


MANAGEMENT OF DENTAL TRAUMATIC INJURIES IN PAEDIATRIC PATIENTS
DR. LARA
outline
PART 1introduction
Aetiology of traumatic injuries
Epidemiology
Classification of traumatic injuries
Radiographic evaluation
PART 2…Treatment protocols for various dental traumatic injuries in primary and young permanent dentition.
FOLLOW UP
PROGNOSISCOMPLICATION OF TRAUMATIC DENTAL INJURIES
CONCLUSION
introduction
Dental trauma is one of the most common presentation in the paediatrics clinic. The fears and anxiety of these patients make management difficult. If improperly managed, it could affect the patient self-esteem and quality of life
Aetiology
The most accident prone times include;2-4 years for primary dentition
7-10 yrs for permanent dentition
Aetiological factors include;
• Falls
• Playing and running
• Contact sports
• Road traffic accident
• Child abuse; ESPN
Emotional-Sexual-Physical-Neglect
Predisposing factors
• 1. Angle class 11 div 1• 2. Increased overjet;
3-6mm..double the risk
>6mm….triple the risk
3. Incompetent lip closure
4. Improperly fitted mouthguard
.twice the risk


Epidemiology
Dental trauma is common in childhood and adolescence.By 5 yrs; boys-- 31-40%
girls….16-30% and
At 12 years;
12-33% of boys and 4-19% of girls would have suffered dental trauma
boys : girl; 2:1 in both dentitions
In primary dentition;
anterior segment is commonly affected especially the maxillary central incisor,concussion, subluxation, and luxation are the commonest
In permanent dentition;
luxation and fracture injuries are the commonest
Maxillary central incisor>maxillary lateral incisor>mandibular incisor
Andreasen’s classification
• Dental Hard Tissue and Pulp OnlyCrown infraction
Uncomplicated crown
Complicated crown
Uncomplicated crown-root
Complicated crown-root
Root fracture
B. Periodontium
Concussion
Subluxation(loosening)
Luxation
intrusive(central dislocation)
extrusive(peripheral dislocation, partial avulsion)
lateral
Exarticulation(complete luxation/avulsion)
C. Surrounding bone
Comminution of alveolar socketFractures of facial or lingual alveolar socket wall
Fractures of alveolar process -/+ involvement of the socket
Fractures of the mandible or maxilla -/+ involvement of the tooth socket
D. Soft tissue
LacerationContusion
Abrasion
Radiographic evaluation
Indication for radiograph;• To detect root fracture
• Ascertain extent of root development
• To determine resorption
• To detect foreign body in soft tissue
• To detect jaw fracture
• To note position and stage of development of permanent teeth
• To detect size of pulp chamber
• To detect periapical radiolucency
• For follow-up evaluation
TREATMENT OPTIONS FOR DENTAL TRAUMATIC INJURIES
Dental trauma to primary dentition
Most common is subluxation, intrusive luxation and avulsion. Crown and root fracture are rare.
Subluxation
Diagnosis; mobile tooth -/+ sulcular bleedingX-ray; no abnormality
Treatment; clean associated soft tissue injury with 0.2% chlohexidine with gauze swabs twice daily.
Slight mobility; place on soft diet for 2 wks
Marked mobility; extract
Follow-up; after 1 month to assess mobility
Prognosis; usually good

Intrusive luxation
Tooth displace towards the socket, compressing the PDL and crushing the alveolar bone.Diagnosis; not mobile, not tender,
appear shortened or in severe
cases would seem missing

Treatment;
a. if apex is displace labially, allow for spontaneous re-eruptionb. if displaced palatally; extract the tooth
Follow-up; Review should be weekly for a month then monthly for a maximum of 6 months. Most re-eruption occurs between 1 and 6 months and if this does not occur then ankylosis is likely and extraction is necessary to prevent ectopic eruption of the permanent successor
Extrusive luxation
Partial avulsion as PDL is severely torn/damagedDiagnosis; tooth appear elongated and mobile
X-ray; increased PDL space apically
Treatment; mild extrusion<3mm allow tooth to reposition spontaneously and heal if tooth is immature.
when do I need to extract?
• Severe extrusion/mobility
b. Tooth near exfoliation
c. Child not cooperatingd. Tooth fully mature
Follow-up; if repositioned take x-ray to determine reduction in the PDL space apically
Lateral luxation
Tooth displaced in any position other than axiallyDiagnosis; tooth appear displace, not mobile nor tender
X-ray; shows increased PDL
space and displaced tooth
apex.

