Tuberculosis
Part 1Epidemiology
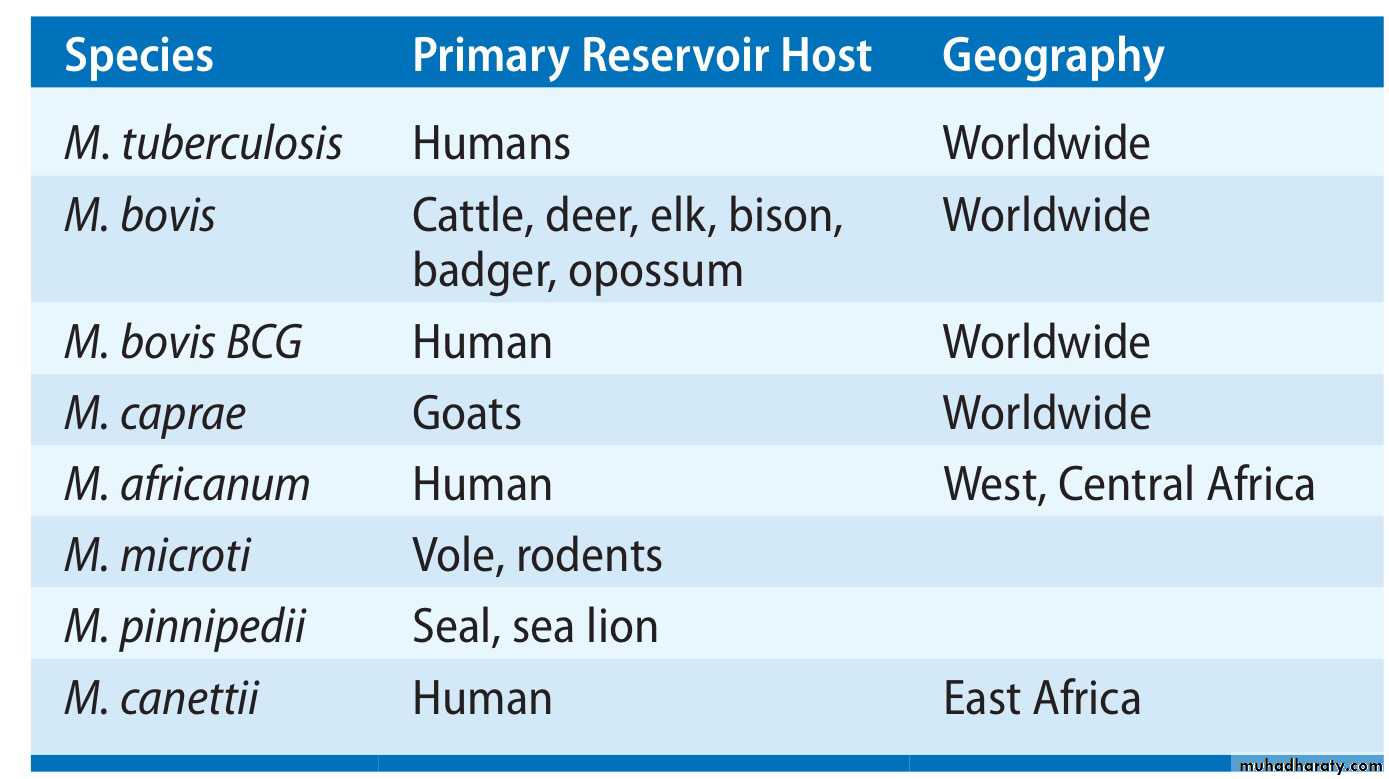
Tuberculosis (TB) is caused by infection with Mycobacterium tuberculosis (MTB), which is part of a complex of organisms including M. bovis (reservoir cattle) and M. africanum (reservoir human).In 2010, an estimated 8.8 million incident cases occurred and TB was estimated to account for nearly 1.5 million deaths, making it the second most common cause of death due to an infective disease.
one-third of the world’s population has latent TB.
Members of the Mycobacterium Tuberculosis Complex (MTBC)
Worldwide incidence of tuberculosis
