
Dr. Monia MN Kandil
Alveolar Ridge AtrophyA diminution in the size of a cell, tissues of the organ, it may be evident in both external form and internal structures.
Atrophy of the alveolar ridge is irreversible process.
Definition:Anatomic factors Metabolic factors
Functional factors Prosthetic factorsEtiology
The Atrophic (Flat) Mandibular RidgeFlat palate with shallow vestibule

• Anatomic factors
• Include type of the bone, size, shape, and density of the ridges.• The thickness and character of the mucosa covering the ridge.
• The ridge relationships.
Type of bone
Cortical bone will resorb of bone slower than cancellous bone.Well formed broad ridge will show less resorption than narrow thin ridge because there is more bone to be resorbed per unit of time and the less force received per unit area.
Size and shape of the ridge
Density of the bone
The denser the bone the slower the rate of resorption because there is more bone to be resorbed per unit of time.The reduction of the lower ridge (anteriorly) approximately four times as greater as of the upper ridge.
Pronounced resorption in patient with marked mandibular base bend and less in patient with flattened mandibular base.
Ridge relationship
Biologic & Metabolic factors
Include all of the multiple nutritional, hormonal, and other metabolic factors which influence the cellular activity of the bone forming cells (osteoplast) and the bone resorbing cells (osteoclast).
Age, sex, and general health, such: blood dyscrasis or DM.
Treatment for certain diseases, by radiation therapy or hormonal drugs.Loss of teeth as result of periodontal problems, lead to more amount of RRR.
Functional factorsInclude the frequency ,intensity ,duration ,and direction of forces applied to the bone which are translated into cellular activity, resulting in either bone formation or bone resorption depending on the patient individual resistance to these forces.
For example patient with history of bruxism show significant bone loss.
Also if there is not sufficient interocclusal distance the frequency and duration of forces on the residual ridge may be increased to a pathologic degree .
Prosthetic factors
Include the techniques, materials, concepts, principles and practices which are incorporated in the prosthesis.For example:
Functional closed mouth impression versus mucostatic impression.Porcelain teeth versus acrylic teeth.
Cusped teeth versus flat teeth.
Wide teeth versus narrow teeth.
Teeth setup over the ridge versus natural placement.
Flat plane versus curved planes.
Balance in all position versus balance in centric position only.
For patients with previous RPD, it also related to:
• Long-term wearing of dentures without serviceability.
• Improperly constructed dentures with improper vertical dimension of occlusion, centric relation, non-balanced occlusion and incomplete coverage of basal seat area.
• Continuous wearing of the dentures without rest to the underlying tissues.
• Porcelain teeth and/or anatomic teeth with high cusp angles transmit more force to the underlying ridge.
The clinical problems
Functional ProblemsInstability
The inability of the residual ridge and its overlying tissues to withstand masticatory forces.
The Mucosa Overlying The Atrophic Mandibular Ridge Influences A Patient's Ability To Withstand Loading. The mucosa is sandwiched between the denture base and the underlying bone so that all the forces generated by the mandible, during function and parafunction, are transmitted through this atrophic tissue.
• The mental foramen occupies a more superior position.
• The shallow sulci adversely influence peripheral seal.
• The mental foramen occupies a more superior position.

