



LOCAL & Regional FLAPS
IN HEAD &NECK RECONSTRUCTIONDr.Wafaa Khalil
Definition :
A flap is a unit of tissue that is transferred from donor site to recipient site while maintaining its own blood supply.Missing tissue most often results from either trauma or oncologic surgery. Commonly there is a wide range of options for repairing a given defect, including healing by secondary intention, primary closure, placement of a skin graft, or mobilization of local or regional tissue.
• Flaps Uses
• Replace tissue loss due to trauma or surgical excision• Provide skin coverage through which surgery can be carried on latter
• Provide padding over bony prominences
• Bring in better blood supply to poorly vascularized bed
• Improve sensation to an area (sensate flap)
• Bring in specialized tissue for reconstruction such
• as bone or functioning muscle
BASED ON LOCATION OF DONOR SITE
LOCAL FLAP: Flap transferred from an area adjacent tothe defect.
DISTANT FLAP : Flap transferred from an noncontiguous anatomic site.
REGIONAL FLAP: Flap recruited from different area of the same part of the body.
CLASSIFICATION OF LOCAL FLAPS
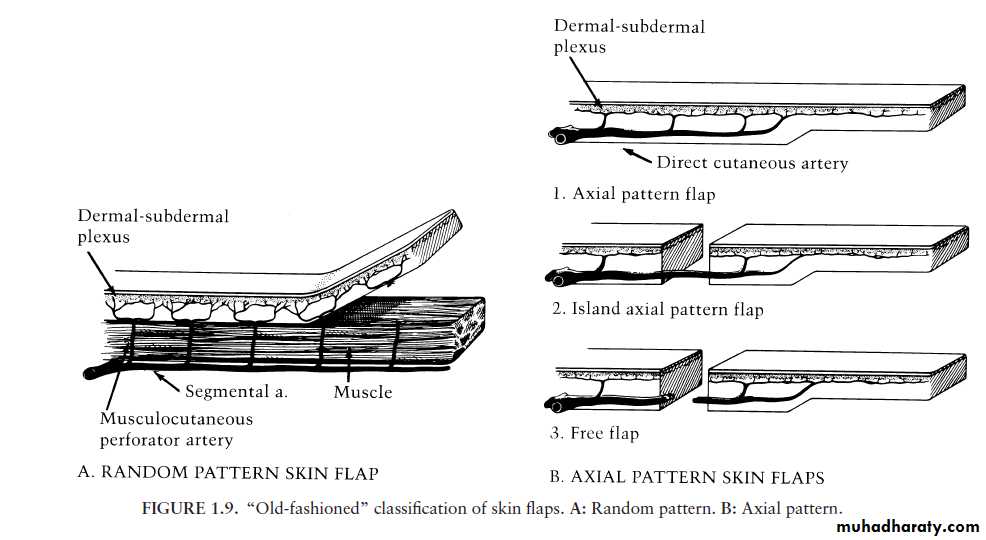
LOCAL FLAPS• Random flaps are supplied by the dermal and subdermal plexus alone
• Its the common type of flap used for reconstructing facial defects• length to width ratio of up to 2 : 1 in the face without risk of flap loss or skin necrosis.
Random flaps
Axial flaps
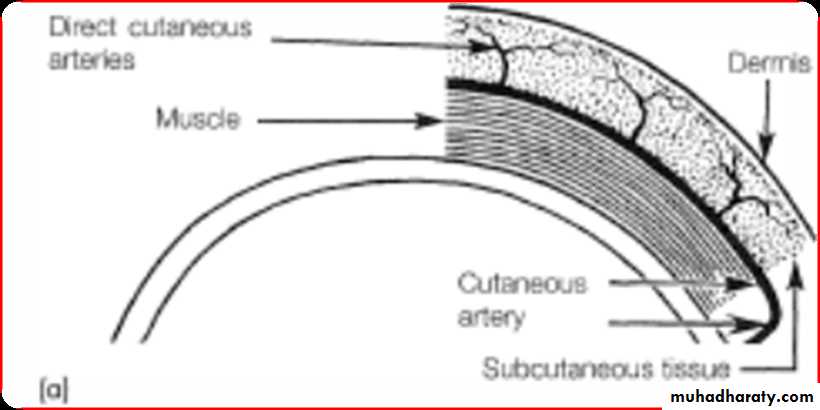
• Derive their blood supply from a direct cutaneous artery or named blood vessel .• Examples :Nasolabial flap (angular artery) , Forehead flap(supratrochlear artery).
