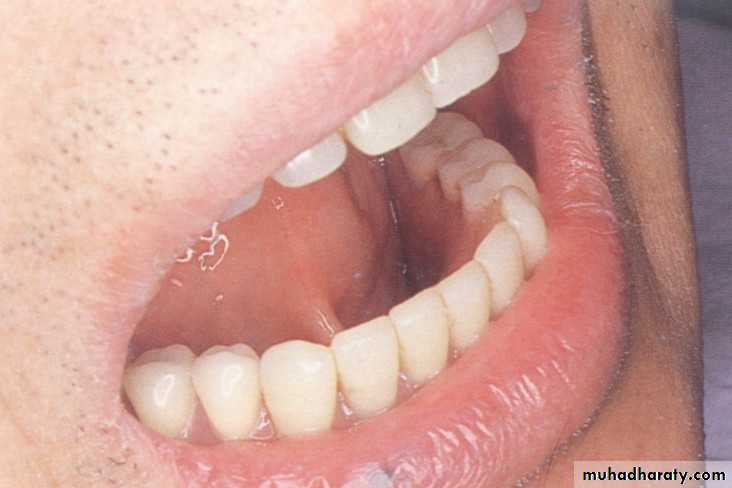
*completely fills the floor of the mouth. The dorsum is round, smooth & free of muscular contractions. The lateral borders rest on the occlusal surface of the posterior teeth & the apex rests on the incisal edges.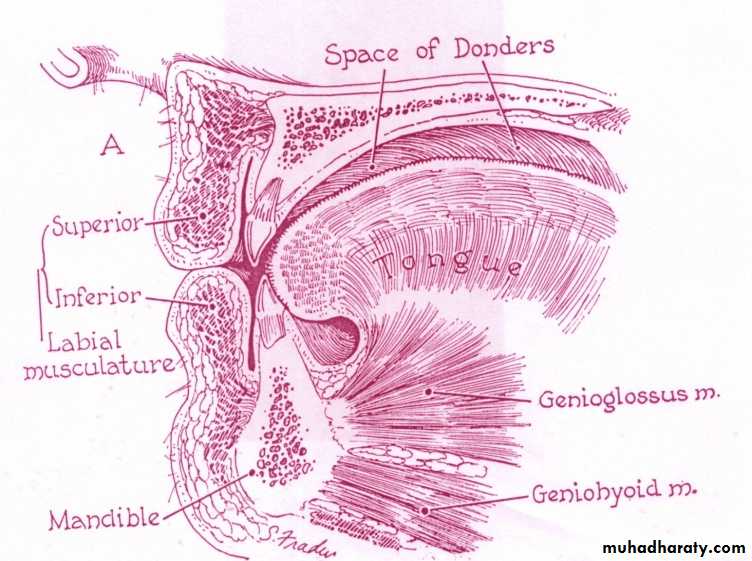
Tongue Position

Normal Resting position (border seal & stability, mastication & deglutition)
Retracted tongue position
Too high occlusal plane
Mal-positioned teeth
Excessively thick palate
Methods To Improve Retracted Tongue position

Tongue exercises
Lingual groove
Acrylic bead

3- Muscular development & Neuromuscular control:
More powerful tongue is associated with loose or inadequate dentures or unreplaced missing teeth, this leads to greater muscular tonicity.Neuromuscular control refers to the functional forces that affect the retention, it depends on:
Arch arrangement
Size of artificial teeth
Contour of the lingual flange
Normal resting & functional movement during border molding maintain the border seal & stabilize the denture.
Role of the Tongue in peripheral lingual seal
1- The tip of the tongue controls the bolus of food & places it on the occlusal surface of the teeth.2- The lingual extensions cover the sublingual glands.
3-Activation of superior constrictor muscle affect the sealing in the distolingual area, while the activation of the mylohyoid muscle affect the sealing in the molar area. Activation of the genioglossus muscle influence the sealing in the sublingual fold space.
Role of The Tongue in Posterior Palatal Seal


During swallowing, the dorsum of the tongue presses against the posterior border of the tray, displacing the palatal tissues superiorly with only minimal downward pressure by the tensor veli palatini, producing an effective posterior palatal seal.