• The shallow sulci adversely influence peripheral seal and in turn affects retention.
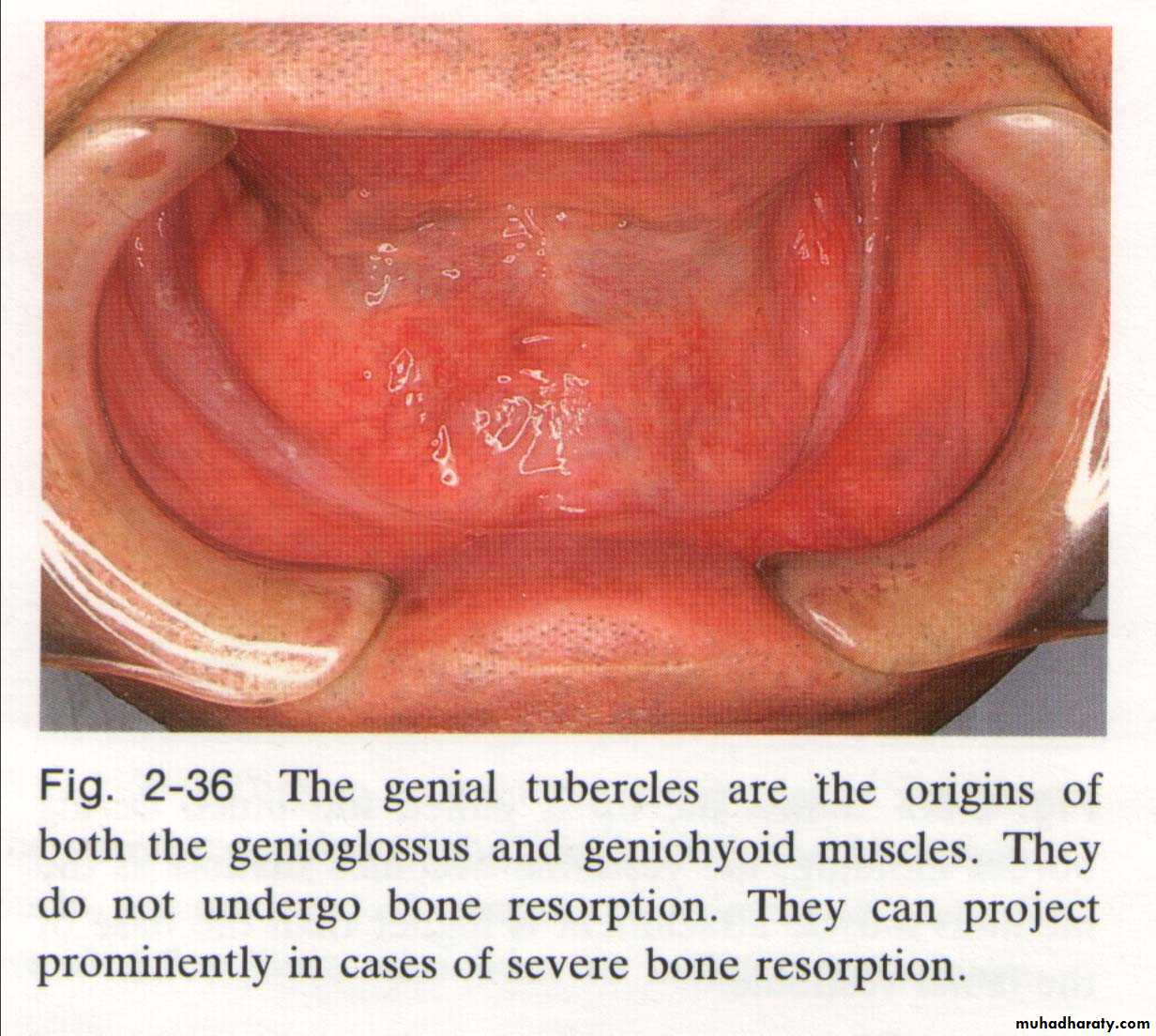
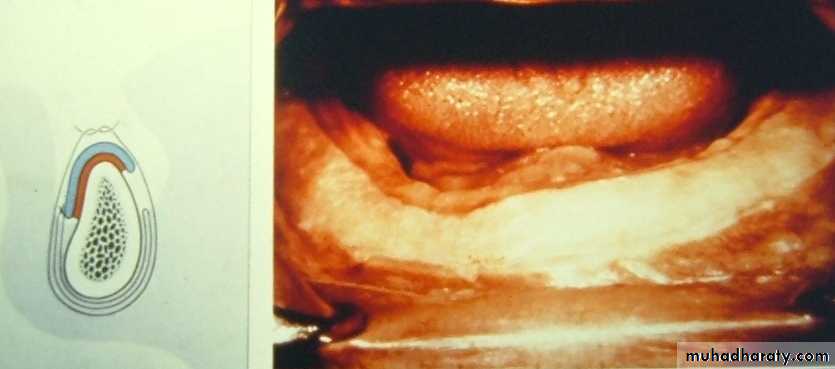
The genial tubercles
are the origins of both genioglossus and geniohyoid muscles, they do not undergo bone resorption. They can project prominently in cases of severe bone resorption.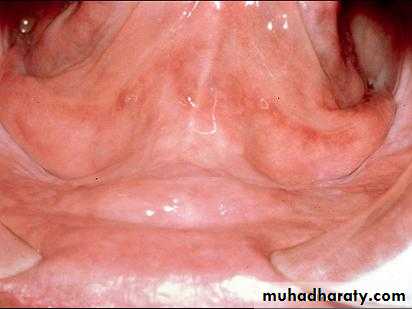
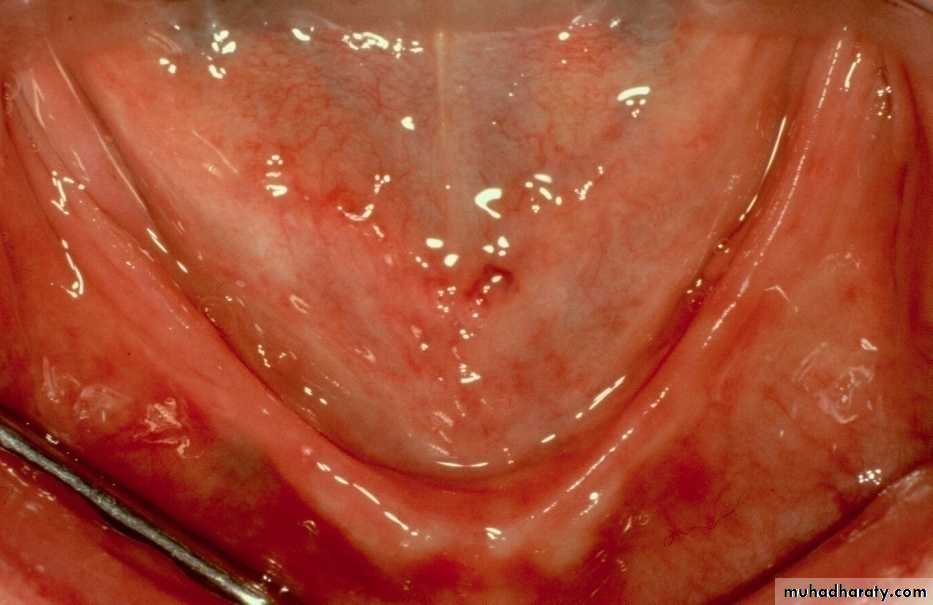
Advanced resorbed ridge with projecting sublingual glands.
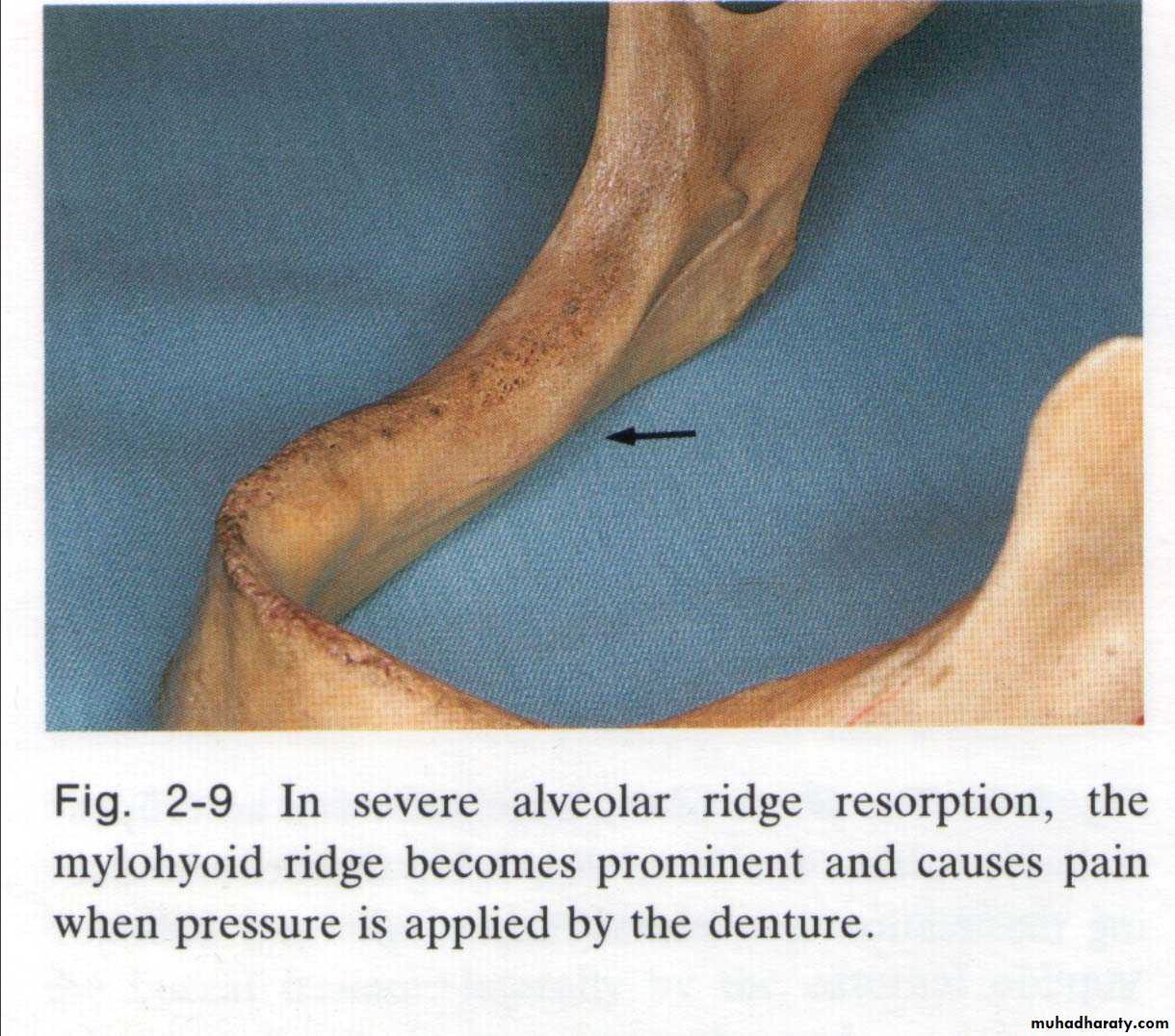
In severe alveolar ridge resorption, the mylohyoid ridge becomes prominent and cause pain when pressure is applied by the denture.
Managements:
Surgical interventions• Vestibuloplasty.
Trimming mylohyoid ridge.
Remove genial tubercle.
• Bone grafting.
• Distraction implants.
• Osseo integrated implants.
Special techniques during impression registration; such as: Muco -compressive, Butterfly, Functional impression technique, and others.
• Jaw relation, esp. considerations.
• Teeth setup, esp. considerations.
Prosthodontic interventions
Surgical Interventions
It is a surgical procedure designed to restore alveolar height and/or width by detachment of buccal or labial tissues from lingual tissues. These tissues are positioned at a level that obtain maximum height of the residual alveolar ridge.I. Vestibuloplasty

