Bronchial Carcinoma
Part 2Management
Surgical resection carries the best hope of long-term survival, but some patients treated with radical radiotherapy and chemotherapy also achieve prolonged remission or cure.Unfortunately, in over 75% of cases, treatment with the aim of cure is not possible, or is inappropriate due to extensive spread or comorbidity.
Radiotherapy and in some cases chemotherapy can relieve distressing symptoms
Surgical treatment
Accurate pre-operative staging, coupled with improvements in surgical and post-operative care, now offers 5-year survival rates of over 75% in stage I disease (N0, tumour confined within visceral pleura) and 55% in stage II disease, which includes resection in patients with ipsilateral peribronchial or hilar node involvementRadiotherapy
Radical radiotherapy can offer long-term survival in selected patients with localised disease in whom comorbidity precludes surgery.
Radical radiotherapy is usually combined with chemotherapy when lymph nodes are involved (stage III).
Highly targeted (stereotactic) radiotherapy may be given in 3–5 treatments for small lesions
The greatest value of radiotherapy is in the palliation of distressing complications, such as superior vena cava obstruction, recurrent haemoptysis, and pain caused by chest wall invasion or by skeletal metastatic deposits.
Obstruction of the trachea and main bronchi can also be relieved temporarily.
Radiotherapy can be used in conjunction with chemotherapy in the treatment of small-cell carcinoma, and is particularly efficient at preventing the development of brain metastases in patients who have had a complete response to chemotherapy.Chemotherapy
The treatment of small-cell carcinoma with combinations of cytotoxic drugs, sometimes in combination with radiotherapy, can increase the median survival from 3 months to well over a year.In general, chemotherapy is less effective in non-small-cell bronchial cancers.
Some non-small-cell lung tumours, particularly adenocarcinomas, carry detectable mutations in the epidermal growth factor receptor (EGFR) gene. Patients with these mutations are particularly responsive to the tyrosine kinase inhibitors gefitinib and Erlotinib.
Nausea and vomiting are common side-effects of chemotherapy and are best treated with 5-HT3 receptor antagonists.
Laser therapy and stenting
Palliation of symptoms caused by major airway obstruction can be achieved in selected patients using bronchoscopic laser treatment to clear tumour tissue and allow re-aeration of collapsed lung.
Endobronchial stents can be used to maintain airway patency in the face of extrinsic compression by malignant nodes
General aspects of management
Multidisciplinary teams, including oncologists, thoracic surgeons, respiratory physicians and specialist nurses.Depression and anxiety may need specific therapy.
The management of non-metastatic endocrine manifestationsManagemen of malignant pleural effusion if present
PrognosisThe overall prognosis in bronchial carcinoma is very poor, with around 70% of patients dying within a year of diagnosis and only 6–8% of patients surviving 5 years after diagnosis.
The best prognosis is with well-differentiated squamous cell tumours that have not metastasised and are amenable to surgical resection.
Secondary tumours of the lung
Blood-borne metastatic deposits in the lungs may be derived from many primary tumours, in particular those of the breast, kidney, uterus, ovary, testes and thyroid.The secondary deposits are usually multiple and bilateral. Often there are no respiratory symptoms and the diagnosis is made on radiological examination.
Endobronchial deposits are uncommon but can cause haemoptysis and lobar collapse.