• The surviving length of an axial pattern flap is entirely related to the length of the included artery.
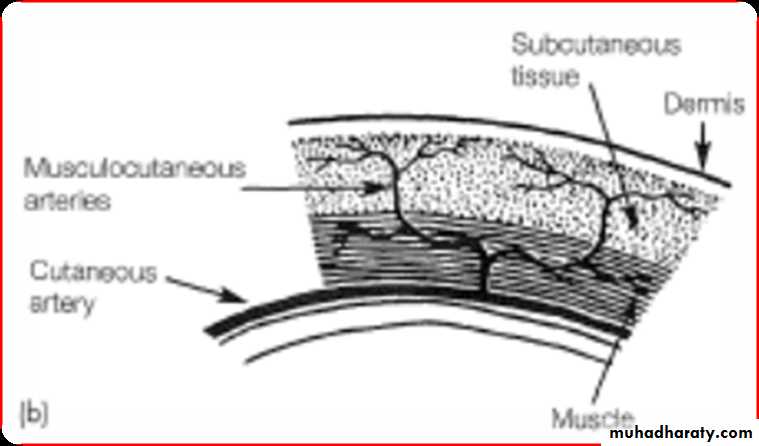
• Pedicle flaps are supplied by large named arteries that supply the skin paddle through muscular perforating vessels.
• Free flap: is a tissue harvested from a remote region and have the vascular connection which transfer and reestablished at the recipient site.
Axial flaps
LOCAL FLAPS
LOCAL FLAPS• Advantages
• Best local cosmetic tissue match
• Often a simple procedure
• Local or regional anaesthesia option
• Disadvantages
• Possible local tissue shortage• Scarring may exacerbate the condition
• Surgeon may compromise local resection
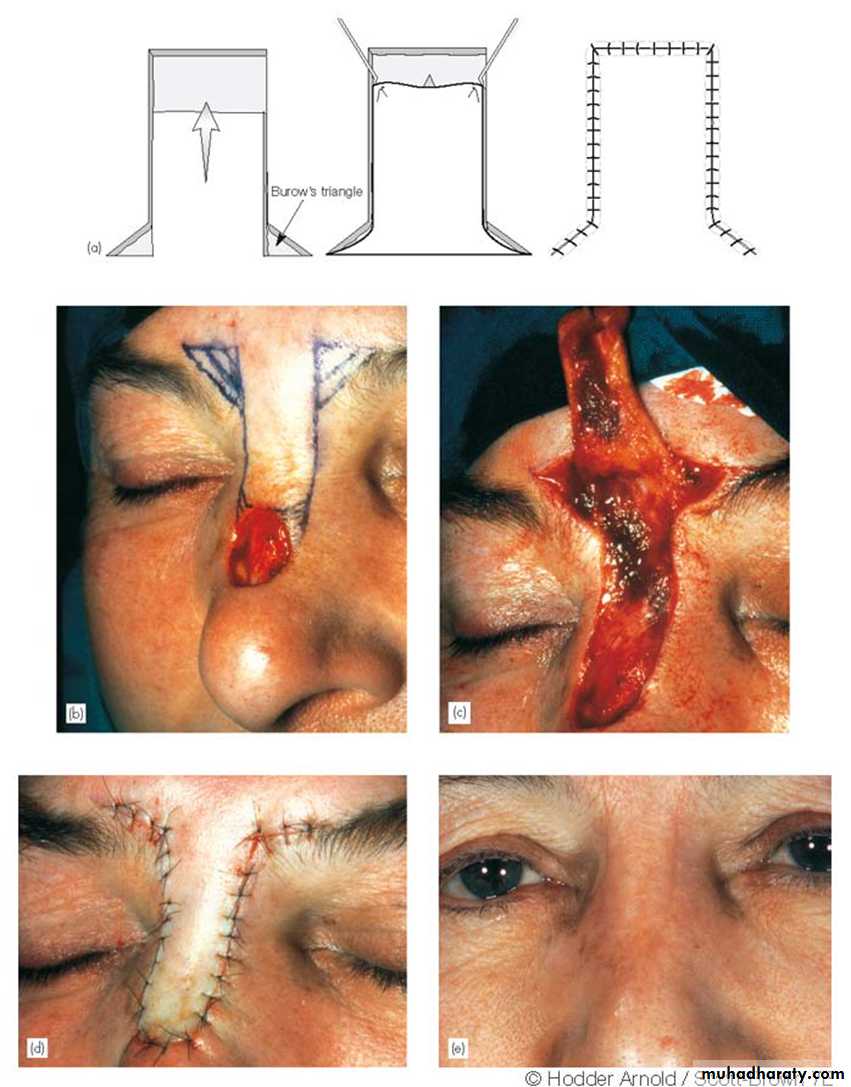
• Advancement flaps are mobilized along a linear axis without any lateral movement into the primary defect.