Vestibuloplasty can be achieved by:
Mucosal advancement vestibuloplasty “submucous resection”Vestibuloplasty with secondary epithelization
Vestibuloplasty with epithelial grafta. Mucosal advancement
The sub epithelial CT, mucosa and muscle insertion are undermined & separated from the periosteum then advanced to line both sides of the vestibule & hold in its new position by an overextended border of a carefully made surgical stent.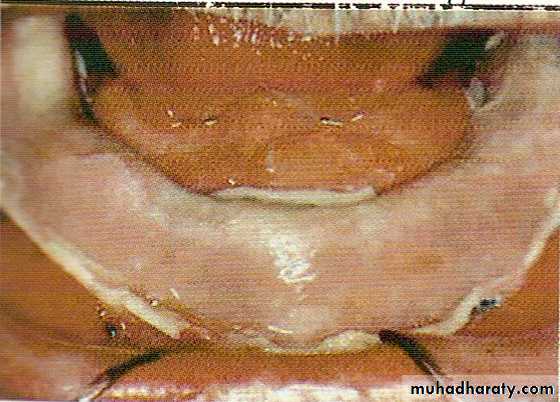
b. Secondary epithelization
An apically repositioned flap is sutured to the periosteum at one side of the vestibule, the other side let to be heals with secondary epitheliztion (this may take long time may be 2 years).A surgical stent lined with tissue conditioning material is helpful in retaining the flap in position and promoting rapid healing.
Vestibuloplasty