Lymphatic infiltration may develop in patients with carcinoma of the breast, stomach, bowel, pancreas or bronchus.‘Lymphangitic carcinomatosis’ causes severe and rapidly progressive breathlessness associated with marked hypoxaemia. The chest X-ray shows diffuse pulmonary shadowing radiating from the hilar regions, often associated with septal lines, and CT demonstrates characteristic polygonal thickened interlobular septa. Palliation of breathlessness with opiates may help
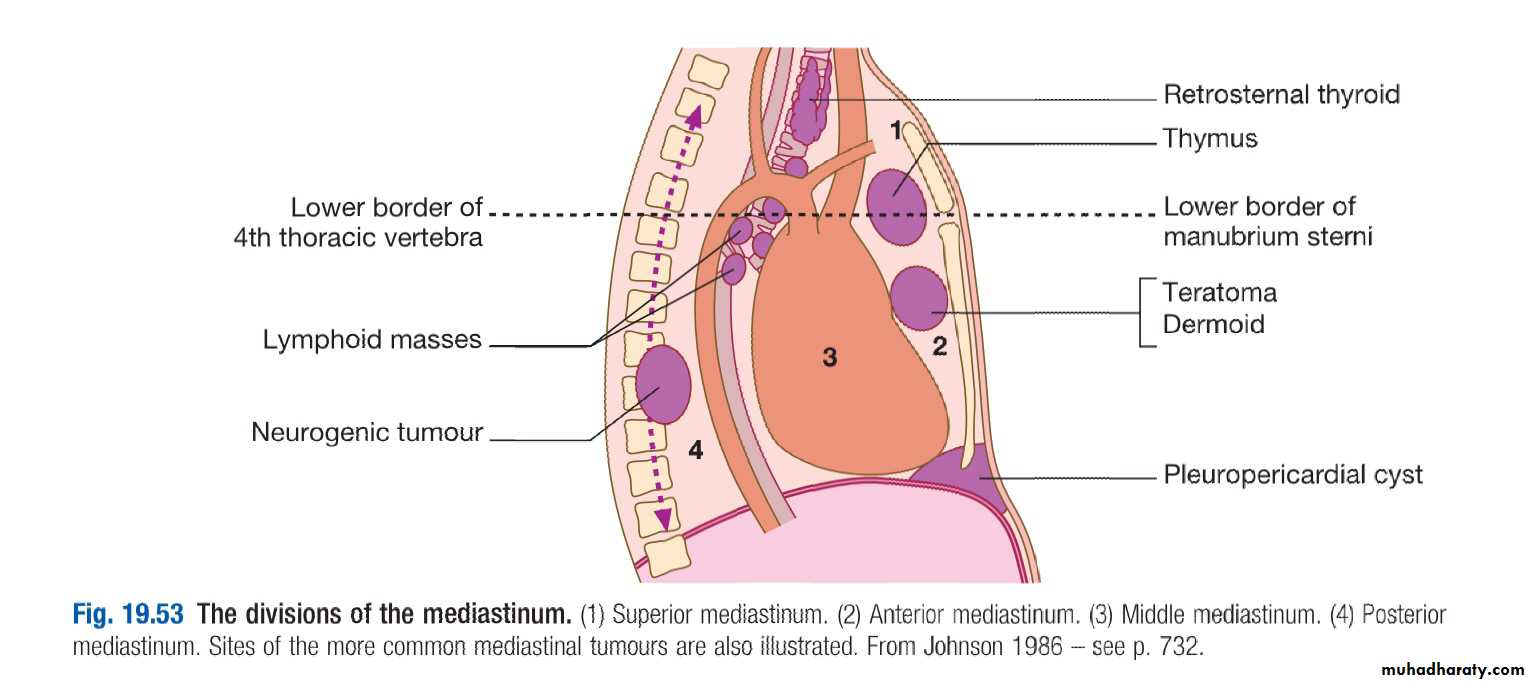