Role of the Tongue in centric jaw relation
1- Contour of the occlusal rim:
a- The occlusion rim must have arch forms that are correctly related to the pattern of the tongue & muscular activities.
b- The lateral borders & the tip of the tongue must have freedom to move naturally during speech & deglutition.
2- Occlusal plane determination:
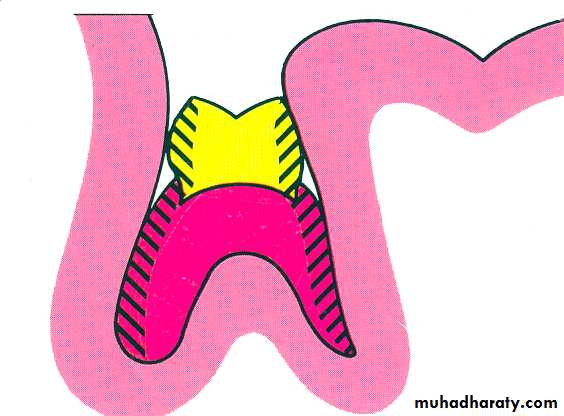
The occlusal plane should be below the lateral borders of the tongue to prevent food from falling into the lingual vestibule.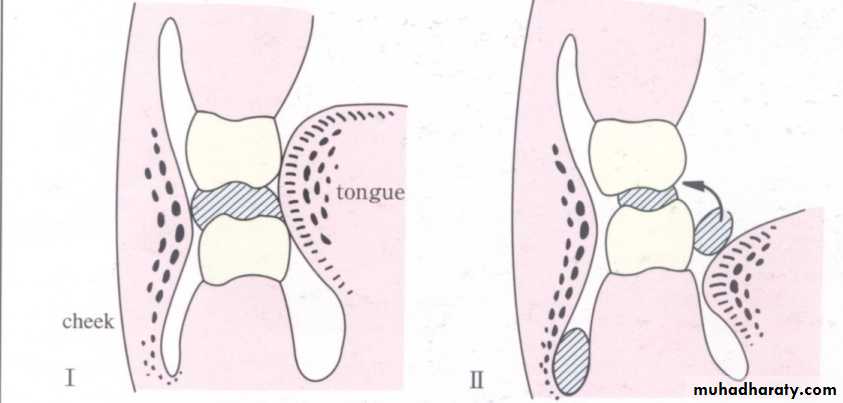
Role of the Tongue in centric jaw relation
• Approaches for occlusal plane determination:• Camper’s plane
• Corner of the mouth & retro-molar pad
• Lateral borders of the tongue
Role of the Tongue in arch arrangement & size of posterior teeth
1- The proper position for the teeth is at a point where the pressure of the tongue & cheek balance each other, in this way the denture will occupy the neutral zone in the mouth.2- The lower posterior teeth must be positioned so that when the tongue is at rest it lies comfortably against them & yet they don’t encroach upon the cheek & not overhang the tongue.
3- The occlusal surface area of the artificial post. teeth should be smaller than that of the natural one in order to reduce the load on the supporting tissues.
Role of the Tongue in contouring the lingual flange
The lingual flange should incline medially & inferiorly.
Role of the Tongue in managing the finished denture
Normal resting tongue position & swallowing pattern is important in retaining & stabilizing both upper & lower dentures.

Removable Prostheses
For Glossectomy DefectsGlossectomy Defect
Malignant tumors of the tongue, floor of the mouth &/or the mandible often require extensive resection of the tongue.Glossectomy, an extremely disabling surgical procedure. Affect the neuromuscular coordination of the tongue that plays an important role in 3 functions: mastication, swallowing and speech.
The nature of disabilities is dependant upon the volume & site of resected tissues, impact of radiation, motor & sensory control of the remaining tongue.
Tselios N. 2004.
Normal swallowing alone requires the fine coordination of 12 cranial & 6 cervical nerves, and 60 muscles. This create a great challenge for clinician to replace this sensitive, highly mobile, muscular organ with hard immobile acrylic resin/or such material and restore acceptable oral competency & function.
Prosthodontic Rehabilitation following total & partial Glossectomy
Tongue defects due to tumor removal can result in either…… total or partial glossectomy.
Speech or deglutition aid prosthesis to be placed either in the maxillary or mandibular arch
The factors influencing prosthetic prognosis of restoring tongue:
• Amount & position of the tongue remaining part(s).• The retaining means (teeth, denture or implants) are very important especially in patient with total glossectomy .