c. Vestibuloplasty with epithelial grafts
Similar to the secondary epithelization procedure except that the denuded tissue is covered with a free epithlial graft:
Skin (which is better for bearing the denture).
Buccal or palatal mucosa so is not left to heal by secondary intention.



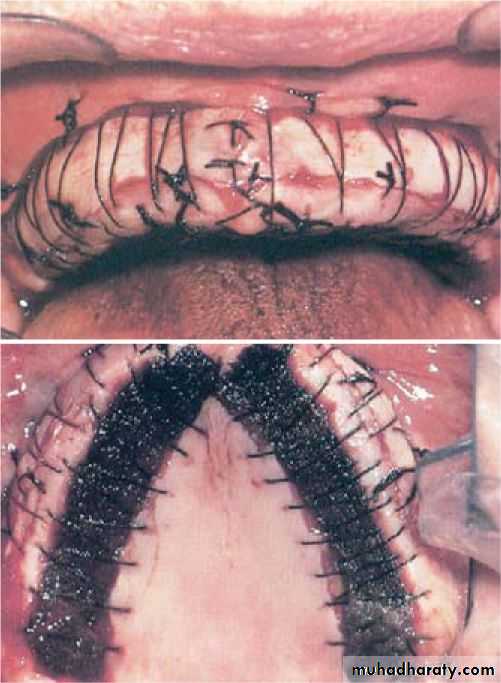
Vestibuloplasty With Split-Thickness Skin Grafting
A combination of split-thickness skin grafting with the vestibuloplasty procedure provides greater patient comfort and better stability.Full-thickness skin grafts include the entire dermis and hair follicles, sweat and sebaceous glands.
Partial-thickness grafts are further classified into thin, intermediate and thick grafts.
The skin graft was harvested from the lateral aspect of the patients thigh. The donor site was covered with an adhesive dressing for patient comfort and infection prophylaxis. The skin graft was then placed and secured with a dermal in a relined, previously constructed acrylic splint.
Vestibuloplasty With Split-Thickness Skin Grafting
II. Trimming mylohyoid ridge
To allow extension of the lingual flange of mandibular denture.
III. Removal of genial tubercle
• To allow extension in the sublingual fold space.
IV. Bone Grafting
Ridge augmentationSinus lift and graft procedure
Nerve repositioninga. Ridge augmentation
In sever cases of ridge resorptionBone graft is placed to increase the ridge height and \or width