Estimated new cases (all forms) per 100 000 population (WHO)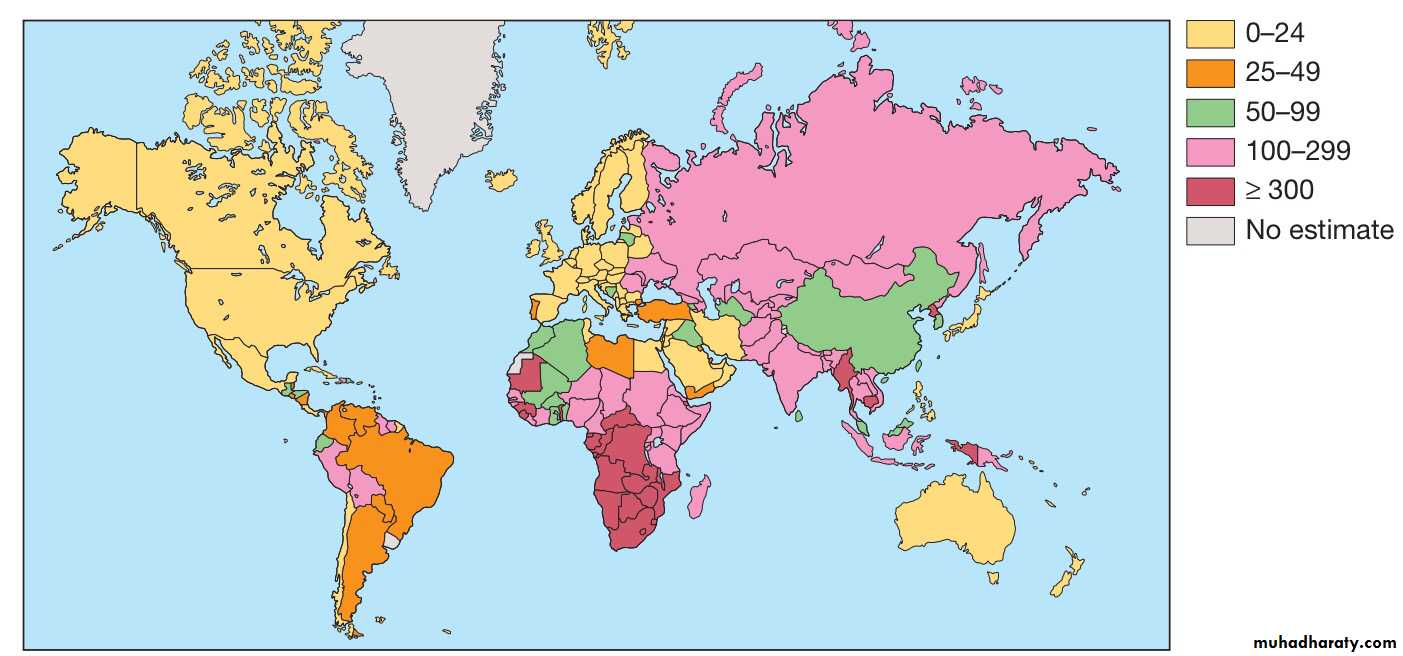
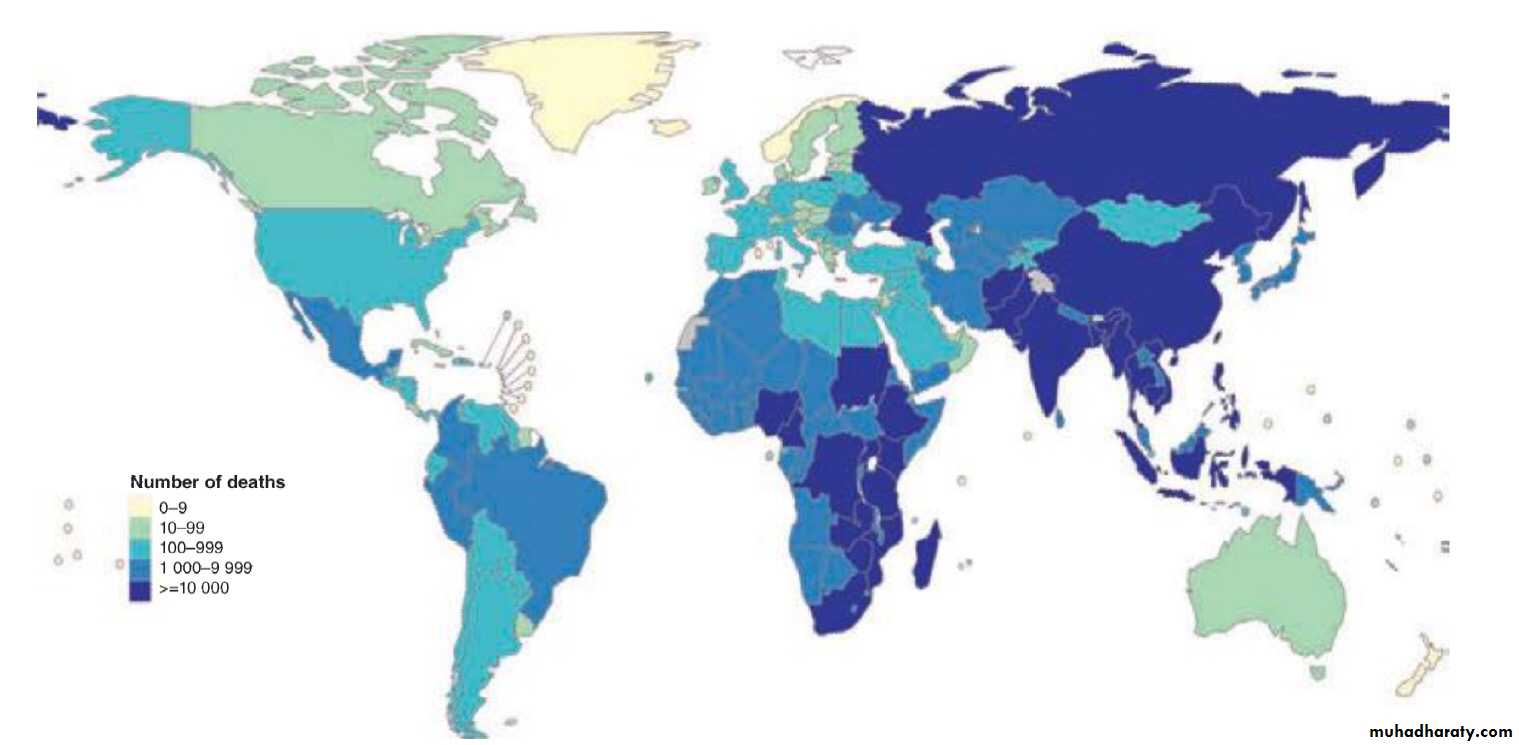
Estimated numbers of tuberculosis-related deaths in 2013
Pathology and pathogenesis
M. bovis infection arises from drinking non-sterilised milk from infected cows.M. tuberculosis is spread by the inhalation of aerosolised droplet nuclei from other infected patients.
Once inhaled, the organisms lodge in the alveoli and initiate the recruitment of macrophages and lymphocytes. Macrophages undergo transformation into epithelioid and Langhans cells, which aggregate with the lymphocytes to form the classical tuberculous granuloma.