• The procedure combines with the glossectomy (eg. Mandibulectomy, palatectomy, radiation therapy).
• The condition of surrounding structures.
• Patient acceptance.
Source: Kharchaf M, Zaki H. 2010
Major objectives of prosthetic rehabilitation for total glossectomy (TG) without surgical reconstruction:
• Reduce oral cavity size to improve resonance.
• Direct food bolus into oro-pharynx.
• Protect the underlining fragile mucosa if skin flaps not used.
• Develop surface contact with surrounding structures during speech & swallowing.
• Improve appearance & psychological adjustment.
Materials used to construct tongue prostheses
In the past:Plastic materials, such as silicon or polyvinyl chloride that used for facial reconstruction (disadvantage: difficult to master), or acrylic materials which have allergic effect on manufacturer or patients.
Source: Taicher Sh, Bergen SF. 1981
Recently:
Polysiloxane materials, which overcomes many former shortcomings has evolved• Not toxic or allergic.
• Can well withstand the forces to which it’s subjected.• A close texture & natural appearance of the tongue.
• Also it gives a retention means for the tongue prosthesis to the max. dent. (Especially in patients with tightened scar tissue in the floor of the mouth).
• Easily cleaned.
• Easily manipulated (removed by gentle squeezing it from its undercut).
Advantages of polydimethylsiloxane-acrylic resin prosthesis:
Cannot replace all the functions of the tongue.
The ability to replace the speaking is difficult, although it’s a plastic & moldable one (it may help in limited degree in field the space & improve the resonance of sounds only).Disadvantages of polydimethylsiloxane-acrylic resin prosthesis:
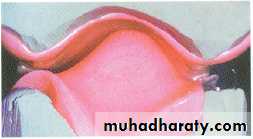
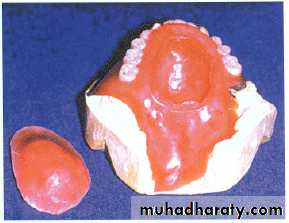
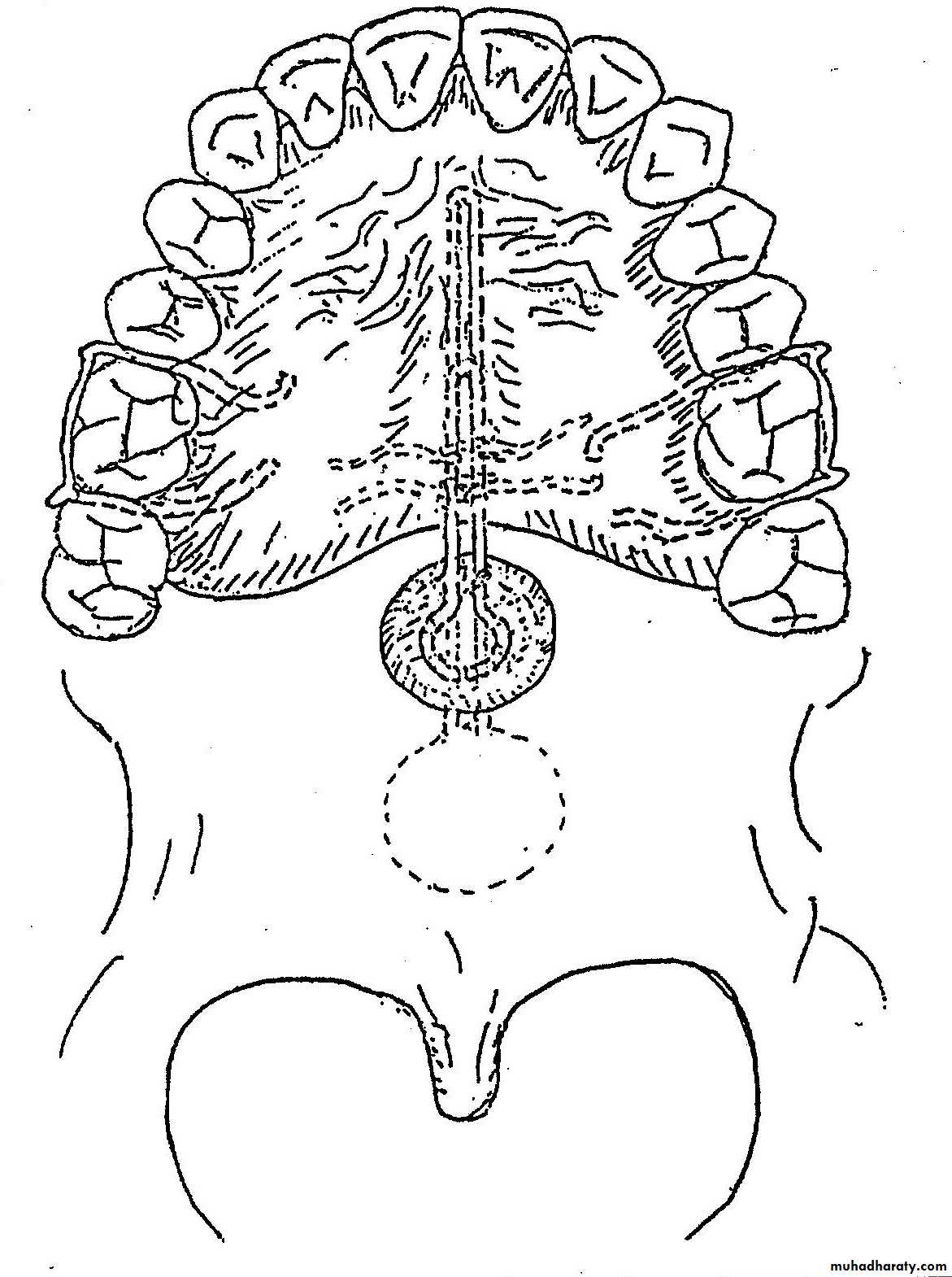
Treatment of choice: [Mandibular tongue prostheses*
Define as: dome-shape prosthesis fills the palatal vault, as much as normal tongue when mouth closed.Types:
For speech.
For swallowing.
For both speech & swallowing.
Total Glossectomy
*According to Leonard and Gillis/ Bumer, they recommend using a mandibular prosthesis with little or no residual tongue remains. They notice an improvement on speech without clear evidence on swallowing.

For speech: should have ant. elevation to facilitate articulation of ant. linguo-alveolar sounds, /t/ & /d/. it also should have posterior one to articulate for linguo-palatal sounds, /g/ & /k/. Both improve vowel production.
For swallowing: should be sloped posteriorly to guide food to pharynx.
For both speech & swallowing: both types of TP can fabricate as interchangeable speech & swallowing prostheses attached via the retentive button on the base portion (this used for highly motivated patient).Source: Taylor. Th. 2000.
In mandibular TP, checking for adequate palatal contact of the tongue.
And ensuring freedom in lateral and protrusive movements.Some important notes
In total glossectomy, the mandibular tongue prosthesis is the treatment of choice, but in situation involving:
complete edentulous patient and an irradiated, desorbed mandibuler ridge or patient with very week abutment, Maxillary TP / PAP should be considered.