b. Sinus lift and graft procedure
This procedure involves elevating the sinus membrane and placing the bone graft onto the sinus floor allowing implant to be placed in the back part of upper jaw.c. Nerve repositioning
• The mandibular nerve may need to be moved in order to make room for placement of dental implant in the lower jaw.
Sources of Bone Grafts:
1- Auto genus materials:A- Intraoral
Chin ,third molar region
B –Extra oral
Hip, outer aspect of the tibia at the knee, iliac crest or rib
2- Allograft material:
Derived from cadaver bone of the same species.3- Alloplastic materials:
Derived from synthetic sources.
4 –Xenografts:
Derived from the inorganic portion of animal bone.
Classification of bone based on source, form & composition:
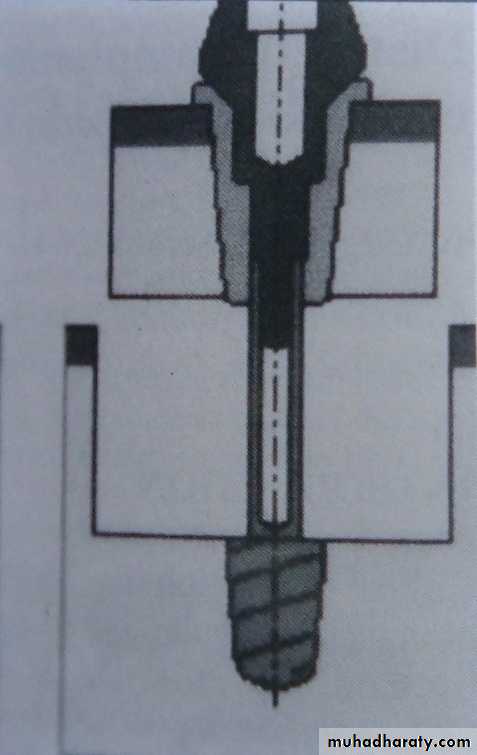
V. Distraction implants
it contains mobile endosteal part that allows heightening of the ridge up to 6 mm. the prosthesis is loaded 4-6 months after distraction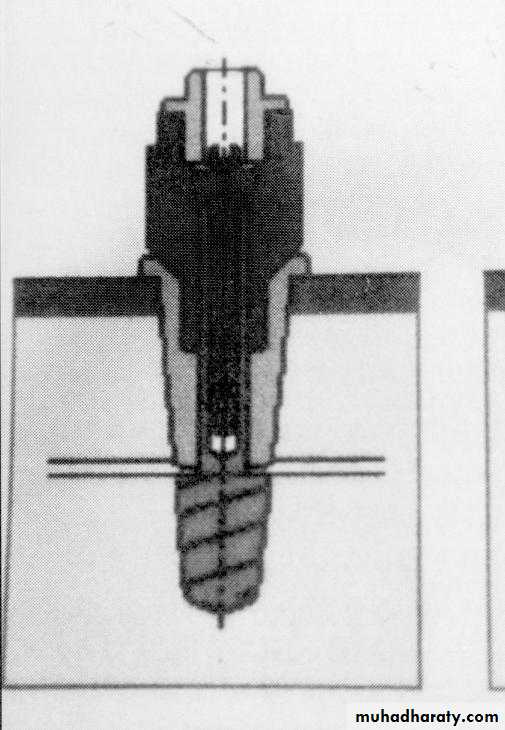


VI. Osseo-integrated implants
Placement of 2 or more of implants in the area anterior to the mental foraminae, increase the horizontal stability and retention of the prosthesis.It can be used with or without bone augmentation.

Prosthetic Management
Without Surgical InterventionHow To Overcome The Problems
The primary consideration for a continued success of the denture isProper diagnosis and full use of every factor, which favor success for this denture,
Maximum base extension within functional anatomical limits (distributed forces over the largest possible area of supporting structures and the force per unit area kept at minimum.)
Reduction of the forces to which the denture is subject
• The polished surface: The creation of the correct form of the polished surfaces,
• The fitting surface: Good impressions that yield an accurate fit spreading the bite load out over the entire ridge.• The border Extension: Proper denture border lengths that allow for free movement of musculature and tissue attachments.
• Tooth Position:
• Molars that are placed proximate to the center of the ridge so as not to create a teeter totter action when chewing.• Correct vertical placement of teeth. Teeth that are placed too high off a lower ridge will create more leverage to rock the denture.
• Occlusion:
• A reduced occlusal table,• An appropriate vertical dimension and
• A balanced occlusion and free articulation creating an uniform application of bite force down on to your ridge.
• Overdenture on implants:
• These may be the only solution for some patients when the first five components have been met and the patient still struggles with retention.
Impression Making
• An ideal impression should provide:
• Maximum extension without muscle impingement.
• Intimate contact with the tissue area covered.
• Proper form of the borders including the posterior border of the maxillary denture.
• Proper relief of hard and sensitive areas.
Impression Techniques
• Primary impressions• Conventional prim. imp. tech.
• Definitive impressions
• # Conventional final imp. tech.
• # Muco-compressive imp. Tech.
• # Butterfly imp. technique.
• # Dynamic & Functional imp. tech(s).
The primary impressions should accurate without excessive tissue distortion .
Primary impressions

Well-formed impression of (lower) lingual sulcus area
Deficiencies of Lower impressions in the retromolar pads and the functional forms of the floor of the mouth and the retromylohyoid fossae result in an unstable denture.