• (Burrows Triangle’s)
• sites – forehead, brow, cheek.
movement is entirely in one direction.
A, Advancement flap for closure of forehead defect. B, Closure of defect with incision lines placed in natural forehead crease
A

B
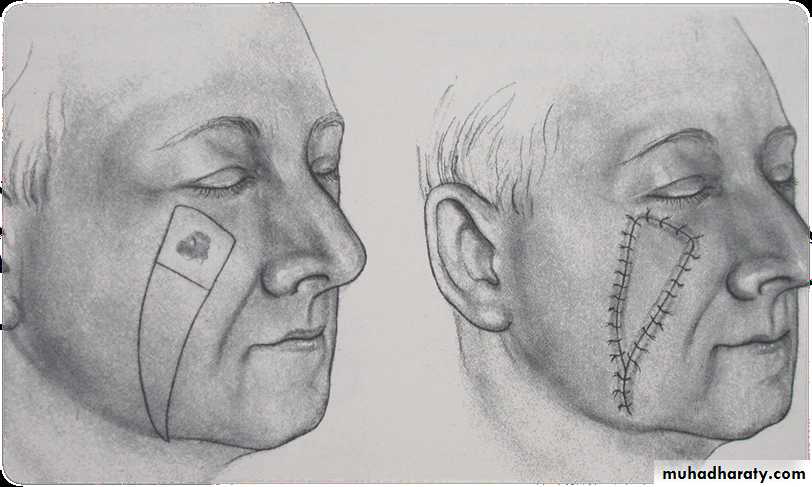
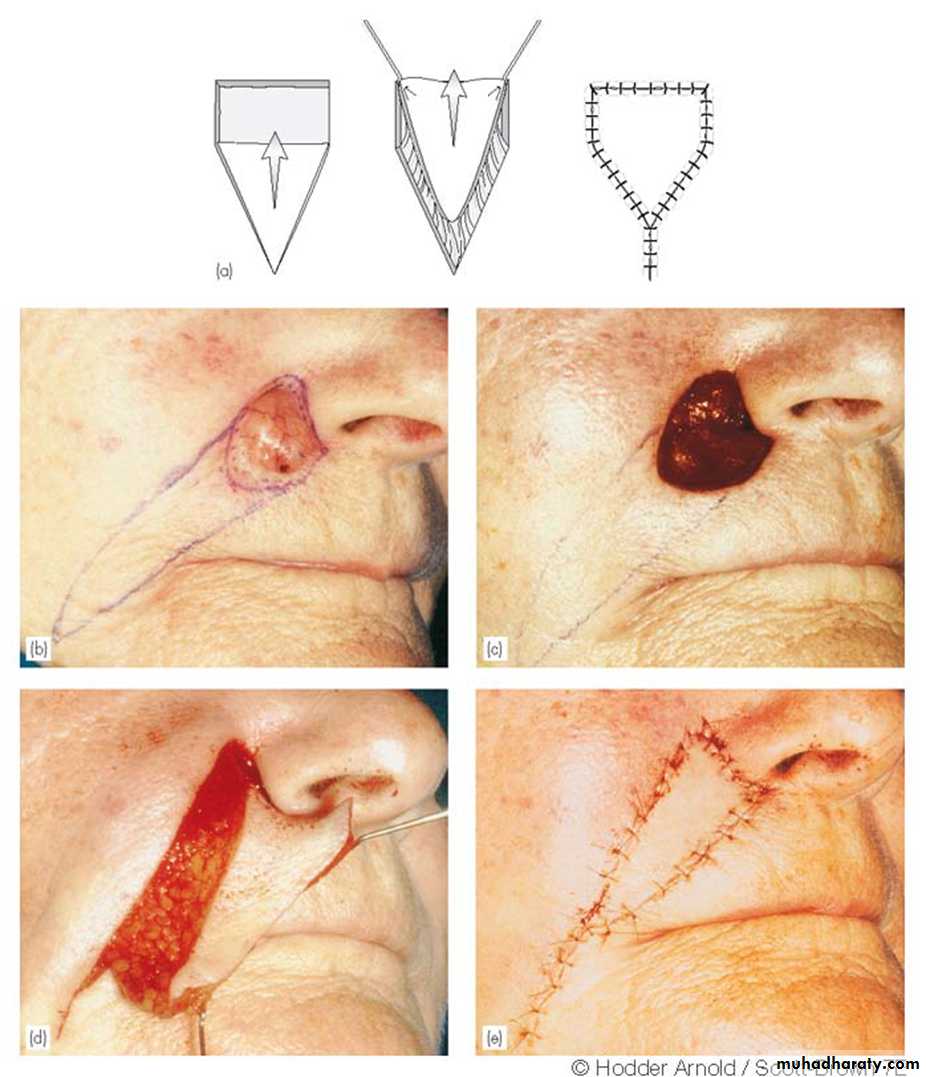
V-y advancement flap: (Herbert flap)
• A V shaped flap is moved into a defect with primary closure of the donor area leaving a final Y shaped suture line.• It is pedicled from the underlying subcutaneous tissue rather than the surrounding skin.
• Ideal for Lesion in
• the cheek
• and alar base
Rotation flaps pivot around a point at the base of the flap.
A, Axial frontonasal flap for repair of a nasal defect. B, Elevation of the flap with thorough undermining. C, Closure of the defectA
B
C
Interpolated flaps are those flaps that are mobilize either over or beneath a complete bridge of intact skin via a pedicle.
A, Outline for a rhombic flap. B, Resection of the lesion. C, The flap is transposed into the defect. D, Postoperative result with the incisions placed in the relaxed skin tension lines