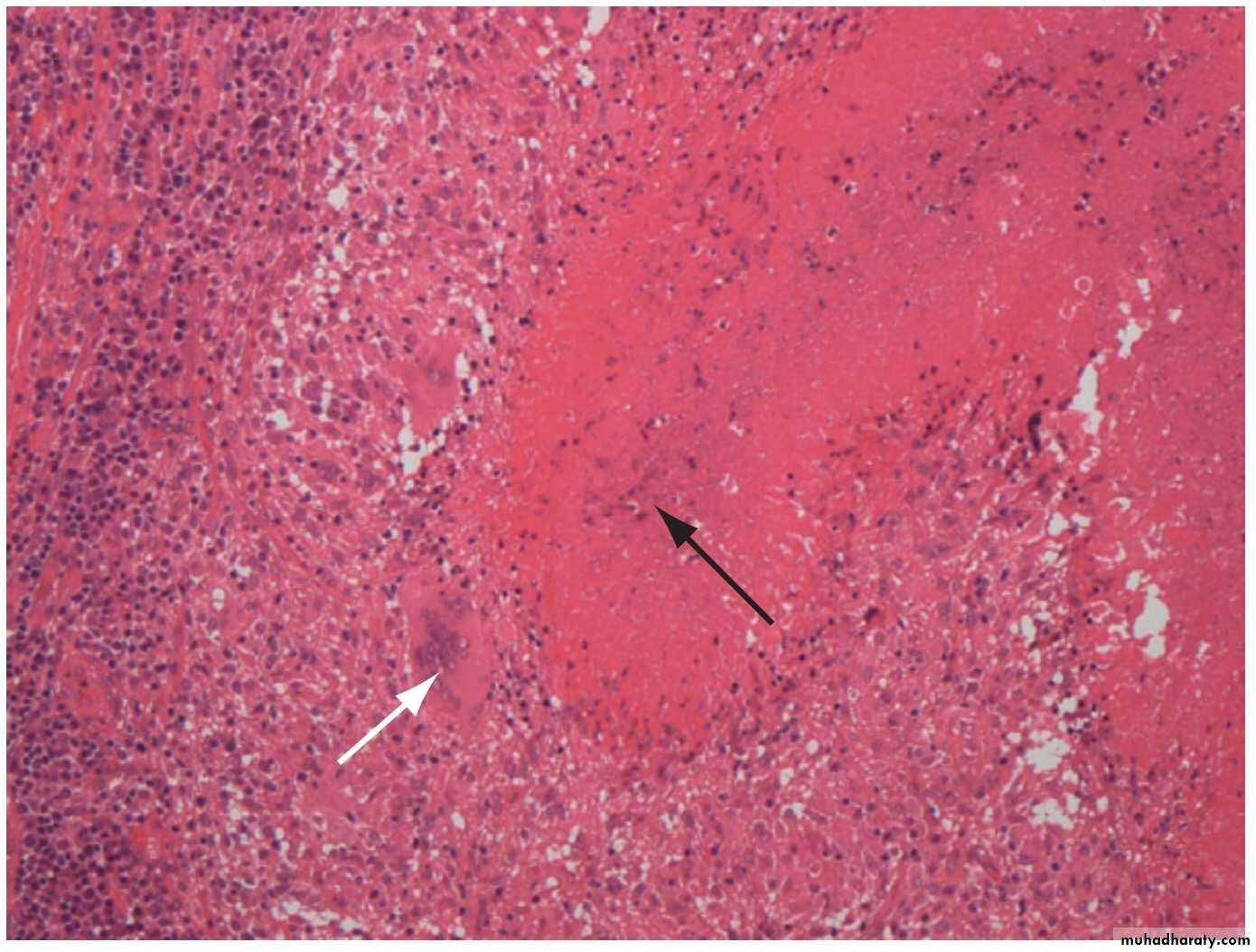
Tuberculous granuloma
Normal lung tissue is lost and replaced by a mass of fibrous tissue with granulomatous inflammation characterised by large numbers of macrophages and multinucleate giant cells (white arrow). The central area of this focus shows caseous degeneration (black arrow).Numerous granulomas aggregate to form a primary lesion or ‘Ghon focus’ (a pale yellow, caseous nodule, usually a few millimetres to 1–2 cm in diameter), which is characteristically situated in the periphery of the lung.
Spread of organisms to the hilar lymph nodes is followed by a similar pathological reaction, and the combination of the primary lesion and regional lymph nodes is referred to as the ‘primary complex of Ranke’.
Reparative processes encase the primary complex in a fibrous capsule, limiting the spread of bacilli: so-called latent TB.
If no further complications ensue, this lesion eventually calcifies and is clearly seen on a chest X-ray.