Definitive
Impressions(secondary impression)
• Alginate impression material
• ZOE• Rubber base impression material.
• By using modified acrylic resin special tray
# Conventional Impression TechniqueOpen mouth tech.
Spacing is required between the tray and the primary cast, e.g. 3 mm spacing is recommended for irreversible hydrocolloids where large undercuts are present
a. Alginate impression material
In the alginate impression, the external oblique ridge shows a groove. The impression should record the ridge. The denture border can be extended 1-2 mm beyond this ridge.

b. Metallic oxide paste (Zinc oxide eugenol impression paste + Green stick impression compound) / close fitting tray





c. Rubber base impression Technique

# Muco-compressive impression technique
Primary impression is made with impression compound using suitable stock tray .Special trays: occ. Blocks at accepted VD
Border molding of the periphery using green stick compound Final impression is made using zinc oxide and eugenol impression paste while the patient is closing on the occluding rims (closed mouth technique)


Impression Making
Muco-compressive impression technique
Final impression is made using zinc oxide and eugenol impression paste while the patient is closing on the occluding rims (closed mouth technique)
This technique is indicated in case of advanced resorbed ridge with projecting sublingual glands.
#Butterfly impression technique
Three applications of tissue conditioning material are used for making this impression
A primary impression is made cover the sublingual crescent area using alginate impression material.
An acrylic resin special tray is fabricated with a butterfly extension over the sublingual crescent area and an occlusion rim is added to simulate the height and position of the anterior and posterior teeth.
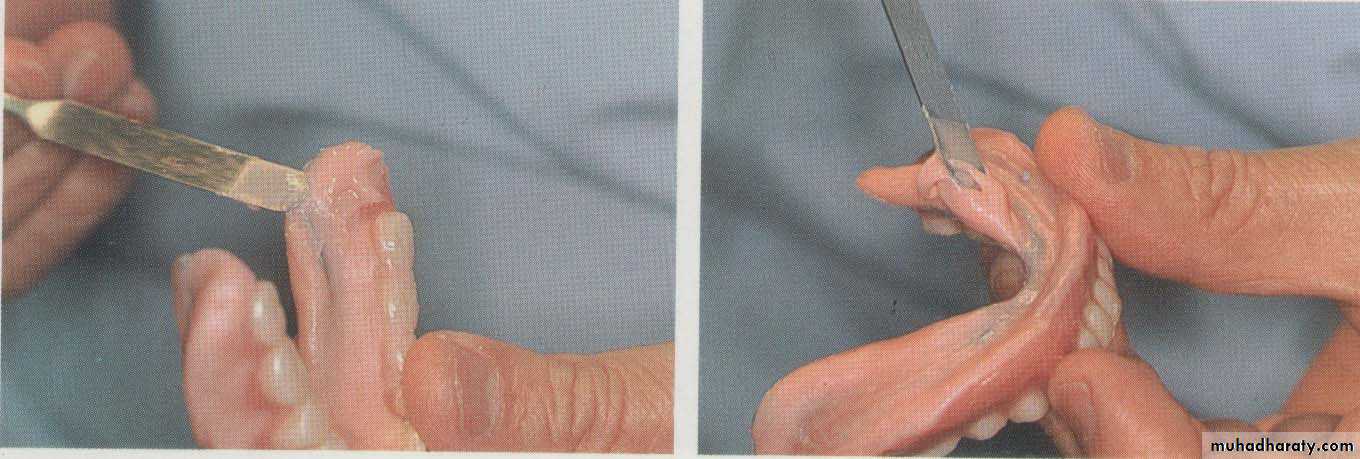
The borders are adjusted.
Three applications of the tissue conditioning material are used with closed mouth technique.
Two application of a viscous tissue conditioning material. Each application is allowed to remain in the mouth for 8-10 minutes pressure areas are corrected after each application.
Third wash is made using either a soft tissue conditioning material or a light-bodied rubber base impression material.

