


Class II Malocclusion
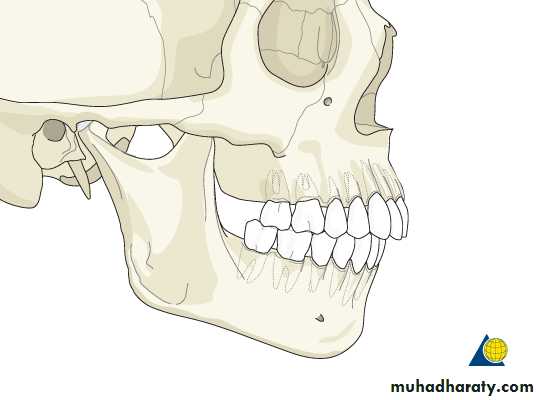
In sagittal plane this malocclusion is called as postnormal occlusion or distoclusion.According to Angles classification indicates that mandibular arch is in a distal relation to that of the maxilla.
The mesiobuccal cusp of the maxillary first molar occlude more than one half cusp width anterior to mesiobuccal groove of the mandibular first molar.

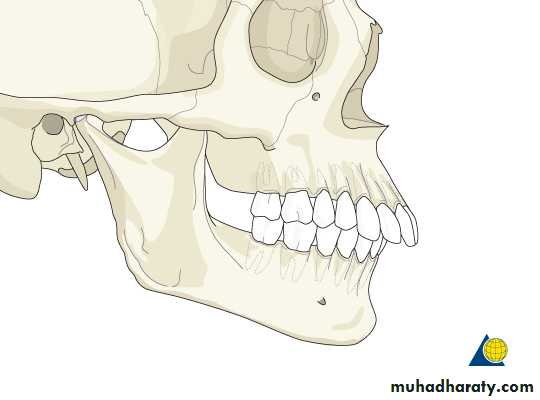
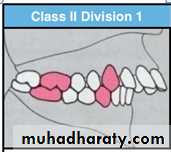
Class II division 1 : The molar relationship in class II with the upper anterior teeth proclined.
Subdivisions of Class II Malocclusion

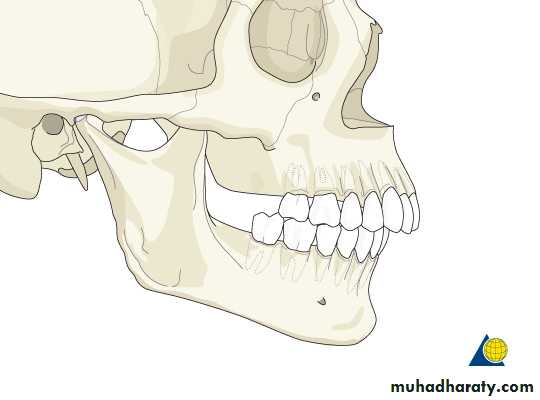
Class II division 2: The molar relationship in class II with the upper central incisor are retroclined and overlapped by the lateral incisors.
In more sever cases both upper central and lateral incisors are retroclined and overlapped by canines.
Subdivisions of Class II malocclusion


2- skeletal class II malocclusion:
1- maxillary protrusion.2- mandibular retrusion.
3- combination of above.
Classification of Class II malocclusion
1- Dentoalveolar Class II malocclusion:
Normal maxillo-mandibular skeletal relation but the defect in alveolar bone or dentition
Mandibular Retrognathisim
Maxillary prognathisimMaxillary dento-alveolar protrusion
Class II Division 1 malocclusion
Etiology
1- skeletal genetic componentPrognathic maxilla
Retrognathic mandible
Combination of above
2- soft tissue factor
Incompetent lips (proclined upper incisors)Lower lip trap behind upper incisors
Tongue thrust
3- habits
Digit sucking habit (proclination of upper incisor, retroclination of lower incisor, anterior open bite)Mouth breathing habit
Features of class II division 1 malocclusion:
Extraoral features1- Convex profile.
2- Posteriorly divegent face
3- Deep mentolabial sulcus
4- Oval shaped face (mesocephalic to dolichocephalic in frontal view.
5- Incompitant lips.
6- Short hypotonic upper lip.
7- Everted lower lip.
8- Hyperactive mentalis muscle.
9- Abnormal perioral musculature.
10- Deficient lower facial height.
11- Lip trap (sometimes).



Intraoral features:
1- Class II molar relationship2- Class II incisor and canine relationship
3- Increased overjet
4- Narrow V shaped upper arch
5- Deep palate
6- Over eruption of lower incisor
7- Deep bite may be traumatic
8- Exaggerated curve of spee
9- Other features may be seen like posterior cross bites or open bites