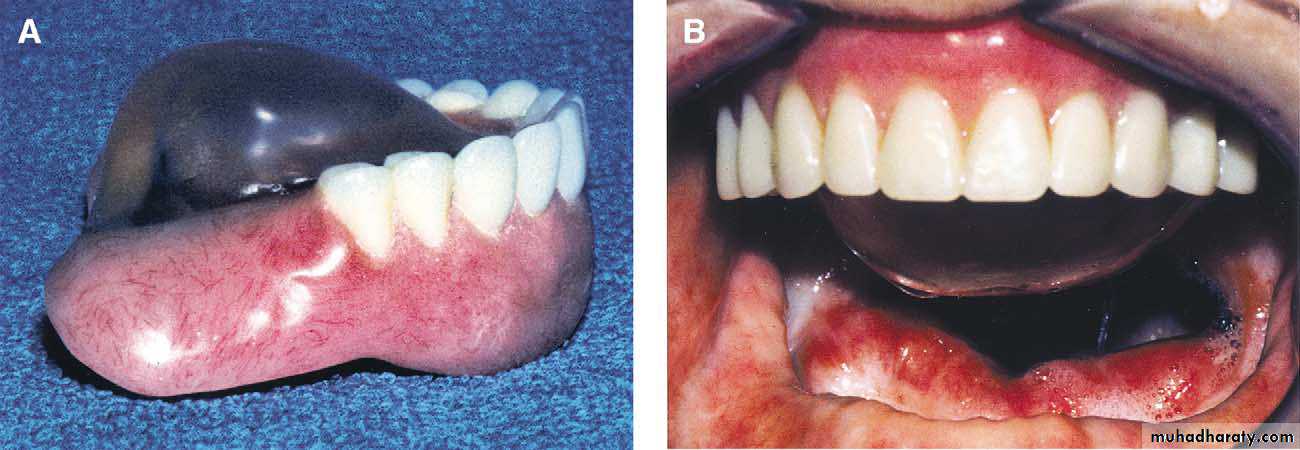
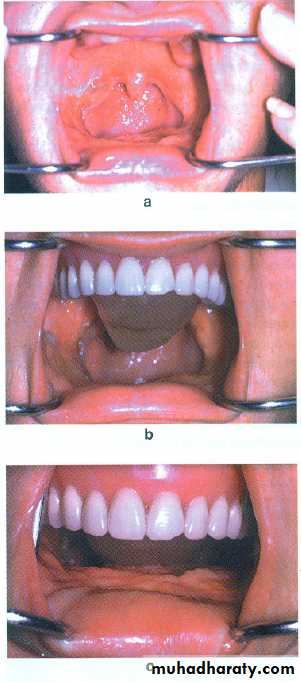
The modified maxillary denture replaces the tissue volume lost by the glossectomy and will assist the patient in swallowing.
By wax that modified intraorally until maximum contact is developed with the floor of the mouth during swallowing, then processed in acrylic resin
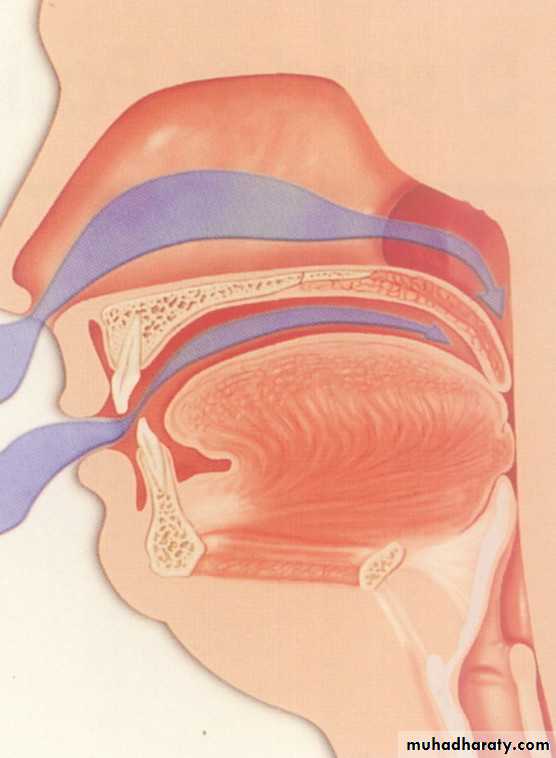
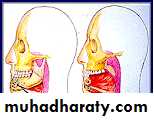
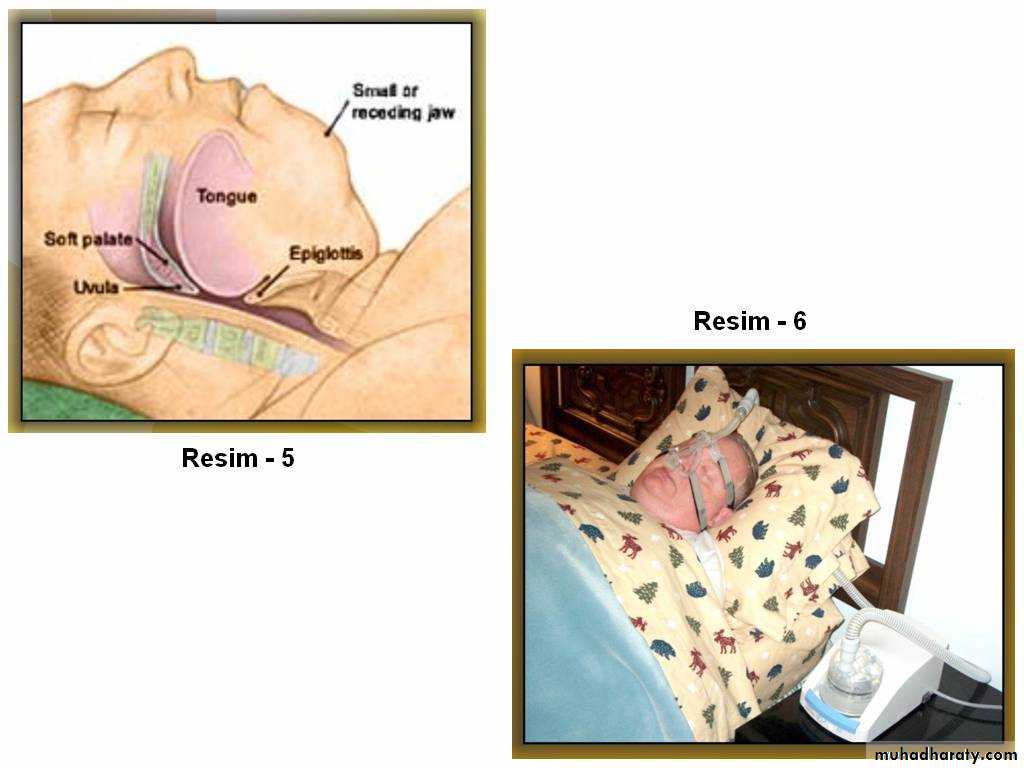
Snoring &Obstructive Sleep Apnea
Snoring
Partial obstruction of airways, (as result of tongue &/or hyoid bone dropping back toward the post. part of pharynx).Attempt to get sufficient oxygen
Velocity of air passing through airway spaces will cause flabby tissue of soft palate& uvula.Vibrate snoring sounds.
It’s more common in men, and it can be strongly suspected if the patient is a middle aged-overweight persons.Causes:
Classification of sleep apnea
According to the cause of airflow cessation it can be classified into:1- Central sleep apnea.(CSA).
2-Obstructive sleep apnea.(OSA).
3-Mixed sleep apnea.
Snoring and obstructive sleep apnea are the most common disorders.
Predisposing factors to OSA
1-Obsity.
2-Alcohal intake.
3-Smoking.
4-Craniofacial and soft tissue anomalies.
5-Pathological conditions.
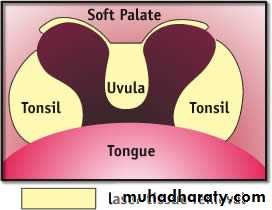
Oral condition predispose to OSA
1-Micrognathia.2-Retrognathia.
3-Angle s class II jaw relationship.
4-Macroglossia.