B
A
D

C
Transpotion flap

A, Nasal defect after excision of squamous cell carcinoma lesion. B, Use of Doppler ultrasonography to locate the supratrochlear artery. C, The forehead flap has been elevated. D, The flap is turned 180° and sutured into place. E, The pedicle is divided 2 to 3 weeks later. F, Postoperative result
A
B
CC
F
E
D
Interpolated flaps
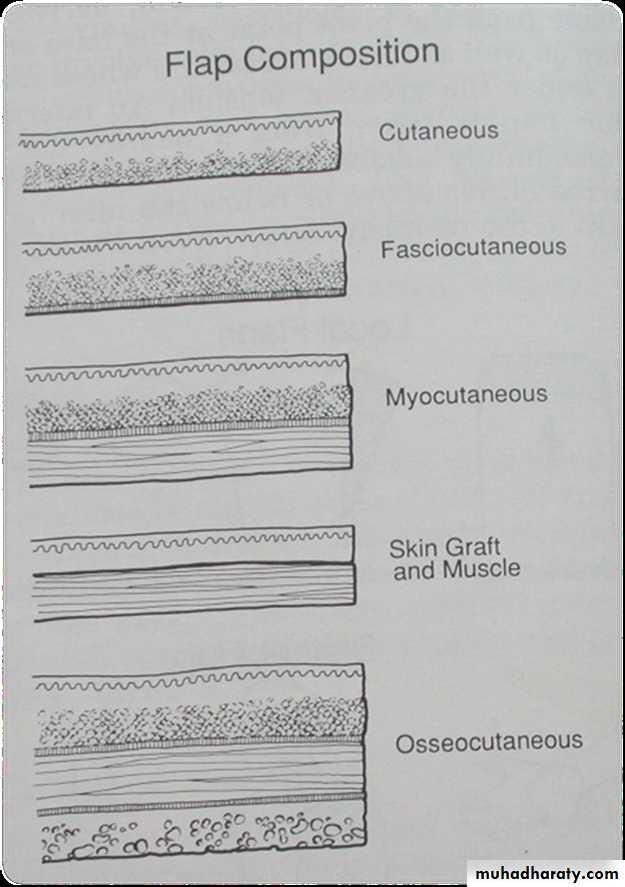
Local flap based on composition
• Skin (cutaneous)• Visceral ( colon, omentum)
• Muscle
• Mucosal
• Composite
• Fasciocutaneous
• Myocutaneous
• Osseocutaneous
• Tendocutaneous
• Sensory/innervated flaps
• Osseo-myo-cutaneous
Local / Regional flaps – Goals (Kinnerw & Jeter)
• 1. Adequate color match
• 2. Adequate thickness – avoid protrusions or deficiencies
• 3. Preservation of clinically perceivable sensory innervation
• 4. Sufficient laxity – avoid retraction or deranged function
• 5. Resultant suture lines of either primary or secondary defects are restricted to anatomic units and fall within natural skin lines.