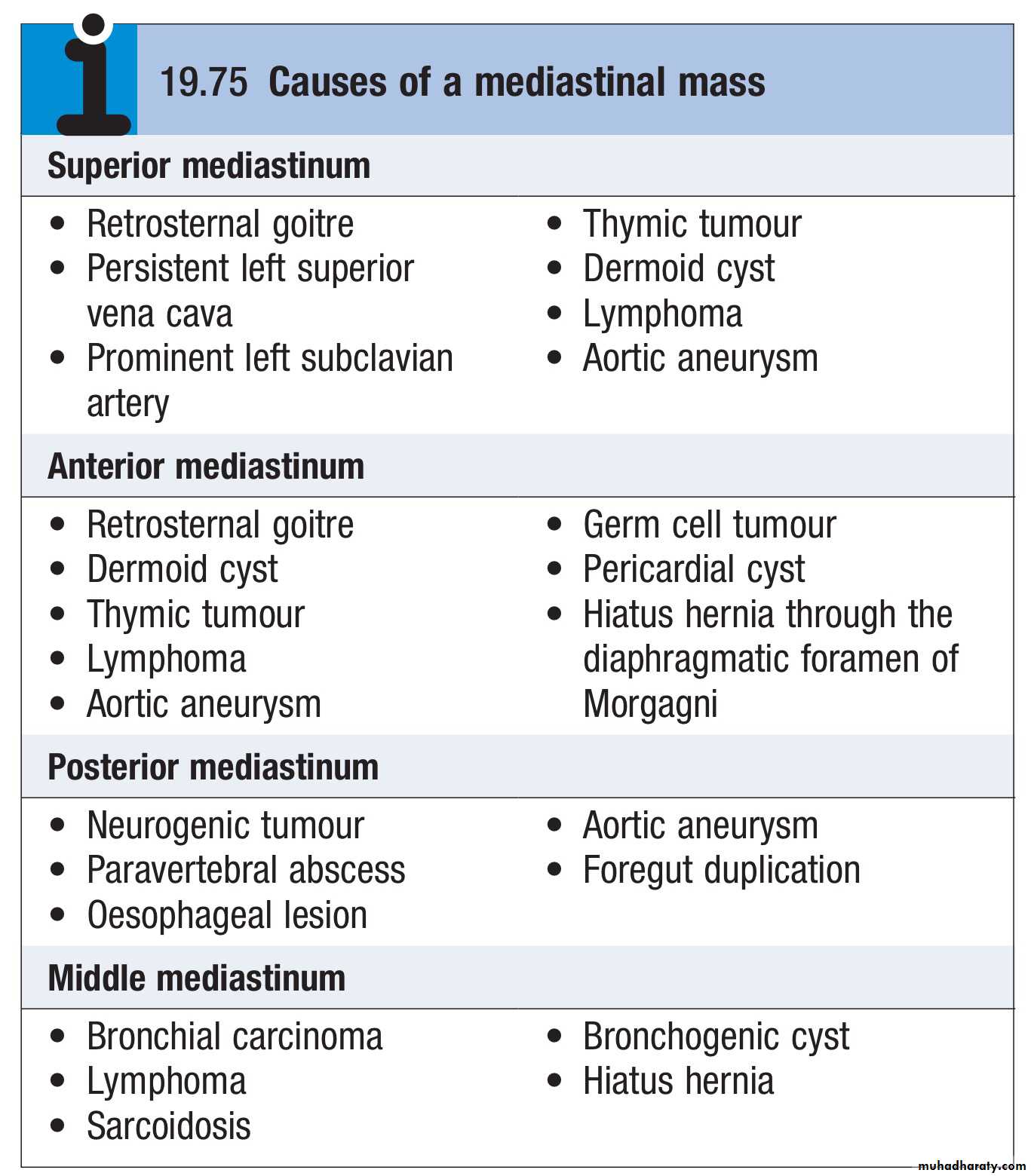
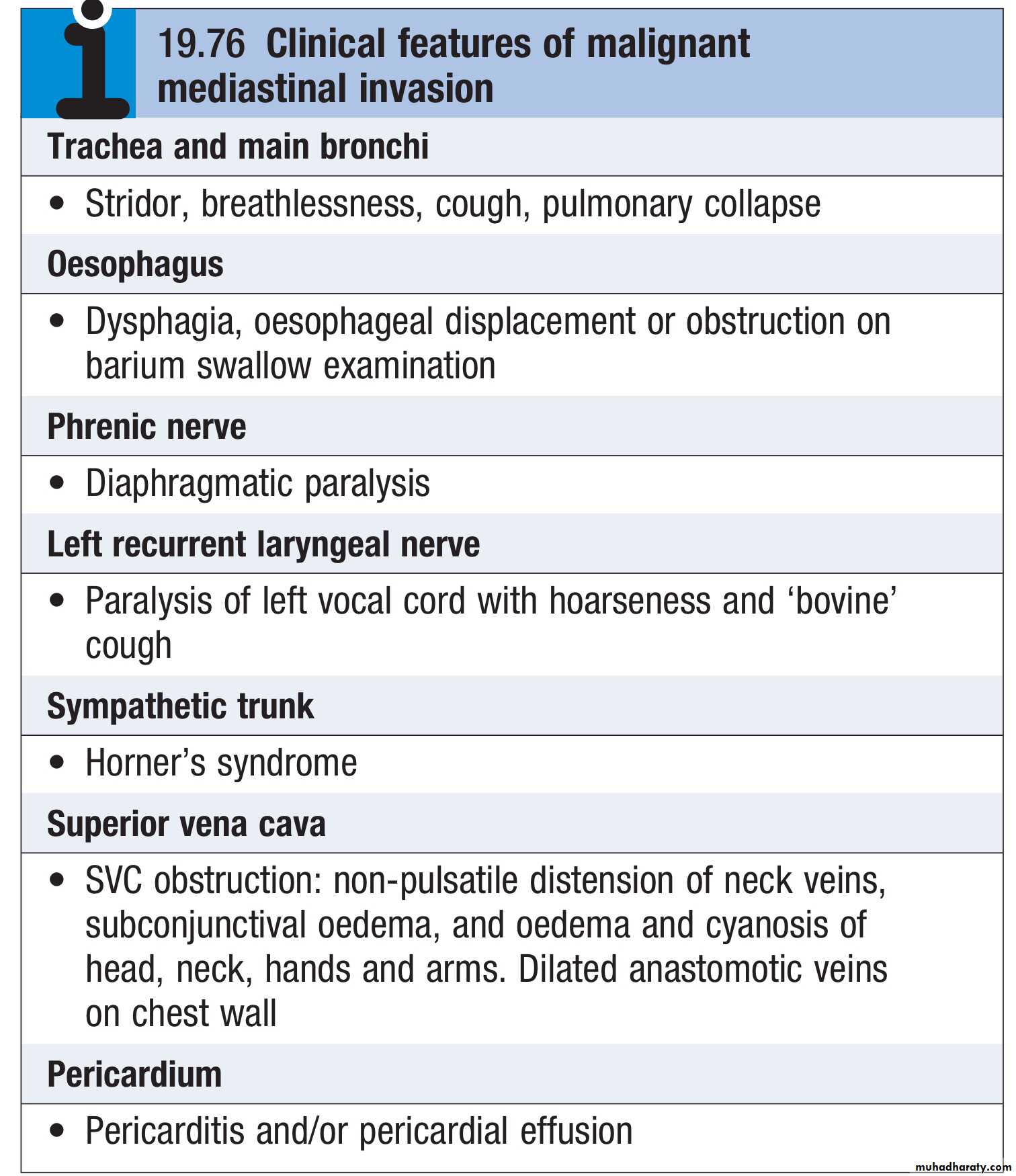
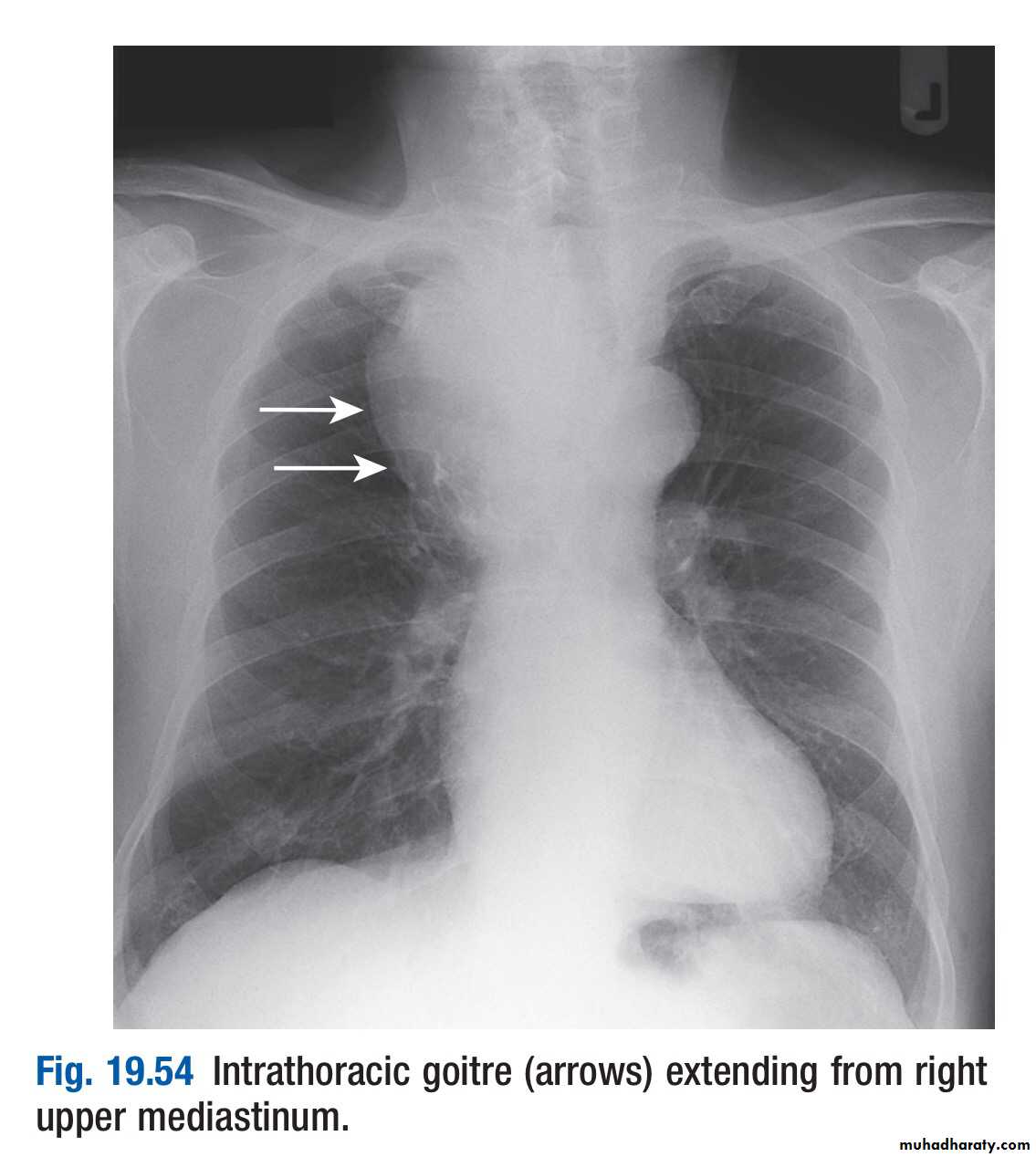
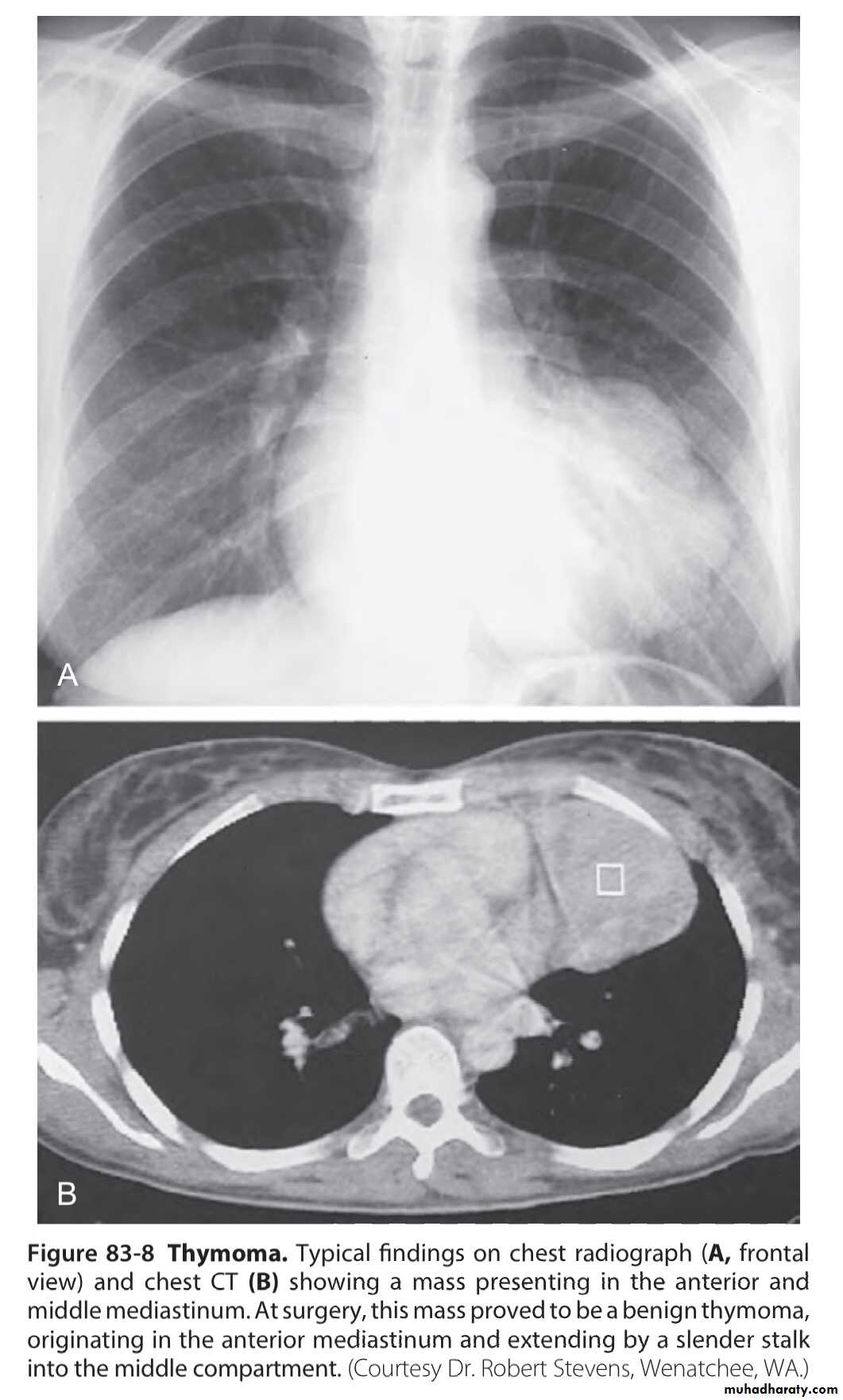
Tumours of the mediastinum