Treatment; if apex is displace buccally and there is no gagging of occlusion, allow spontaneous realignment.
extract if apex is displaces towards the permanent tooth bud.
prognosis; If tooth is repositioned, there is risk of pulpal necrosis compare to spontaneous eruption.
Avulsion
Diagnosis; Tooth is out of the socketX-ray; do a chest x-ray if tooth can’t be accounted for
Treatment; do not re-implant due to risk of damaging the permanent tooth bud.
Though space maintenance is not necessary, a fixed or removable be fabricated to allaw aesthetic concerns
Follow-up; permanent tooth eruption could be delay for 1-2yrs due to formation of fibrotic band
avulsion

HARD TISSUE INJURIES
Uncomplicated crown fractureEnamel -/+ dentine # without pulpal involvement.
Treatment;
aim is to preserve pulp vitality and restore aesthetics.
small fracture: smoothen rough margins/edges
large fracture:
for large enamel fracture restore with acid-etch-composite resin
Fracture edges can be disked

if dentine is involved;
protect the pulp using acid resistant calcium hydroxide or GIC restore with acid-etch compositeCOMPLICATED CROWN FRACTURE
Is uncommon in primary dentitionDiagnosis; loss of tooth structure with pulp exposure clinically and on radiograph.
Treatment options; Depends on
patients cooperation
vitality of the tooth
stages of root development
formocresol pulpotomy; if tooth is vital
pulpectomy with zinc oxide and eugenol
non-vital tooth
3/4th of the root must be formed.
extraction; if child is uncooperative
tooth is non-vital
Final restoration; depends on amount of tooth structure remaining
composite resin if remnant can support the composite restorationstainless steel crown with composite veneering if small fragment remains
Prognosis; depends on concomitant injury to the PDL.
ROOT FRACTURE;
Diagnosis; mobile coronal segment -/+ displacedRadiograph;
take at least 2 views
reveal radiolucent line b/w fragment
succedaneous tooth could obscure root fragment
Treatment; depends on level of fracture:
at apical 1/3rd and with minimal mobility, observe. Take serial radiograph of the tooth.
Middle 3rd fracture

If the coronal fragment becomes non-vital and symptomatic then it should be removed. The apical portion usually remains vital and undergoes normal resorption.
At the middle and cervical 3rd, tooth should be extracted.
Trauma to young permanent teeth
Prompt and accurate diagnosis is important in the success of treatment.Aims and objective of treatment;
• Emergency/immediate; to
retain vitality of fracture and displaced tooth
treat exposed pulp tissue;
reduction and immobilization of displaced teeth
antiseptic mouthwash, +/- antibiotics and tetanus prophylaxis.
2. Intermediate:
(a) pulp therapy;(b) minimally invasive crown restoration.
3. Permanent:
(a) apexogenesis/apexification;
(b) root filling + root extrusion;
(c) gingival and alveolar collar modification;
(d) permanent coronal restoration.
Hard tissue injuries and management
Enamel infraction;
Incomplete fracture in the enamel
Examination; reveal craze lines on transillumination
Treatment; periodic recalls are necessary.
Uncomplicated crown fracture
Loss of enamel -/+ dentine fracture without pulp involvement.
CLASS I




A fracture confined to the enamel with loss of tooth structure
Enamel fractureA fracture confined to enamel and dentin with loss of tooth structure but not involving the pulp





Enamel-dentin fracture
,Treatment;
for small fracture use fine disk to smoothen the margins
for larger loss, protect the pulp with calcium hydroxide or GIC then restore with acid-etch composite.
Enamel and dentine bonding agents have also been used to protect the pulp from thermal irritants and bacterial ingress.
Complicated crown fracture;
Factors that influence choice of treatment:vitality of expose pulp
time elapse since the exposure
degree of root maturation of the fracture tooth
restorability of the fracture crown
Aim of treatment; to preserve pulp vitality
• A fracture involving enamel and dentin with loss of tooth structure and exposure of the pulp





Enamel-dentin-pulp fracture
• Types of coronal fracture• Most frequent injury
•



enamel only
enamel and dentine
enamel and dentine
with the pulp exposedTreatment options;
direct pulp capping(DPC)pulpotomy; partial or complete
pulpectomy
carry out DPC ;
when exposure is pin-point
when exposure is just of few hours>24hrs
when the apex is open
as an emergency measure even pulpotomy is to be done
When to do pulpotomy:
pulpal exposure for longer hours >24hrslarger pulpal exposure
immature open apices
Aim of treatment; to eliminate inflamed pulp tissue and preserve vital radicular pulp aiding complete root development(apexogenesis)
Vital(full) pulpotomy or partial pulpotomy could be done depending on the level of inflammation and extent of bleeding on amputation
Follow-up
Review after a month, 3 months, 6 monthly intervals for up to 4 years to assess pulp vitality.Do periodic radiograph.
If vitality is lost, non-vital pulp therapy should be undertaken whether or not there is a calcific bridge
Prognosis;
success rates for partial pulpotomies are quoted at 97%. Those for coronal pulpotomies at 75%.
Pulpectomy as an option; done
in non-vital pulppulp with open apex.
an apical root end closure(apexification) is done, but dentinal wall is left fragile and easily fracture
Follow-up;
first month, then 3 mths, then 6 mthsDo periodic radiograph to check evidence of calcific barrier formation. This will normally take b/w 9-24 mths
final treatment; these include
Definitive canal obturation
composite restoration
porcelain veneer and crown
post-retained crown
Closed apex
Open apex
RCT
Vital tooth
Non-vital tooth
Direct Pulp Capping
Pulpotomy
Apexification
Treatment summary for Complicated crown fracture;
Non-vital tooth
Root fracture.Diagnosis; clinically mobile teeth and 1 or more radiolucent lines separating fracture segments
Aims of treatment;
to reposition and stabilise coronal segment
encourage healing of PDL and vascular supply
to restore aesthetics and function
Treatment;
reposition segment and immobilise for 2-3mths (preferably fixed splint composite resin)
• Fracture radical part of tooth.
• cervical third
• middle third
• apical third
•