• REGIONAL FLAPS
• Defined as those flaps that are located near a defect but are not in the immediate proximity.• They are frequently harvested from the neck, chest, or axilla.
• Classified as axial, however most flaps have random pattern at their distal ends
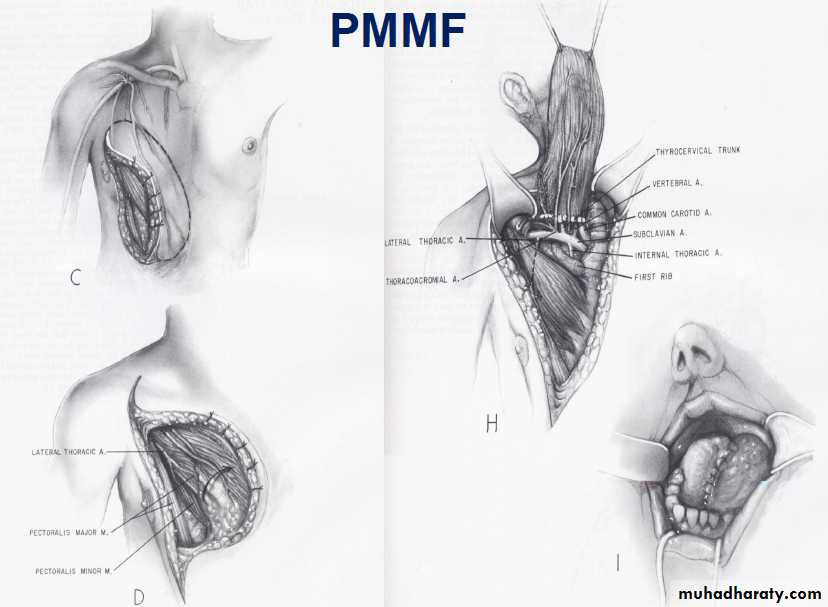
• Utilized to cover large defects which require bulk
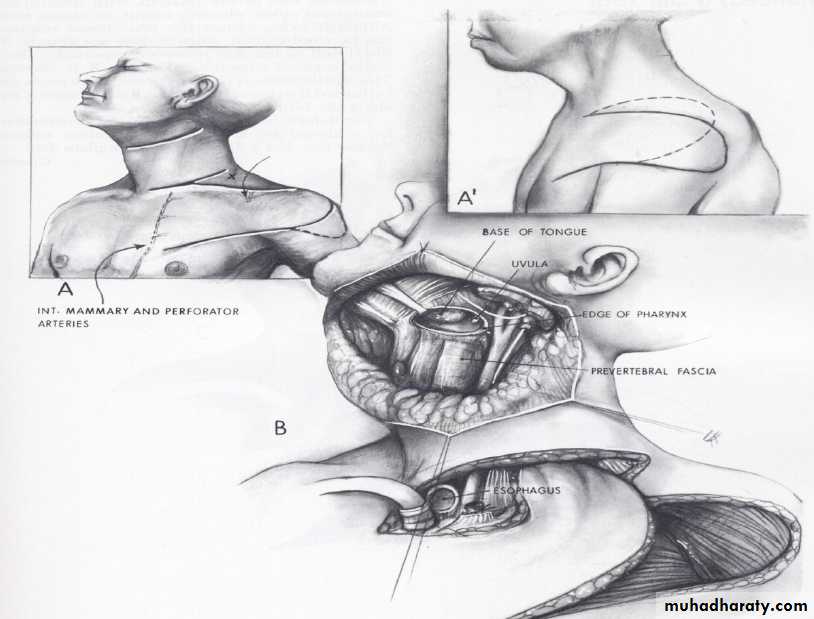
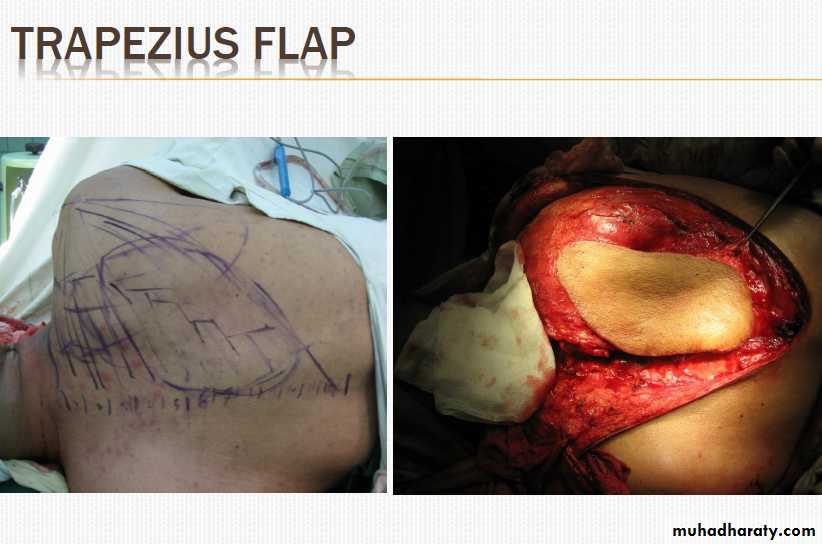
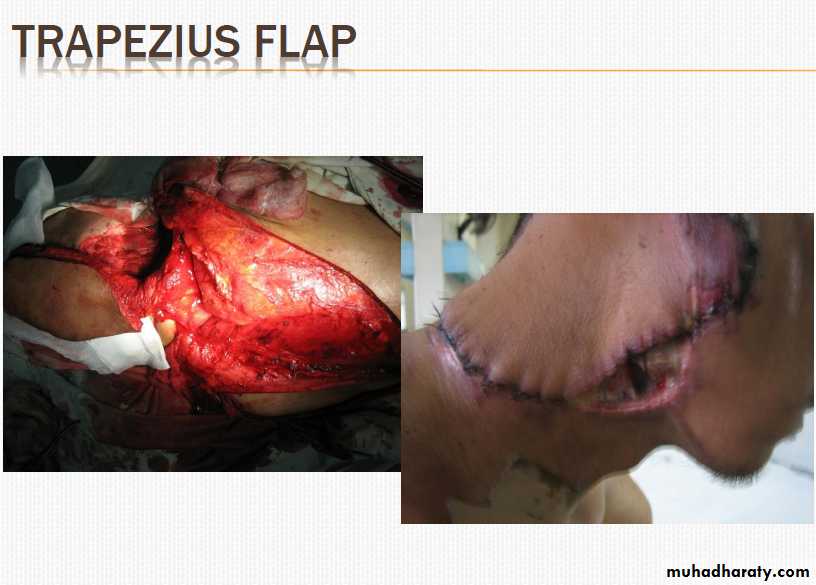
• Examples : 1. PMMF (Pectoralis Major Myocutaneous flap) 2. DPF (deltopectoral flap) 3. Trapezius flap
REGIONAL FLAPS
Advantages of regional flaps• large amount of soft tissue and skin available.
Disadvantages of regional flaps
• poor color and texture match
• excessive bulkiness of the flap
• donor site morbidity.
Deltopectoral Flap
Postoperative Care
• Pain reliever• Wound care
• antibiotic ointment
• Sutures removed at 5-7 days
• Revision if required - 6 months
Complications
• Infection
• Dehiscence
• Vascular insufficiency due to
• Mechanical tension
• Kinking
• compression
• Hematoma/seroma
• Failure/necrosis
• Causes of flap failure
• poor anatomical knowledge when raising the flap (such that the blood supply is deficient from the start)• flap inset with too much tension
• local sepsis or a septicaemic patient
• the dressing applied too tightly around the pedicle;