5-Enlarged palatine tonsils.
6-Enlarged uvula.
7-High arched palate.
8-Long soft palate.
9-Nasal septum deviation.
10-Long anterior facial height.
11-inferiorly displaced hyoid bone.
12-Steep and short anterior cranial base.
SIGNS & SYMPTOMS (S&S)
• Excessive day-time sleepiness.
• Morning headache.
• Loud snoring & Pauses in breathing.
• Waking up gasping for breath.
• Increased irritability & Depression.
• Reduced memory, attention & concentration.
• High blood pressure & Heart failure symptoms that does not effectively respond to medication.
• Frequent nocturnal urination, Xerostomia may developed.
TREATMENT MODALITIES FOR (OSA)
I-Surgery:Tonsillectomy, tracheostomy, septoplasty & uvulopalatopharyngoplasty (UPPP) removing or repositioning the redundant tissue to increase airway volume.
Radio-frequency ablation ("Somnoplasy") of the soft palate reduce the volume of tissue while preserving its anatomy.
Orthognathic surgery advance the maxilla or the mandible and the hyoid bone.
TREATMENT MODALITIES FOR (OSA)
II - Conservative treatment:1-Weight loss
2-Positional therapy
3-Nocturnal oxygen
4-Medication elimination or adjustment.
5-Positive pressure airway devices, i.e., CPAP
6-Oral appliances, which needs:
A Cephalometric radiographs to evaluate the degree of airway obstruction.
Mounted diagnostic casts todetermine if a presumed retrognathic mandibular position contributes to the collapse of the tongue against pharyngeal walls or not .