lymphatic or haematogenous spread may occur before immunity is established, seeding secondary foci in other organs, including lymph nodes, serous membranes, meninges, bones, liver, kidneys and lungs, which may lie dormant for years.
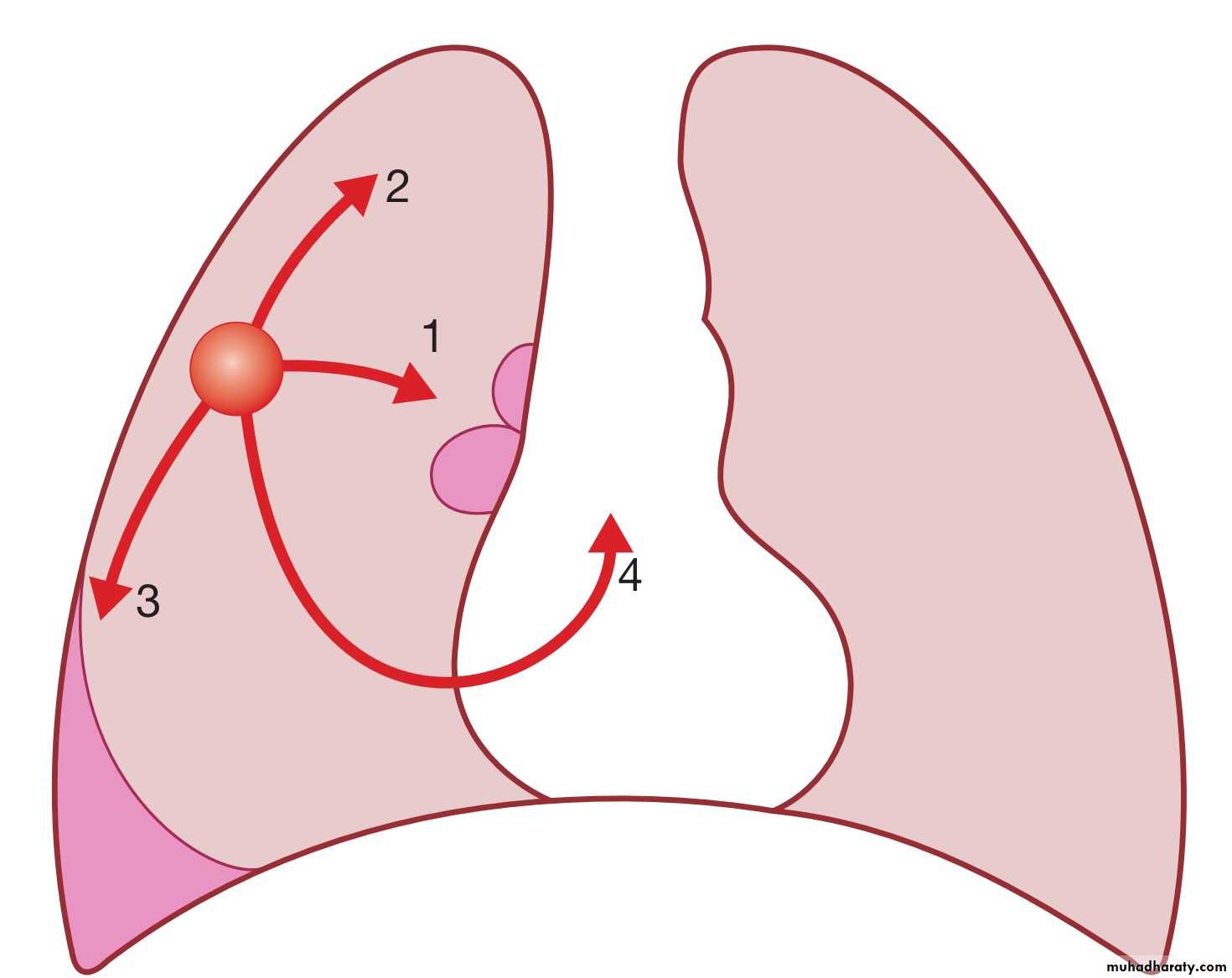
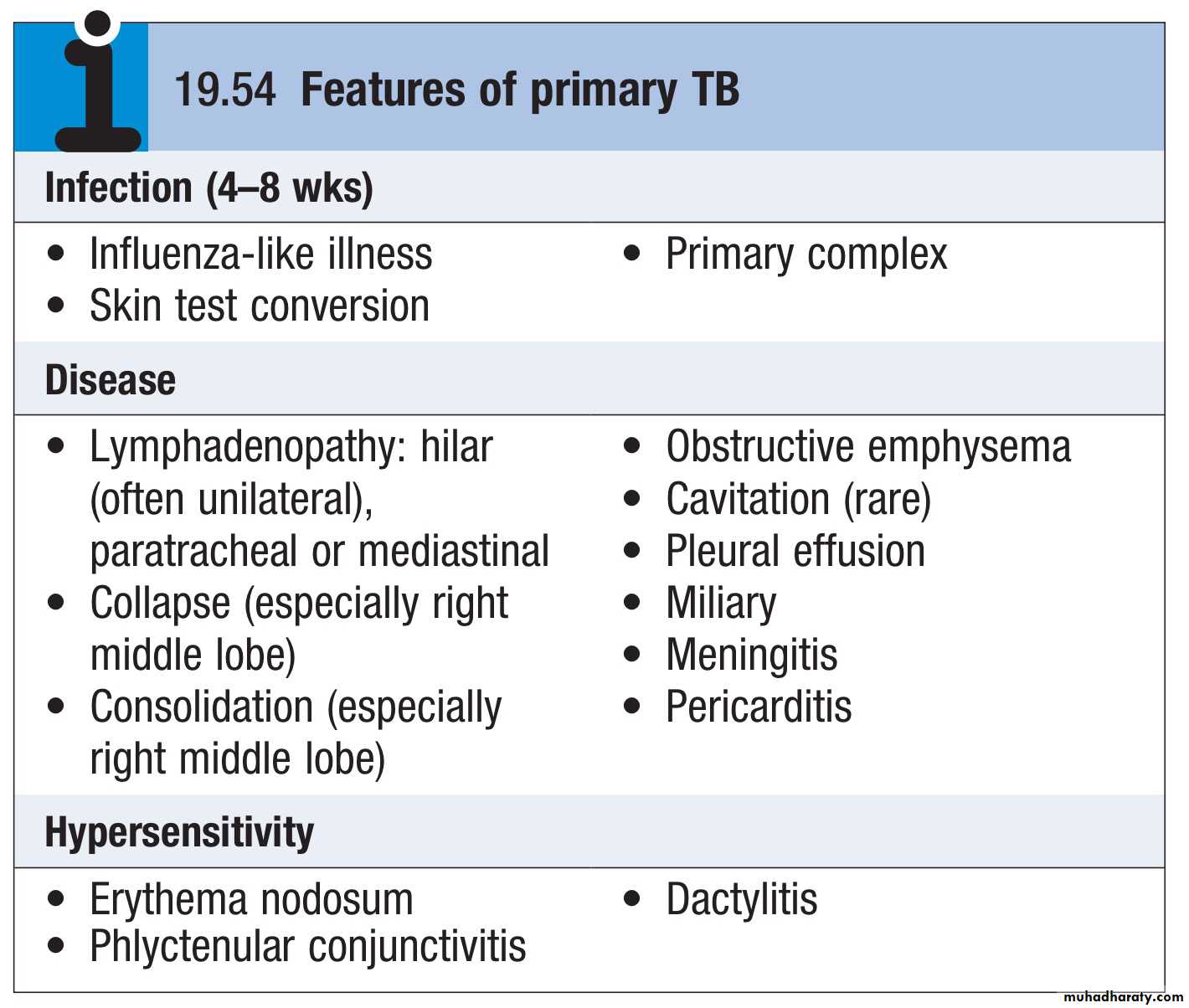
Primary pulmonary TB
• Spread from the primary focus to hilar and mediastinal lymph glands to form the ‘primary complex’, which inmost cases heals spontaneously.
(2) Direct extension of the primary focus – progressive pulmonary TB.
(3) Spread to the pleura – tuberculous pleurisy and pleural effusion.
(4) Blood-borne spread: few bacilli pulmonary, skeletal, renal, genitourinary infection, often months or years later; massive spread – miliary TB and meningitis.
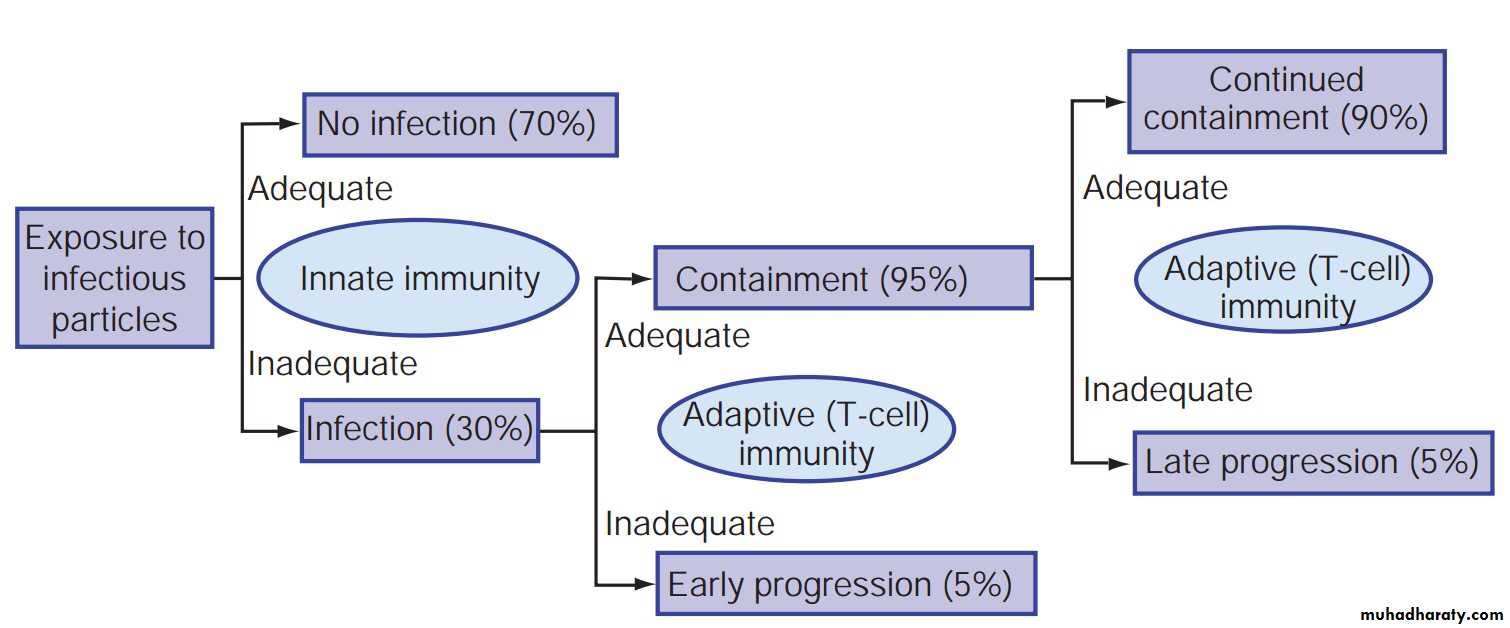
Consequences of exposure to an infectious source case of tuberculosis depending on the status of immunity.