Final impression is made using a viscous and soft tissue conditioning material. while the patient is closing on the occluding rims (closed mouth technique)
This technique is used to record the range of muscle action as well as spaces into which the denture can be extended without displacement.
# Dynamic impression technique



Stoppers on the fitting surface
The stops must contact the upper teeth at the selected OVD.
The upper denture is set up conventionally to the prescribed occlusal vertical dimension (OVD).Opposing the upper set-up is a resin base with three vertical stops joined by a wire bent in a sinusoidal manner.
Final impression is made using a thin mix of alginate impression material.
Then, the patient is asked to close slowly until the mandibular rests firmly contact the maxillary arch and keep his tongue in contact with the tongue rest.The patient is instructed to swallow 3-4 times and forcefully protrude the lips forwards.
The resulting impression covers the maximum possible basal seat area and the borders are in harmony with the adjacent moving tissues.
# Functional impression
• Two variations are commonly used for functional impressions.• (a) Neutral Zone Impression Techniques
• (b) Local areas of modification
Indications:
It is designed for patients with poor track records of (lower) denture stability.
A large tongue or other anatomical anomaly.
a. Neutral Zone Impression Technique:
The neutral zone concept
Is based on the belief that the muscles should be functionally mold not only the borders and the artificial teeth, but also the entire polished surface.facial and lingual forces generated by the musculature of the lips, cheeks and tongue are balanced.


Technique of neutral zone impression using Viscogel material
Primary impressions of the upper and lower jaws are taken in impression compound.Upper wax rims and a lower special tray are constructed.
The special tray is a plate of acrylic without a handle, with spurs or fins projecting upwards towards the upper arch. These help with retention of the impression material.

A lower acrylic special tray with metal sprues to aid retention of the impression material
Occlusal pillars have been built up in green stick to the correct occlusal height

Establishing the correct occlusal height

The upper wax rim is adjusted as in normal registration for the compl. Denture / The lower special tray is placed in the mouth. Two occlusal pillars are then built up with self - cured acrylic on
the opposite sides of the lower arch.
These pillars are molded and adjusted to the correct height so as to give the usual 3mm freeway space.
Thick mix of viscogel is then placed around the rest of the lower special tray distally, and mesially to the occlusal pillars.

The patient is then asked to talk, swallow, drink some water …. etc.
Then• After about 5-10 minutes the set impression is removed from the mouth and examined. The viscogel material would have been
• molded by the patient's musculature into a position of balance.

Functional Neutral Zone Impression Technique / recorded in PVS putty:
Polyvinylsiloxane putty is added to the conventional fitting surface and also to the buccal and lingual aspects of the lower base which has been coated with the requisite adhesive, and placed in the patient's mouth. the upper try-in is inserted and the patient asked to close to the OVD, swallow and carry out closed mouth exercises.These exercises provide an indication of where inward-directed forces from the buccinator muscles are equaled or 'neutralized' by outwardly-directed lingual forces ie the zone of minimal conflict.

Completed functional impression of denture form - recorded in PVS putty

These enable an exact wax form to be poured to give a functional form to the polished surfaces and occlusal form of the lower denture.
Setting of the lower teeth to match with the functional template.
Plaster or laboratory-putty keys made of the functional impression to give A functional form to the polished surfaces and occlusal form of the lower denture.
A plaster index used to locate the teeth to the neutral zone.
b. Local areas of modification:Functional impression using : “chair-side resilient lining material”.

Dentures may exhibit looseness, not arising primarily from retention problems but because of localized areas of poor functional adaptation.
In these cases, the application of a thin mix of a chairside resilient lining material (eg Visco-Gel) may be used.
The mixed material is added to the fitting surface of the denture and the patient is instructed to wear the denture for one hour.
After one hour of functional moulding the denture is then removed from the mouth and the conventional relining process completed.


Jaw Relation
• Jaw relation registration is carried out using check bite technique.• Occlusal plane is adjusted nearer to the flat ridge to decrease the lever arm.
Setting up of teeth
• Cross-linked cuspless acrylic teeth are used to decrease the lateral component of force and improve denture stability.
• Decrease the occlusal table to increase the cutting efficiency, so decreast the transmitted forces.
• Setting up of teeth in the neutral zone would help to achieve denture stability.
The teeth positioned in the neutral zone leaving plenty of tongue space

The occlusal table has been reduced significantly by reducing the length and width of the posterior table.

The occlusal table proved to be a problem because the wide posterior teeth presented lingual undercuts. In addition, the length of the table, extending over the ascending portion of the ridge, adversely affected denture stability.
This is the desirable form of posterior buccal flange of a complete lower denture which restores an atrophic mandibular ridge.



Note
also