Conservative treatment
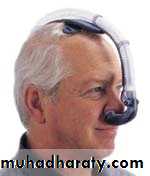
Nasal valve dilatorsActs mainly to improve patency of the nose by dilating the nares.
MASKS FOR SLEEP APNEA
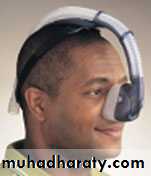

Continuous positive airway pressure (CPAP)

ORAL APPLIANCE THERAPY
Oral appliances are devices worn during sleep that aim at relieving upper airway obstruction by modifying the position of the mandible, tongue, and other oropharyngeal structures.ORAL APPLIANCES
An oral appliance is a small acrylic device that fits over the upper and lower teeth or tongue (similar to an orthodontic retainer or mouth guard). This device slightly advances the lower jaw or tongue, which moves the base of the tongue forward and opens the airway. This improves breathing and reduces snoring and apnea. The appliance is fabricated and customized for each patientOral appliances are established to treatment of OSA
Surgical high failure rate strategy.
Provide a good alternative solution for the
With simple cases
With sever cases
Simple in use
Difficult in use
Reversible
Portable & generally have low complication rate
Effective option
Unreversible
Complicated & have more complications
Limited option
Cheep
Expensive
Types of OA treated OSA:
Source: Hoekema A, Stegenga B & de Bont M. 2010.Tongue retaining appliances
(TRA)
Mandibular repositioning appliances
(MRA)
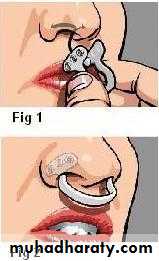
Tongue stabilizing device
Tongue posture trainers
Labial shields
Palatal lifting device

Action by:
• reposition the tongue in an anterior position by securing it with negative pressure in a soft plastic bulb.• with plastic depressor that comes into direct contact with the tongue base.
Limitation:
• Compromising nasal passage.
• Discomfort and loss of negative pressure in the bulb.
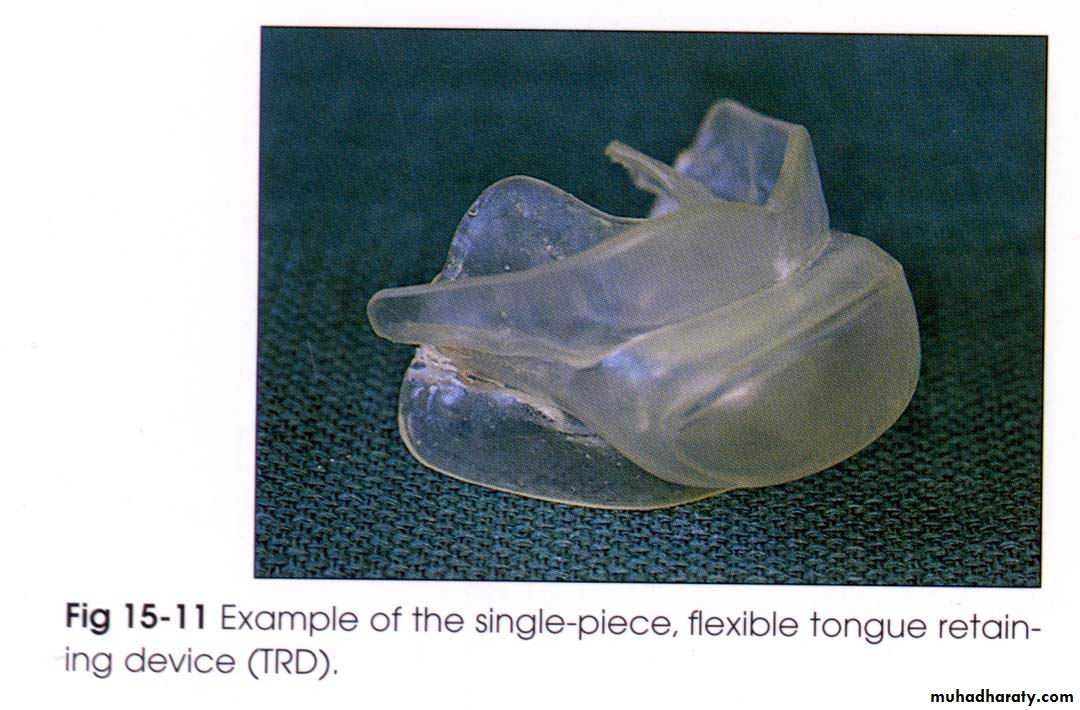
Tongue retaining appliances
Mandibular repositioning appliancesFixed position
Partly adjustable custom
Without bulb
One-piece ( more simple design)
Two-piece (more adjustable)
Boil-and-bite
. Lab-fabricated
Off-the-shelf










Boil-and-bite
. Lab-fabricatedWith bulb
Lab-fabricated


The size of bulb is selected by measuring the thickness & width of the anterior quarter of tongue, when protruded.