Clinical features: pulmonary disease
Primary pulmonary TBPrimary TB refers to the infection of a previously uninfected (tuberculin-negative) individual.
A few patients develop a self-limiting febrile illness but clinical disease only occurs if there is a hypersensitivity reaction or progressive infection.
Progressive primary disease may appear during the course of the initial illness or after a latent period of weeks or months
Miliary TB
Blood-borne dissemination gives rise to miliary TB, which may present acutely but more frequently is characterised by 2–3 weeks of fever, night sweats, anorexia, weight loss and a dry cough.Hepatosplenomegaly may develop
the presence of a headache may indicate tuberculous meningitis.
Auscultation of the chest is frequently normal, but in more advanced
disease, widespread crackles are evident.
Fundoscopy may show choroidal tubercles.
The classical appearances on chest X-ray are of fine 1–2 mm lesions (‘millet seed’) distributed throughout the lung fields, although occasionally the appearances are coarser.
Anemia and leucopenia reflect bone marrow involvement.
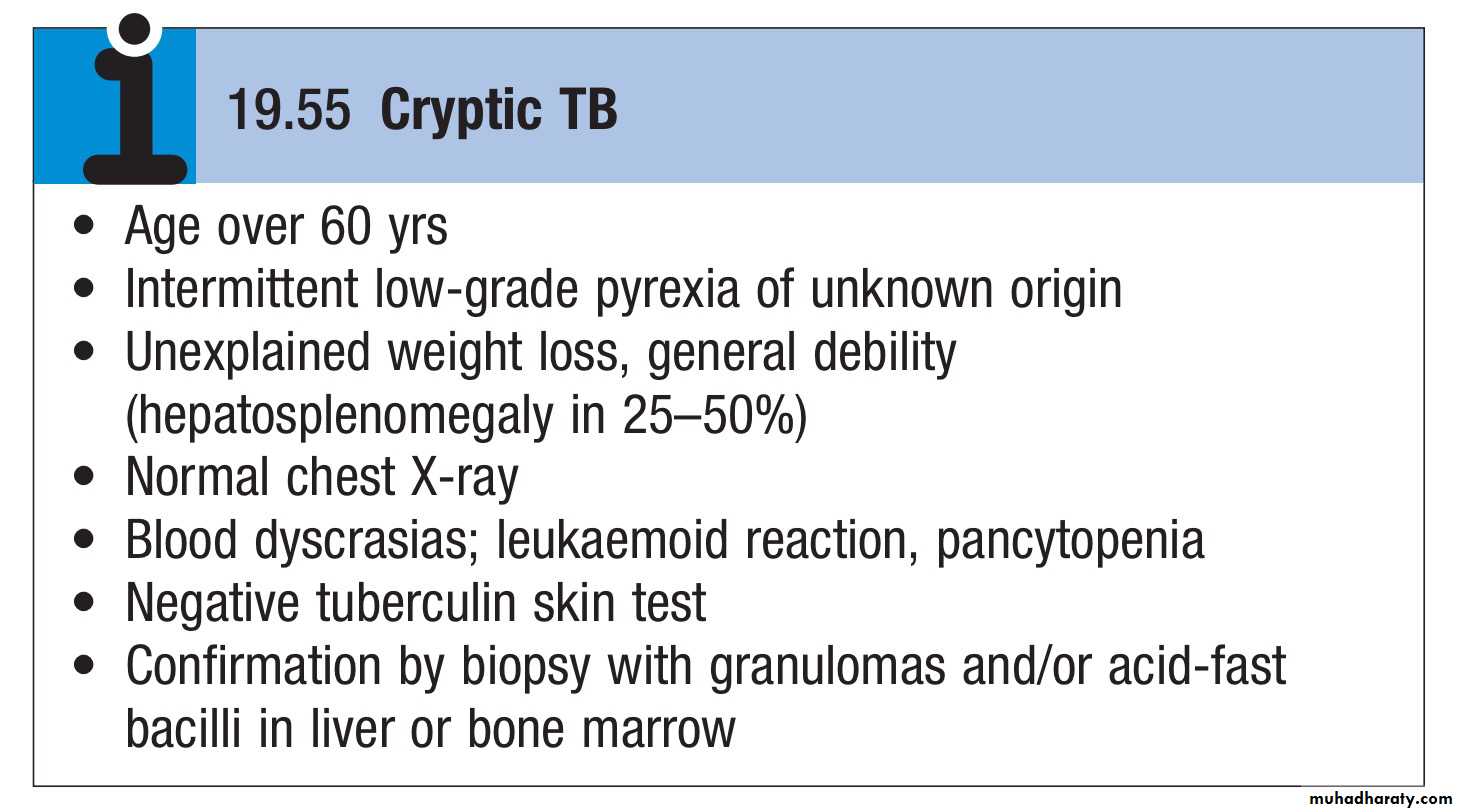
‘Cryptic’ miliary TB is an unusual presentation sometimes seen in old age.
Post-primary pulmonary TB
Post-primary disease refers to exogenous (‘new’ infection) or endogenous (reactivation of a dormant primary lesion) infection in a person who has been sensitised by earlier exposure.It is most frequently pulmonary and characteristically occurs in the apex of an upper lobe, where the oxygen tension favours survival of the aerobic organism.