Decision to splint;
this depend on the level of fracture and whether long term stability of the tooth depends on itApical 1/3rd fracture; no need to splint except there is an associated subluxation. The child should be kept under observation, somtimes the fractured part reattached with the root by overlay new layer of cementum.
• Middle and cervical 1/3rd;
• splint if tooth is to be retained.• If coronal segment is extracted for cervical fracture, root portion is extruded surgically or via orthodontic mean and pulp therapy done. A post-retained crown is planned
• Both fragments could be extracted and prosthesis planned.
• follow-up assess pulp vitality
assess stability of tooth
Prognosis
this is best for apical 3rd fracturebecomes poorer in middle and cervical fracture
Luxation injuries in permanent dentition
This involve damage to supporting structures of the teeth i.e PDL and alveolar bone.
Primary objective is to maintain vitality of the PDL which is important in the long term prognosis of the luxated teeth.
CONCUSSION
Diagnosis; tooth is firm, tender to pressure and percussionRadiograph; usually no abnormality.
Treatment; soft diet for 2wks, relieve it from occlusion if there is complain of pain
Follow-up; vitality test for 1, 3 and 6 month then yearly. Radiograph to assess root development
Prognosis; usually good, but necrosis in 3-6% of cases
Subluxation
Diagnosis; tooth is mobile. Bleeding at the marginal gingival, tender to percussionRadiology; the PDL space is widened.
Treatment; stabilize and relieve from occlusion. For comfort use flexible splint(<2wks) if apex is fully formed and extremely tender.

Prognosis;
mature teeth with closed apices are at risk of pulpal necrosis hence, close monitoring is required.LATERAL LUXATION
Diagnosis;
tooth is displacedcrown may be palatal or labially
displaced ;
not mobile nor tender
Radiology; PDL space is increased
and the apex is displaced
labially or palatally

Note labially displaced crown

Treatment;
reposition tooth with gentle and firm digital pressureuse flexible splint 6-8wks
place on antibiotics and TT(if indicated)
use 0.12% chlohexidine mouth wash
Follow-up; do periodic radiograph to monitor DPL re-attachment.
Prognosis; tooth with closed apices could become necrotic(start root canal trt) and have the canal obliterated
INTRUSIVE LUXATION
Diagnosis; teeth appear shortened, or in severe cases could appear missing, not mobile nor tender
Radiograph; root apex is displaced
apically PDL space is non-continuous