48%
55%Tongue retaining appliances
Mandibular repositioning appliancesFull or partial occlusal coverage
With edentulous patients
Mainly affect tongue muscles (with modified TRA/increase genioglossus EMG activity)*
Increase upper airway muscles tone (except post apnea period, genioglossus tone was lowered)*Sources: Ferguson KA. Clin Chest Med. Vol: 24, pp: 355-36, 2003. *Source: Ferguson KA. Clin Chest Med. Vol: 24, pp: 355-36, 2003. **Source: Chierici G, Lawson L. 1973.
Whom suffer from TMJ problems**
No TMJ symptoms (sensitivity)**
The amount of space between soft palate & tongue, Patient acceptance, also identify the type of oral devices.**
In patients with large tongue
In adequate protrusive ability
Advanced periodontal disease
Suitable anchor teeth
Adequate protrusive ability
Patients with normal or small tongue
Source: Ferguson KA. Clin Chest Med. Vol: 24, pp: 355-36, 2003.
Excessive salivation & temporary discomfort after awaking.Occlusion &VJR alteration.
Mucosal ulceration & soreness.
Tooth discomfort.
TMJ pain & condyl dislocation.
Concerns has been expressed that there can be a damage to the stomatognathic system. Yoshida recorded: The prosthesis maintained the desired mandibular position without craniomandibular disorders in 20 patients who wore the appliance for an average of 55 months.
Side effects & complications (for 2 types):
Bumer
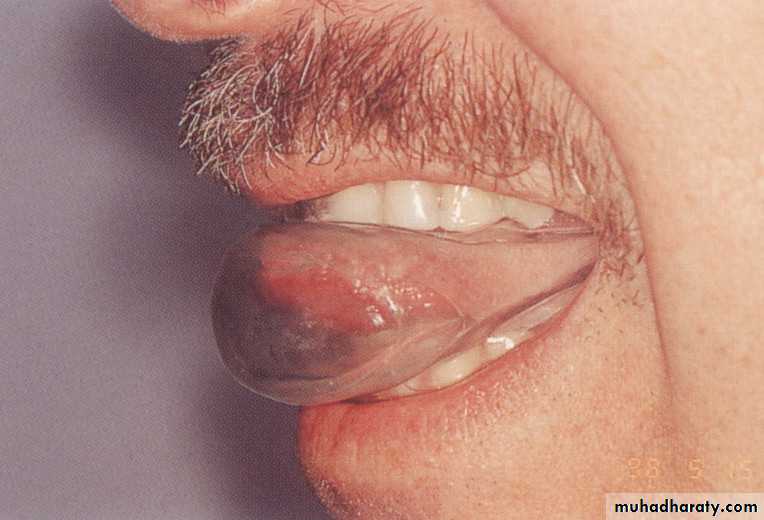
Tongue retaining appliances
Mandibular repositioning appliancesAction manner: Fallowing the same goal as the MRA (the tongue & soft palate are advanced away from the back wall of throat), work through the use of hollow bulb & sufficient vacuum to hold the tongue forward.
Source: Eckhart JE. J Califor Dent Assoc. Augest 1998.
• Made from non rigid vinyl material & the patient is instructed to protrude the tongue into the hollow bulb & the vacuum hold it there for at least 6 hours of sleep.
Disadvantage: can cause tongue tip soreness, due to the suction; that lead to difficult accommodation of the appliance.
Advantage: The Tongue advancers, since they’re not stretch the mandible, so the TMJ symptoms would not be exceeded from the usual.