Management of class II division 1 malocclusion
Treatment is depend on:1- patient age.
2- severity of malocclusion.
3- patient facial profile.
4- etiology of malocclusion.
There are three approach for the treatment of class II malocclusion:
1- Prevent malocclusion from occurrence.2- Intercept the developing malocclusion.
3- Correct an already existing malocclusion.Timing of the treatment is an important factor in the amount of changes that can be produced.
Optimum time for growth modification is prepubertal growth spurt.
Therefore proper diagnosis of the patient at early age and the use of correct functional appliances will cause the patient to avoid surgery.Management of functional disturbances:
Mouth breathing – habit breaking appliancesAbnormal tongue position and swallowing patterns – fixed or removable habit breaking appliances
Lip posture and activity – lip exerciser
Finger sucking habit - fixed or removable habit breaking appliances
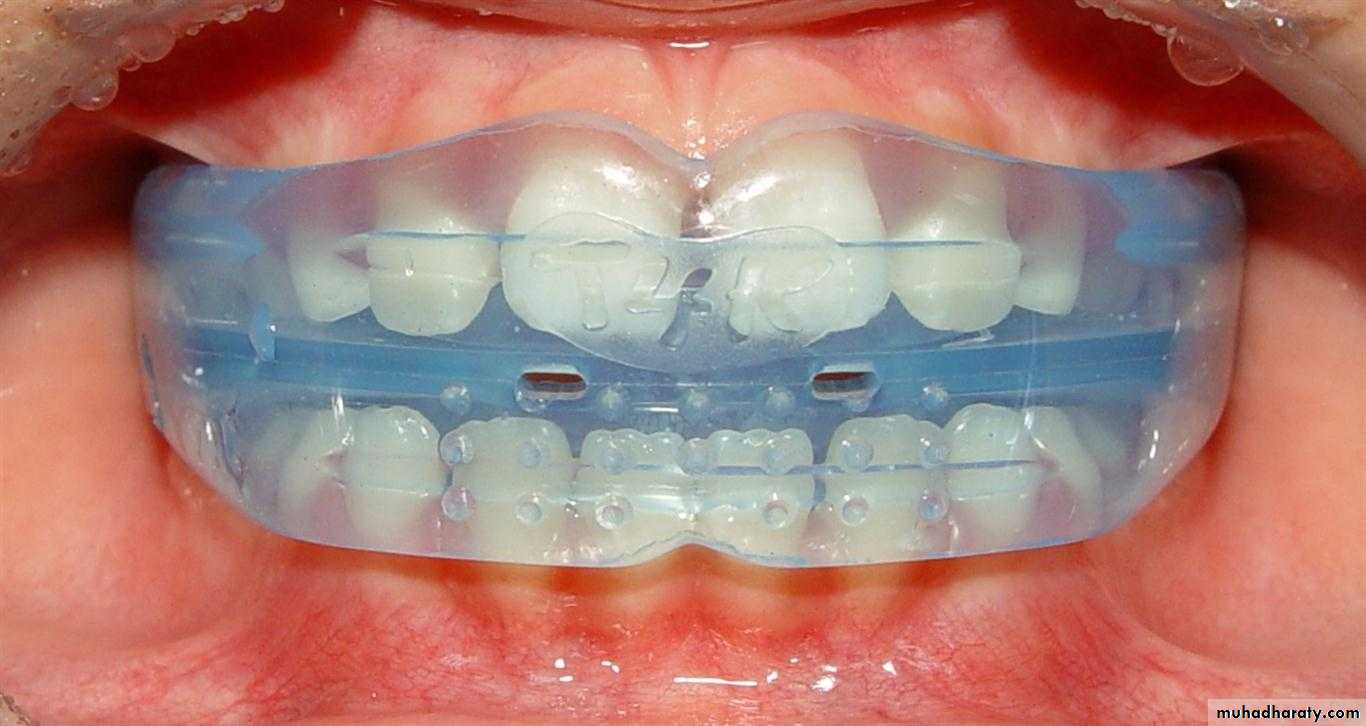

functional appliances is indicated for growth modification in growing patients.
Mild to moderate class II division 1Proclined upper incisors
No lower and upper arch crowding
Deep overbite
Average or reduced lower facial height

Skeletal Class II In growing patient:
Mixed dentition period (modifying growth)Prognathic maxilla – headgears
Retrognathic mandible – activator, frankle and other bite jumping devices








Dentoalveolar class II is treated with:
Removable appliances – robert retractorFixed appliances
Indication of removable appliances (Robert retrector)1- Proclined upper incisors
2- Spaced upper incisors3- Normal or reduced overbite

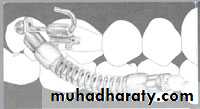
3- fixed appliances
Indicated for most complicated tooth movements which involve bodily tooth movement, intrusion, extrusionUse class II elastics

Skeletal class II
Dentoskeletal compensation for the skeletal defect through reduction of tooth material is the treatment of choice ( camouflaging).Generally maxillary first premolars are extracted.
Indicated in adults with no growth potential
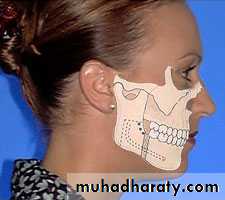
mandibular advancement
Indication : skeletal class II caces with mandibular deficiency
The intraoral sagittal split ramus osteotomy is the popular technique for surgical mandibular advancement.
Orthognathic surgery
Maxillary impaction (Le Fort 1 maxillary osteotomy)
Indication : Vertical maxillary excessAnterior maxillary sub-apical set back
Indication : maxillary excess in antero-posterior dimentional mid-face protrusion ( no vertical excess)Orthognathic surgery
Combined surgical approaches : maxillary and mandibular
Indication : maxillary excess and mandibular deficiencyOrthognathic surgery
For overjet reduction to be stable , anterior lip seal must be achieved, lower lip contact the upper incisor
Appliances used for retention
1- lingual fixed retainer2- Howly labial arch
Retention and stability