Treatment; depends on:
1. stage of root development: open or close2. severity of injury; mild <3 mm, moderate (3-6 mm); or severe (>6 mm).
OPEN APEX ;
If the crowns remain visible, it may be allowed to re-erupt spontaneously for 2-4 months, but if not re-erupt then disimpact and surgically reposition. Functional splint for 7-10 days is needed.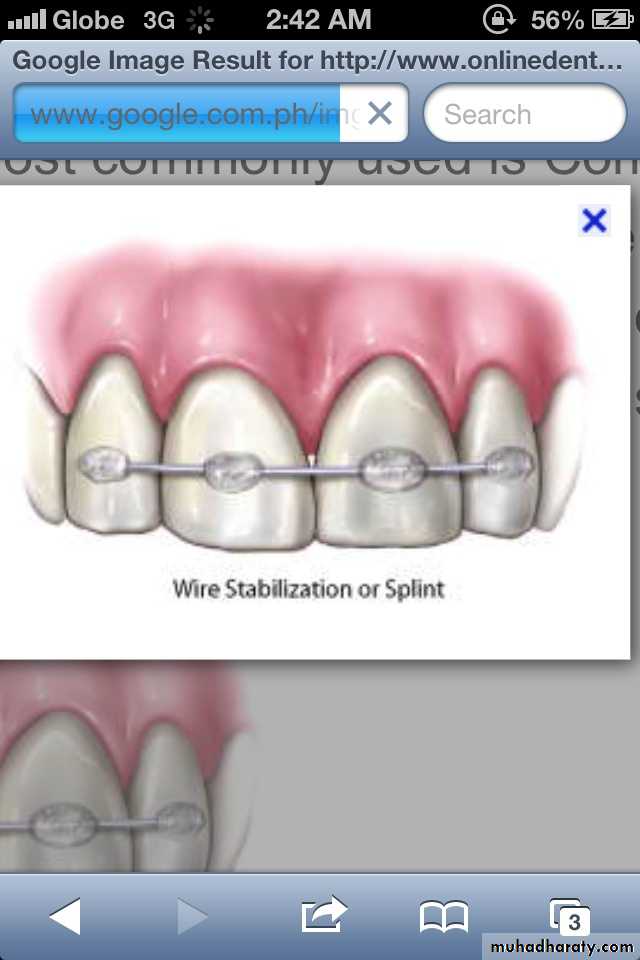
Follow-up.
Monitor pulpal status clinically and radiographically at regular intervals during the first 6 months after injury, and then 6 monthly, and start endodontics if necessary:Non-setting calcium hydroxide in root canal should be used, once apexification has occured obturate canal with gutta percha.
CLOSED APEX ;.
immediate repositioning (Orthodontic/ surgical extrusion) is probably indicated for mature teeth. Functional splint for 7-10 days after surgical extrusion. Followed by non-setting calcium hydroxide in root canal during orthodontic tooth movement before obturation with gutta percha.Partially intruded with ortho disimpaction

Prognosis;
mature closed apex have higher risk of pulp necrosis(96%), root resorption and ankylosisimmature apex have 60% risk of necrosis and resorption
teeth treated early enough have better prognosis
EXTRUSIVE LUXATION
Tooth displace axially from the socketDiagnosis; clinically appear longer and is mobile
On radiograph; PDL space is increased apically
treatment; reposition tooth with gentle and firm digital pressure
splint for 2wks
Follow-up; closed apex are at risk of necrosis hence, pulp therapy is indicated after splinting
Note teeth appearing longer

AVULSION/EXARTICULATION
As a rule all avulsed teeth should be re-implant.Diagnosis; clinically and radiological evidence show absence of tooth in the socket in case complete intrusion is been suspected.
Management;
• Give first aid if you receive a phone call
avulsion

First aid for avulsed tooth
1. Do not touch the root of the tooth. Handle the tooth by the crown only.2. Rinse the tooth off only if there is dirt covering it. Do not scrub or scrape the tooth.
3. Attempt to reimplant the tooth into the socket with gentle pressure, and hold it in position.
4. If unable to reimplant the tooth, place it in a protective transport solution, such as Hank's solution, milk or saline.
This will hydrate and nourish the periodontal ligament cells which are still attached to the root.
small container of Hank's Balanced Salt Solution can be purchased in dental emergency kit form at many drug stores.
Contact lens solution is not an acceptable storage medium.
5. The tooth should not be wrapped in tissue or cloth. The tooth should never be allowed to dry.
6. Take the child to a dentist or hospital emergency room for evaluation and treatment.
7. Radiographs may need to be taken of the airway, stomach, and mouth if the tooth cannot be found .
8. Tetanus prophylaxis should be considered if the dental socket is contaminated with debris.
treatment
Considerations;1. Extra-oral time
2. Stage of root development

Open Apex:
If the extra-oral dry time is <60 minutes, may undergo pulp revascularization.. If the extra -oral dry time is >60 minutes, endodontic treatment is required.
Apply a flexible, functional splint for 7 to 10 days.
If an alveolar fracture is present, provide a very rigid splint for 4-6 weeks.
Intracanal dressing (antibiotic/sdteroid) ledermix paste
Subsequent non-setiing calciuum hydroxide.
No progressive resorption, obturate with guttapercha.
Canal obturation with gutta percha and the tooth reimplanted and splinted rigidly for 6 weeks, the aim of this treatment is to produce ankylosis allowing the tooth to be maintained as a space maintainer.
Closed Apex:
suture any laceration
place on antibiotics and analgesicsprescribe 0.12% chlohexidine mouthwash
check TT status
Complication of traumatic dental injuries
In primary dentition;Pulpitis; reversible or irreversible
Pulp canal obliteration
Pulp necrosis
root Resorption
Injury to developing permanent teeth; hypoplasia, hypomineralisation, crown dilacerations, arrested root development, odontoma-like formation
conclusion
Trauma dental injuries is common among toddlers and adolescence. Due to the instability of children in their developmental stage they become prone to it. Mouth guard use in contact sport can greatly reduce the incidence and severity.Effort should be made if possible to preserve a traumatise tooth considering the aesthetics and functional role they play.