The onset is usually insidious, developing slowly over several weeks.
Systemic symptoms include fever, night sweats, malaise, and loss of appetite and weight, and are accompanied by progressive pulmonary symptoms.
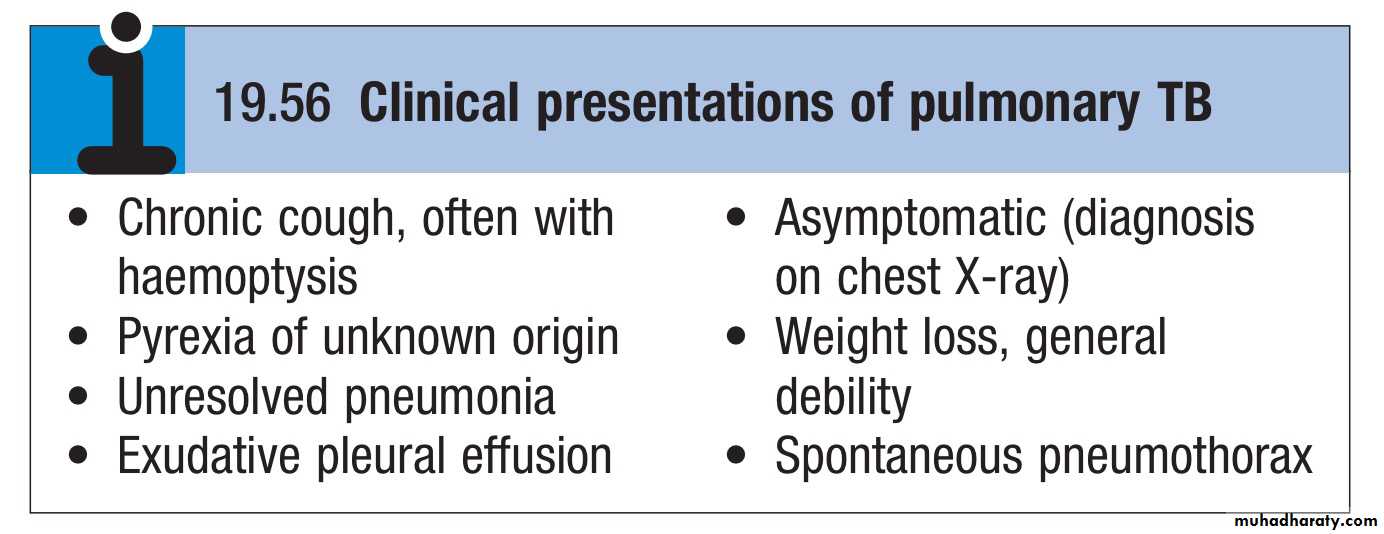
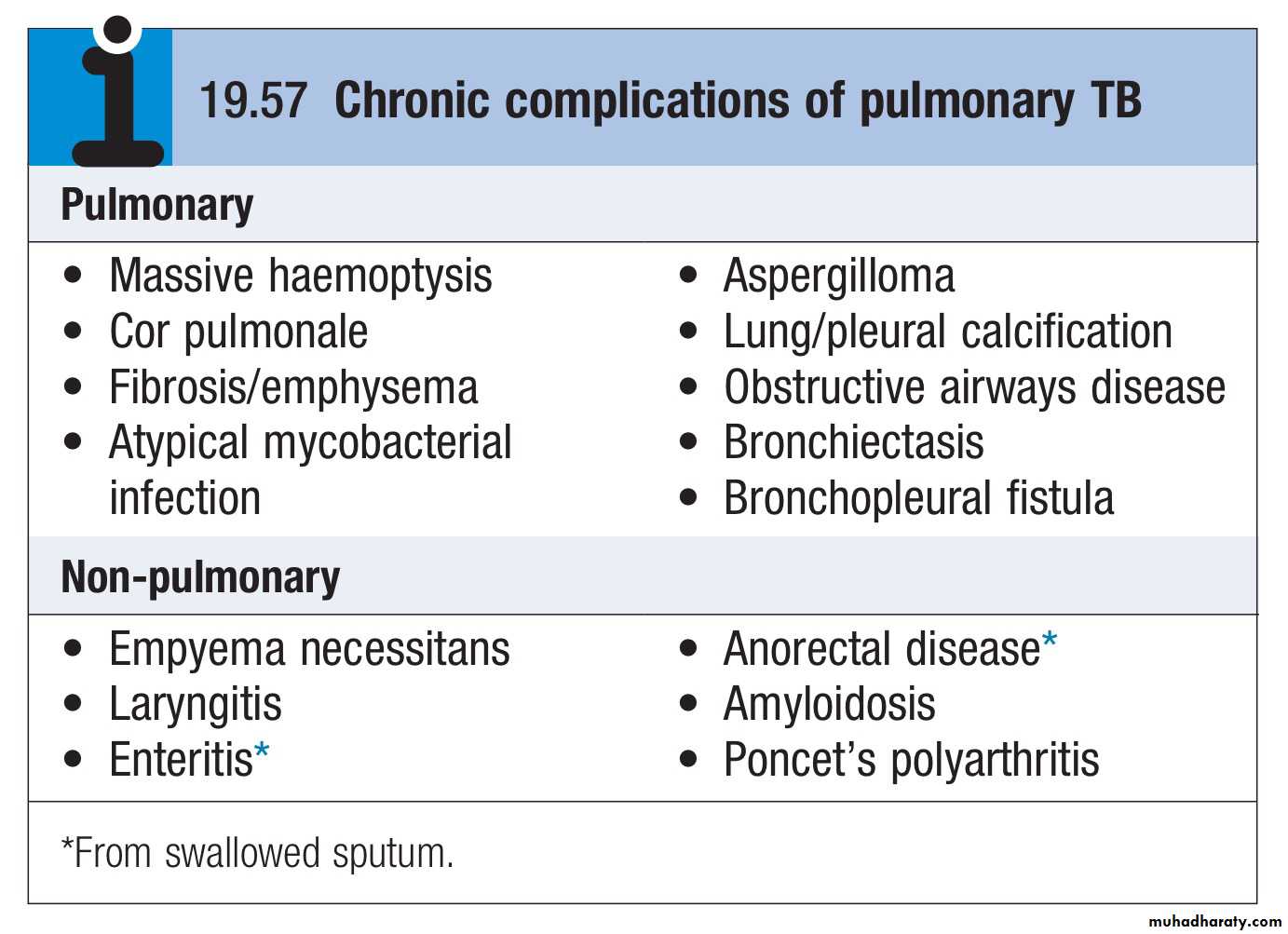
This form of TB may present with one of the complications:
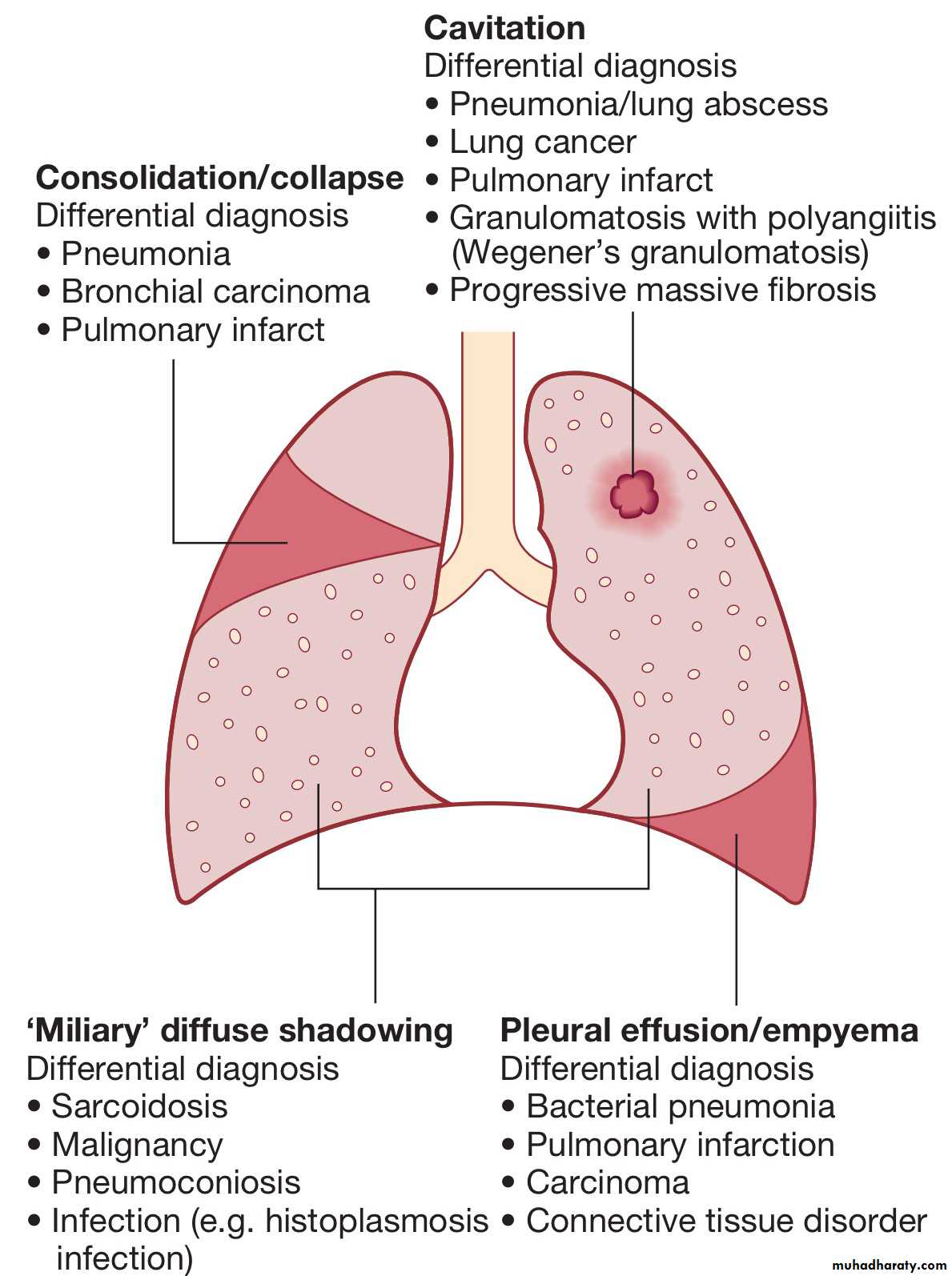
Radiological changes include ill-defined opacification in one or both of the upper lobes, and as progression occurs, consolidation, collapse and cavitation develop to varying degrees.
It is often difficult to distinguish active from quiescent disease on radiological criteria alone, but the presence of a miliary pattern or cavitation favours active disease.
In extensive disease, collapse may be marked and results in significant displacement of the trachea and mediastinum.
A caseous lymph node may drain into an adjoining bronchus, leading to tuberculous pneumonia
Less common manifestations include pneumothorax, ARDS, cor pulmonale and localised emphysema.
Clinical features: extrapulmonary disease
Extrapulmonary tuberculosis accounts for about 20% of cases in those who are HIV-negative but is more common in HIV-positive individuals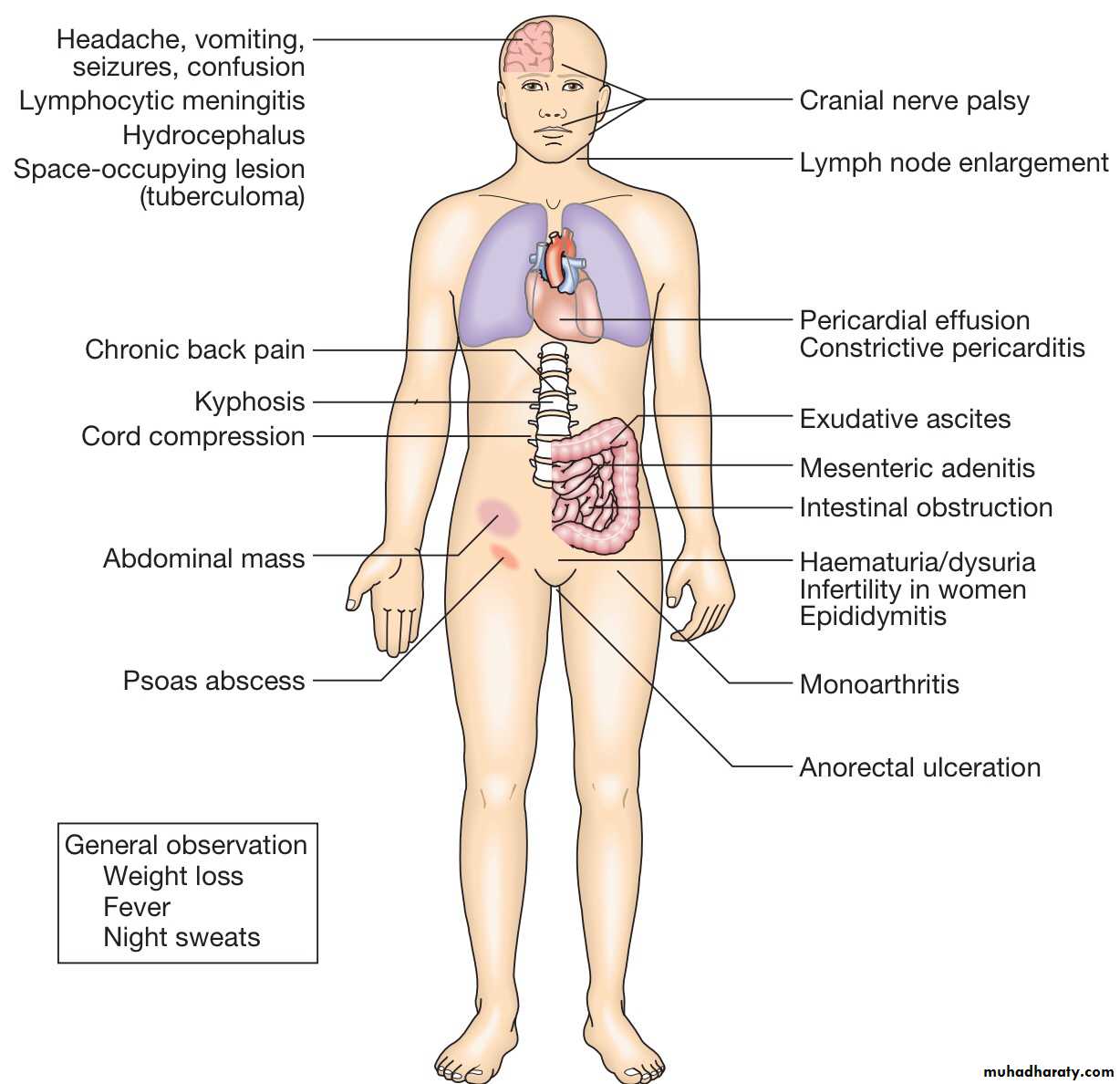
Lymphadenitis
Lymph nodes are the most common extrapulmonary site of disease. Cervical and mediastinal glands are affected most frequently, followed by axillary and inguinal, and more than one region may be involved.Disease may represent primary infection, spread from contiguous sites, or reactivation.
The nodes are usually painless and initially mobile but become matted together with time.
When caseation and liquefaction occur, the swelling becomes fluctuant and may discharge through the skin with the formation of a ‘collar-stud’ abscess and sinus formation.
Half of cases fail to show any constitutional features, such as fevers or night sweats.
The tuberculin test is usually strongly positive.
During or after treatment, paradoxical enlargement, development of new nodes and suppuration may all occur but without evidence of continued infection.
Gastrointestinal tuberculosis
TB can affect any part of the bowel.Upper gastrointestinal tract involvement is rare.
Ileocaecal disease accounts for approximately half of abdominal TB cases.
Fever, night sweats, anorexia and weight loss are usually prominent and a right iliac fossa mass may be palpable.
Up to 30% of cases present with an acute abdomen.
Ultrasound or CT may reveal thickened bowel wall, abdominal lymphadenopathy, mesenteric thickening or ascites.
Barium enema reveal narrowing, shortening and distortion of the bowel, with caecal involvement predominating.
Diagnosis rests on obtaining histology by either colonoscopy or minilaparotomy.
The main differential diagnosis is Crohn's disease.
Tuberculous peritonitis is characterised by abdominal distension, pain and constitutional symptoms.
The ascitic fluid is exudative and cellular, with a predominance of lymphocytes.
Laparoscopy reveals multiple white ‘tubercles’ over the peritoneal and omental surfaces.
Low-grade hepatic dysfunction is common in miliary disease, in which biopsy reveals granulomas.
Patients may be frankly icteric, with a mixed hepatic/cholestatic picture
Pericardial disease
Disease occurs in two forms : pericardial effusion and constrictive pericarditis.Fever and night sweats are rarely prominent and the presentation is usually insidious, with breathlessness and abdominal swelling. Coexistent pulmonary disease is very rare, with the exception of pleural effusion.
Pulsus paradoxus, a raised JVP, hepatomegaly, prominent ascites and peripheral oedema are common to both types.
Pericardial effusion is associated with increased pericardial dullness and a globular enlarged heart on chest X-ray, and pericardial calcification occurs in around 25% of cases.
Constriction is associated with an early third heart sound and, occasionally, atrial fibrillation. Diagnosis is based on the clinical, radiological and echocardiographic findings.
The effusion is frequently blood-stained. Open pericardial biopsy can be performed where there is diagnostic uncertainty.
The addition of corticosteroids to antituberculosis treatment has been shown to help both forms of pericardial disease
Central nervous system disease
Meningeal disease represents the most important form of central nervous system TB. Unrecognised and untreated, it is rapidly fatal
Even when appropriate treatment is prescribed, mortality rates of 30% have been reported, whilst survivors may be left with neurological sequelae.
Bone and joint disease
The spine is the most common site for bony TB (Pott’s disease), which usually presents with chronic back pain and typically involves the lower thoracic and lumbar spine.The infection starts as a discitis and then spreads along the spinal ligaments to involve the adjacent anterior vertebral bodies, causing angulation of the vertebrae with subsequent kyphosis.
Paravertebral and psoas abscess formation is common and the disease may present with a large (cold) abscess in the inguinal region. CT or MRI is valuable in gauging the extent of disease, the amount of cord compression, and the site for needle biopsy or open exploration, if required.
The major differential diagnosis is malignancy, which tends to affect the vertebral body and leave the disc intact. Important complications include spinal instability or cord compression
TB can affect any joint but most frequently involves the hip or knee. Presentation is usually insidious, with pain and swelling; fever and night sweats are uncommon.
Radiological changes are often non-specific but, as disease progresses, reduction in joint space and erosions appear.
Poncet’s arthropathy is an immunologically mediated polyarthritis that usually resolves within 2 months of starting treatment
Genitourinary disease
Fever and night sweats are rare with renal tract TB and patients are often only mildly symptomatic for many years.Haematuria, frequency and dysuria are often present, with sterile pyuria found on urine microscopy and culture.
In women, infertility from endometritis, or pelvic pain and swelling from salpingitis or a tuboovarian abscess occurs occasionally.
In men, genitourinary TB may present as epididymitis or prostatitis